Source: European Medicines Agency (EU) Revision Year: 2018 Publisher: GlaxoSmithKline (Ireland) Limited, 12 Riverwalk, Citywest Business Campus, Dublin 24, Ireland
Pharmacotherapeutic group: Anti-hypertensives, other anti-hypertensives
ATC code: C02KX02
Ambrisentan is an orally active, propanoic acid-class, ERA selective for the endothelin A (ETA) receptor. Endothelin plays a significant role in the pathophysiology of PAH.
Two randomised, double-blind, multi-centre, placebo controlled, Phase 3 pivotal studies were conducted (ARIES-1 and 2). ARIES-1 included 201 patients and compared ambrisentan 5 mg and 10 mg with placebo. ARIES-2 included 192 patients and compared ambrisentan 2.5 mg and 5 mg with placebo. In both studies, ambrisentan was added to patients' supportive/background medication, which could have included a combination of digoxin, anticoagulants, diuretics, oxygen and vasodilators (calcium channel blockers, ACE inhibitors). Patients enrolled had IPAH or PAH associated with connective tissue disease (PAH-CTD). The majority of patients had WHO functional Class II (38.4%) or Class III (55.0%) symptoms. Patients with pre-existent hepatic disease (cirrhosis or clinically significantly elevated aminotransferases) and patients using other targeted therapy for PAH (e.g. prostanoids) were excluded. Haemodynamic parameters were not assessed in these studies.
The primary endpoint defined for the Phase 3 studies was improvement in exercise capacity assessed by change from baseline in 6 minute walk distance (6MWD) at 12 weeks. In both studies, treatment with ambrisentan resulted in a significant improvement in 6MWD for each dose of ambrisentan.
The placebo-adjusted improvement in mean 6MWD at week 12 compared to baseline was 30.6 m (95% CI: 2.9 to 58.3; p=0.008) and 59.4 m (95% CI: 29.6 to 89.3; p<0.001) for the 5 mg group, in ARIES 1 and 2 respectively. The placebo-adjusted improvement in mean 6MWD at week 12 in patients in the 10 mg group in ARIES-1 was 51.4 m (95% CI: 26.6 to 76.2; p<0.001).
A pre-specified combined analysis of the Phase 3 studies (ARIES-C) was conducted. The placeboadjusted mean improvement in 6MWD was 44.6 m (95% CI: 24.3 to 64.9; p<0.001) for the 5 mg dose, and 52.5 m (95% CI: 28.8 to 76.2; p<0.001) for the 10 mg dose.
In ARIES-2, ambrisentan (combined dose group) significantly delayed the time to clinical worsening of PAH compared to placebo (p<0.001), the hazard ratio demonstrated an 80% reduction (95% CI: 47% to 92%). The measure included: death, lung transplantation, hospitalisation for PAH, atrial septostomy, addition of other PAH therapeutic agents and early escape criteria. A statistically significant increase (3.41 ± 6.96) was observed for the combined dose group in the physical functioning scale of the SF-36 Health Survey compared with placebo (-0.20 ± 8.14, p=0.005). Treatment with ambrisentan led to a statistically significant improvement in Borg Dyspnea Index (BDI) at week 12 (placebo-adjusted BDI of -1.1 (95% CI: -1.8 to -0.4; p=0.019; combined dose group)).
Patients enrolled into ARIES-1 and 2 were eligible to enter a long term open label extension study ARIES-E (n=383). The combined mean exposure was approximately 145 ± 80 weeks, and the maximum exposure was approximately 295 weeks. The main primary endpoints of this study were the incidence and severity of adverse events associated with long-term exposure to ambrisentan, including serum LFTs. The safety findings observed with long-term ambrisentan exposure in this study were generally consistent with those observed in the 12 week placebo-controlled studies.
The observed probability of survival for subjects receiving ambrisentan (combined ambrisentan dose group) at 1, 2 and 3 years was 93%, 85% and 79% respectively.
