Source: European Medicines Agency (EU) Revision Year: 2019 Publisher: CSL Behring GmbH, Emil-von-Behring-Strasse 76, D-35041, Marburg, Germany
Pharmacotherapeutic group: Antihemorrhagics, proteinase inhibitor
ATC code: B02AB02
Human alpha1-proteinase inhibitor is a normal constituent of human blood. Human alpha1-proteinase inhibitor has a molecular weight of 51 kDa and belongs to the family of serine protease inhibitors.
Human alpha1-proteinase inhibitor is understood to be the primary anti-protease in the lower respiratory tract, where it inhibits neutrophil elastase (NE). Normal healthy individuals produce sufficient alpha1-proteinase inhibitor to control the NE produced by activated neutrophils and are thus able to prevent inappropriate proteolysis of lung tissue by NE. Conditions that increase neutrophil accumulation and activation in the lung, such as respiratory infection and smoking, will in turn increase levels of NE. However, individuals deficient in endogenous alpha1-proteinase inhibitor are unable to maintain appropriate antiprotease defence and experience more rapid proteolysis of the alveolar walls starting prior to the development of clinically evident chronic obstructive lung disease in the third or fourth decade.
The administration of Respreeza increases and maintains serum levels and lung epithelial lining fluid (ELF) levels of alpha1-proteinase inhibitor leading to a slowdown of the progression of emphysema.
The safety and efficacy of Respreeza was evaluated in a randomized, double-blind, placebocontrolled, multi-center study (RAPID) followed by a 2-year open-label extension study (RAPID extension study). A total of 180 subjects with alpha1-proteinase inhibitor deficiency characterized by a serum alpha1-proteinase inhibitor level <11 μM (i.e. <50 mg/dL as determined by nephelometry) and clinical evidence of emphysema, were randomized to receive a weekly 60 mg/kg bw intravenous dose of either Respreeza (93 subjects) or placebo (87 subjects) for up to 24 months. The subjects ranged in age from 31 to 67 years (median age 54 years) with average baseline alpha1-proteinase inhibitor levels of approximately 6.15 µM, and average volume-adjusted CT lung density of 47 g/L / 50 g/L for Respreeza and placebo subjects, respectively. One-hundred forty subjects (76 Respreeza-treated subjects and 64 subjects treated with placebo in the RAPID Study) continued into the RAPID extension study and were treated with a weekly 60 mg/kg bw intravenous dose of Respreeza for up to 24 months.
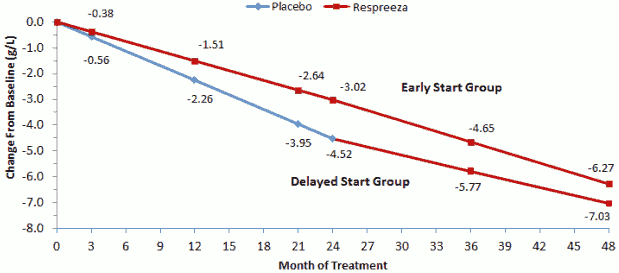
The studies investigated the effect of Respreeza on the progression of emphysema, assessed by the decline of lung density, measured by computer tomography (CT). Respreeza-treated subjects demonstrated a consistent pattern of slower lung density decline than those receiving placebo (see Figure 1). The annual rate of lung density decline, as measured by CT scan at total lung capacity (TLC) over 2 years was lower with Respreeza (-1.45 g/L) as compared with placebo (-2.19 g/L), reflecting a 34% reduction (p=0.017, 1-sided).
The RAPID extension study demonstrated that the reduced rate in lung density decline was maintained for subjects continuously treated with Respreeza for 4 years (see Figure 1).
Figure 1. Changes in Lung Density (TLC) from baseline in the RAPID and RAPID Extension studies:
Single doses of 120 mg/kg bw have been administered to 137 subjects treated with Respreeza.