In an open label study (AMB222), ambrisentan was studied in 36 patients to evaluate the incidence of increased serum aminotransferase concentrations in patients who had previously discontinued other ERA therapy due to aminotransferase abnormalities. During a mean of 53 weeks of treatment with ambrisentan, none of the patients enrolled had a confirmed serum ALT >3xULN that required permanent discontinuation of treatment. Fifty percent of patients had increased from 5 mg to 10 mg ambrisentan during this time.
The cumulative incidence of serum aminotransferase abnormalities >3xULN in all Phase 2 and 3 studies (including respective open label extensions) was 17 of 483 subjects over a mean exposure duration of 79.5 weeks. This is an event rate of 2.3 events per 100 patient years of exposure for ambrisentan. In the ARIES-E open label long term extension study, the 2 year risk of developing serum aminotransferase elevations >3xULN in patients treated with ambrisentan was 3.9%.
An improvement in haemodynamic parameters was observed in patients with PAH after 12 weeks (n=29) in a Phase 2 study (AMB220). Treatment with ambrisentan resulted in an increase in mean cardiac index, a decrease in mean pulmonary artery pressure, and a decrease in mean pulmonary vascular resistance.
Decrease in systolic and diastolic blood pressures has been reported with ambrisentan therapy. In placebo controlled clinical trials of 12 weeks duration mean reduction in systolic and diastolic blood pressures from base line to end of treatment were 3mm Hg and 4.2 mm Hg respectively. The mean decreases in systolic and diastolic blood pressures persisted for up to 4 years of treatment with ambrisentan in the long term open label ARIES E study.
No clinically meaningful effects on the pharmacokinetics of ambrisentan or sildenafil were seen during a drug-drug interaction study in healthy volunteers, and the combination was well tolerated. The number of patients who received concomitant ambrisentan and sildenafil in ARIES-E and AMB222 was 22 patients (5.7%) and 17 patients (47%), respectively. No additional safety concerns were identified in these patients.
A multicenter, double-blind, active comparator, event-driven, Phase 3 outcome study (AMB112565/AMBITION) was conducted to assess the efficacy of initial combination of ambrisentan and tadalafil vs. monotherapy of either ambrisentan or tadalafil alone, in 500 treatment naive PAH patients, randomised 2:1:1, respectively. No patients received placebo alone. The primary analysis was combination group vs. pooled monotherapy groups. Supportive comparisons of combination therapy group vs. the individual monotherapy groups were also made. Patients with significant anaemia, fluid retention or rare retinal diseases were excluded according to the investigators' criteria. Patients with ALT and AST values >2xULN at baseline were also excluded.
At baseline, 96% of patients were naive to any previous PAH-specific treatment, and the median time from diagnosis to entry into the study was 22 days. Patients started on ambrisentan 5 mg and tadalafil 20 mg, and were titrated to 40 mg tadalafil at week 4 and 10 mg ambrisentan at week 8, unless there were tolerability issues. The median double-blind treatment duration for combination therapy was greater than 1.5 years.
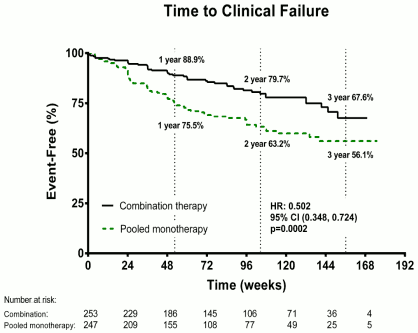
The primary endpoint was the time to first occurrence of a clinical failure event, defined as:
The mean age of all patients was 54 years (SD 15; range 18–75 years of age). Patients WHO FC at baseline was II (31%) and FC III (69%). Idiopathic or heritable PAH was the most common aetiology in the study population (56%), followed by PAH due to connective tissue disorders (37%), PAH associated with drugs and toxins (3%), corrected simple congenital heart disease (2%), and HIV (2%). Patients with WHO FC II and III had a mean baseline 6MWD of 353 metres.