The European Medicines Agency has waived the obligation to submit the results of studies with Respreeza in all subsets of the pediatric population in chronic obstructive pulmonary disease (COPD) due to alpha1-proteinase inhibitor deficiency (see section 4.2 for information on pediatric use).
Four clinical studies were conducted with Respreeza in 89 subjects (59 males and 30 females) to evaluate the effect of Respreeza on serum levels of alpha1-proteinase inhibitor. The subjects ranged in age from 29 to 68 years (median age 49 years). At screening, serum alpha1-proteinase inhibitor levels were between 3.2 and 10.1 µM (mean of 5.6 µM).
A double-blind, randomized, active-controlled, crossover pharmacokinetic study was conducted in 13 males and 5 females with alpha1-proteinase inhibitor deficiency, ranging in age from 36 to 66 years. Nine subjects received a single 60 mg/kg bw dose of Respreeza followed by a comparator product, and 9 subjects received comparator product followed by a single 60 mg/kg bw dose of Respreeza, with a wash-out period of 35 days between doses. A total of 13 post-infusion serum samples were taken at various time points up to Day 21. Table 1 shows the mean results for the Respreeza pharmacokinetic parameters.
Table 1. Pharmacokinetic parameters for alpha1-proteinase inhibitor following a single 60 mg/kg bw dose of Respreeza:
| Pharmacokinetic Parameter | Mean (standard deviation)* |
|---|---|
| Area under the curve (AUC0-∞) | 144 (±27) µM x day |
| Maximum concentration (Cmax) | 44.1 (±10.8) µM |
| Terminal half-life (t1/2ß) | 5.1 (±2.4) days |
| Total clearance | 603 (±129) mL/day |
| Volume of distribution at steady state | 3.8 (±1.3) L |
* n=18 subjects.
A population pharmacokinetic analysis was conducted using data from 90 Respreeza-treated subjects from the RAPID trial. The population estimate of mean half-life was 6.8 days. The model predicted mean steady-state concentration was 21.8 µM after a 60 mg/kg bw/week dose. The population pharmacokinetic analysis did not indicate that there were any significant effects of age, gender, weight, or baseline serum antigenic alpha1-proteinase inhibitor concentrations on the clearance of Respreeza.
In a double-blind, controlled clinical study to evaluate the safety and biochemical efficacy of Respreeza 44 subjects were randomized to receive 60 mg/kg bw intravenous dose of Respreeza once weekly for 24 weeks. The mean trough serum alpha1-proteinase inhibitor levels at steady state (Weeks 7-11) were maintained above 11 µM. The mean (Standard Deviation) of the steady state trough serum alpha1-proteinase inhibitor level for Respreeza-treated subjects was 17.7 µM (2.5). In a subgroup of subjects enrolled in this study (10 Respreeza-treated subjects) broncho-alveolar lavage was performed. Epithelial lining fluid measurements (ELF) of alpha1-proteinase inhibitor levels showed a consistent increase following treatment. ELF levels of antigenic alpha1-proteinase inhibitor and alpha1-proteinase inhibitor: NE complexes increased from baseline. Free elastase was immeasurably low in all samples.
Following the completion of the RAPID study, an analysis of achieved median alpha1-proteinase inhibitor levels and lung density decline was conducted. This analysis revealed an inverse linear relationship between trough serum alpha1-proteinase inhibitor levels and the annual decline in lung density as measured by volume adjusted CT scans for subjects receiving 60 mg/kg bw intravenous dose of Respreeza.
The safety of Respreeza has been assessed in several preclinical studies. Non-clinical data reveal no special risk for humans based on safety pharmacology and short term toxicity studies. Repeat dose toxicity studies longer than 5 days, reproductive toxicity studies and carcinogenicity studies, have not been performed. Such studies are not considered meaningful due to the production of antibodies against the heterologous human protein in animals. Since human alpha1-proteinase inhibitor is a protein and a physiological constituent of human blood, it is not expected to present carcinogenic, genotoxic, or teratogenic effects.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.