Treatment with combination therapy resulted in a 50% risk reduction (hazard ratio [HR] 0.502; 95% CI: 0.348 to 0.724; p=0.0002) of the composite clinical failure endpoint up to final assessment visit when compared to the pooled monotherapy group [Figure 1 and Table 1]. The treatment effect was driven by a 63% reduction in hospitalisations on combination therapy, was established early and was sustained. Efficacy of combination therapy on the primary endpoint was consistent on the comparison to individual monotherapy and across the subgroups of age, ethnic origin, geographical region, aetiology (iPAH /hPAH and PAH-CTD). The effect was significant for both FC II and FC III patients.
Figure 1:
Table 1:
| Ambrisentan + Tadalafil (N=253) | Monotherapy Pooled (N=247) | Ambrisentan monotherapy (N=126) | Tadalafil monotherapy (N=121) | |
|---|---|---|---|---|
| Time to First Clinical Failure Event (Adjudicated) | ||||
| Clinical failure, no. (%) | 46 (18%) | 77 (31%) | 43 (34) | 34 (28) |
| Hazard ratio (95% CI) | 0,502 (0,348, 0,724) | 0,477 (0,314, 0,723) | 0,528 (0,338, 0,827) | |
| P-value, Log-rank test | 0,0002 | 0,0004 | 0,0045 | |
| Component as First Clinical Failure Event (Adjudicated) | ||||
| Death (all-cause) | 9 (4%) | 8 (3%) | 2 (2) | 6 (5) |
| Hospitalisation for worsening PAH | 10 (4%) | 30 (12%) | 18 (14) | 12 (10) |
| Disease progression | 10 (4%) | 16 (6%) | 12 (10) | 4 (3) |
| Unsatisfactory long-term clinical response | 17 (7%) | 23 (9%) | 11 (9) | 12 (10) |
| Time to First Hospitalisation for Worsening PAH (Adjudicated) | ||||
| First hospitalisation, no. (%) | 19 (8%) | 44 (18%) | 27 (21%) | 17 (14%) |
| Hazard ratio (95% CI) | 0,372 | 0,323 | 0,442 | |
| P-value, Log-rank test | 0,0002 | <0,0001 | 0,0124 | |
Secondary endpoints were tested:
Table 2:
| Secondary Endpoints (change from baseline to week 24) | Ambrisentan + Tadalafil | Monotherapy pooled | Difference and Confidence Interval | p value |
|---|---|---|---|---|
| NT-proBNP (% reduction) | -67,2 | -50,4 | % difference -33,8, 95% CI: -44,8, -20,7 | p<0,0001 |
| % subjects achieving a satisfactory clinical response at week 24 | 39 | 29 | Odds ratio 1,56, 95% CI: 1,05, 2,32 | p=0,026 |
| 6MWD (metres, median change) | 49,0 | 23,8 | 22,75 m, 95% CI: 12,00, 33,50 | p<0,0001 |
A study of 492 patients (ambrisentan N=329, placebo N=163) with idiopathic pulmonary fibrosis (IPF), 11% of which had secondary pulmonary hypertension (WHO group 3), has been conducted, but was terminated early when it was determined that the primary efficacy endpoint could not be met (ARTEMIS-IPF study). Ninety events (27%) of IPF progression (including respiratory hospitalisations) or death were observed in the ambrisentan group compared to 28 events (17%) in the placebo group. Ambrisentan is therefore contraindicated for patients with IPF with or without secondary pulmonary hypertension (see section 4.3).
Ambrisentan is absorbed rapidly in humans. After oral administration, maximum plasma concentrations (Cmax) of ambrisentan typically occur around 1.5 hours post-dose under both fasted and fed conditions. Cmax and area under the plasma concentration-time curve (AUC) increase dose proportionally over the therapeutic dose range. Steady-state is generally achieved following 4 days of repeat dosing.
A food-effect study involving administration of ambrisentan to healthy volunteers under fasting conditions and with a high-fat meal indicated that the Cmax was decreased 12% while the AUC remained unchanged. This decrease in peak concentration is not clinically significant, and therefore ambrisentan can be taken with or without food.
Ambrisentan is highly plasma protein bound. The in vitro plasma protein binding of ambrisentan was, on average, 98.8% and independent of concentration over the range of 0.2–20 microgram/ml. Ambrisentan is primarily bound to albumin (96.5%) and to a lesser extent to alpha1-acid glycoprotein.
The distribution of ambrisentan into red blood cells is low, with a mean blood:plasma ratio of 0.57 and 0.61 in males and females, respectively.
Ambrisentan is a non-sulphonamide (propanoic acid) ERA.
Ambrisentan is glucuronidated via several UGT isoenzymes (UGT1A9S, UGT2B7S and UGT1A3S) to form ambrisentan glucuronide (13%). Ambrisentan also undergoes oxidative metabolism mainly by CYP3A4 and to a lesser extent by CYP3A5 and CYP2C19 to form 4-hydroxymethyl ambrisentan (21%) which is further glucuronidated to 4-hydroxymethyl ambrisentan glucuronide (5%). The binding affinity of 4-hydroxymethyl ambrisentan for the human endothelin receptor is 65-fold less than ambrisentan. Therefore at concentrations observed in the plasma (approximately 4% relative to parent ambrisentan), 4-hydroxymethyl ambrisentan is not expected to contribute to pharmacological activity of ambrisentan.
In vitro data indicate that ambrisentan at 300 μM resulted in less than 50% inhibition of UGT1A1, UGT1A6, UGT1A9, UGT2B7 (up to 30%) or of cytochrome P450 enzymes 1A2, 2A6, 2B6, 2C8, 2C9, 2C19, 2D6, 2E1 and 3A4 (up to 25%). In vitro, ambrisentan has no inhibitory effect on human transporters at clinically relevant concentrations, including Pgp, BCRP, MRP2, BSEP, OATP1B1, OATP1B3 and NTCP. Furthermore, ambrisentan did not induce MRP2, Pgp or BSEP protein expression in rat hepatocytes. Taken together, the in vitro data suggest ambrisentan at clinically relevant concentrations (plasma Cmax up to 3.2 μM) would not be expected to have an effect on UGT1A1, UGT1A6, UGT1A9, UGT2B7 or cytochrome P450 enzymes 1A2, 2A6, 2B6, 2C8, 2C9, 2C19, 2D6, 2E1, 3A4 or transport via BSEP, BCRP, Pgp, MRP2, OATP1B1/3, or NTCP.
The effects of steady-state ambrisentan (10 mg once daily) on the pharmacokinetics and pharmacodynamics of a single dose of warfarin (25 mg), as measured by PT and INR, were investigated in 20 healthy volunteers. Ambrisentan did not have any clinically relevant effects on the pharmacokinetics or pharmacodynamics of warfarin. Similarly, co-administration with warfarin did not affect the pharmacokinetics of ambrisentan (see section 4.5).
The effect of 7-day dosing of sildenafil (20 mg three times daily) on the pharmacokinetics of a single dose of ambrisentan, and the effects of 7-day dosing of ambrisentan (10 mg once daily) on the pharmacokinetics of a single dose of sildenafil were investigated in 19 healthy volunteers. With the exception of a 13% increase in sildenafil Cmax following co-administration with ambrisentan, there were no other changes in the pharmacokinetic parameters of sildenafil, N-desmethyl-sildenafil and ambrisentan. This slight increase in sildenafil Cmax is not considered clinically relevant (see section 4.5).
The effects of steady-state ambrisentan (10 mg once daily) on the pharmacokinetics of a single dose of tadalafil, and the effects of steady-state tadalafil (40 mg once daily) on the pharmacokinetics of a single dose of ambrisentan were studied in 23 healthy volunteers. Ambrisentan did not have any clinically relevant effects on the pharmacokinetics of tadalafil. Similarly, co-administration with tadalafil did not affect the pharmacokinetics of ambrisentan (see section 4.5).
The effects of repeat dosing of ketoconazole (400 mg once daily) on the pharmacokinetics of a single dose of 10 mg ambrisentan were investigated in 16 healthy volunteers. Exposures of ambrisentan as measured by AUC(0-inf) and Cmax were increased by 35% and 20%, respectively. This change in exposure is unlikely to be of any clinical relevance and therefore ambrisentan may be co-administered with ketoconazole.
The effects of repeat dosing of cyclosporine A (100–150 mg twice daily) on the steady-state pharmacokinetics of ambrisentan (5 mg once daily), and the effects of repeat dosing of ambrisentan (5 mg once daily) on the steady-state pharmacokinetics of cyclosporine A (100–150 mg twice daily) were studied in healthy volunteers. The Cmax and AUC(0-τ) of ambrisentan increased (48% and 121%, respectively) in the presence of multiple doses of cyclosporine A. Based on these changes, the dose of ambrisentan should be limited to 5 mg once daily when co-administered with cyclosporine A (see section 4.2). However, multiple doses of ambrisentan had no clinically relevant effect on cyclosporine A exposure, and no dose adjustment of cyclosporine A is warranted.
The effects of acute and repeat dosing of rifampicin (600 mg once daily) on the steady-state pharmacokinetics of ambrisentan (10 mg once daily) were studied in healthy volunteers. Following initial doses of rifampicin, a transient increase in ambrisentan AUC(0–τ) (121% and 116% after first and second doses of rifampicin, respectively) was observed, presumably due to a rifampicin-mediated OATP inhibition. However, there was no clinically relevant effect on ambrisentan exposure by day 8, following administration of multiple doses of rifampicin. Patients on ambrisentan therapy should be closely monitored when starting treatment with rifampicin (see sections 4.4 and 4.5).
The effects of repeat dosing of ambrisentan (10 mg) on the pharmacokinetics of single dose digoxin were studied in 15 healthy volunteers. Multiple doses of ambrisentan resulted in slight increases in digoxin AUC0-last and trough concentrations, and a 29% increase in digoxin Cmax. The increase in digoxin exposure observed in the presence of multiple doses of ambrisentan was not considered clinically relevant, and no dose adjustment of digoxin is warranted (see section 4.5).
The effects of 12 days dosing with ambrisentan (10 mg once daily) on the pharmacokinetics of a single dose of oral contraceptive containing ethinyl estradiol (35 μg) and norethindrone (1 mg) were studied in healthy female volunteers. The Cmax and AUC(0–∞) were slightly decreased for ethinyl estradiol (8% and 4%, respectively), and slightly increased for norethindrone (13% and 14%, respectively). These changes in exposure to ethinyl estradiol or norethindrone were small and are unlikely to be clinically significant (see section 4.5).
Elimination
Ambrisentan and its metabolites are eliminated primarily in the bile following hepatic and/or extrahepatic metabolism. Approximately 22% of the administered dose is recovered in the urine following oral administration with 3.3% being unchanged ambrisentan. Plasma elimination half-life in humans ranges from 13.6 to 16.5 hours.
Special populations
Based on the results of a population pharmacokinetic analysis in healthy volunteers and patients with PAH, the pharmacokinetics of ambrisentan were not significantly influenced by gender or age (see section 4.2).
Renal impairment
Ambrisentan does not undergo significant renal metabolism or renal clearance (excretion). In a population pharmacokinetic analysis, creatinine clearance was found to be a statistically significant covariate affecting the oral clearance of ambrisentan. The magnitude of the decrease in oral clearance is modest (20-40%) in patients with moderate renal impairment and therefore is unlikely to be of any clinical relevance. However, caution should be used in patients with severe renal impairment (see section 4.2).
Hepatic impairment
The main routes of metabolism of ambrisentan are glucuronidation and oxidation with subsequent elimination in the bile and therefore hepatic impairment might be expected to increase exposure (Cmax and AUC) of ambrisentan. In a population pharmacokinetic analysis, the oral clearance was shown to be decreased as a function of increasing bilirubin levels. However, the magnitude of effect of bilirubin is modest (compared to the typical patient with a bilirubin of 0.6 mg/dl, a patient with an elevated bilirubin of 4.5 mg/dl would have approximately 30% lower oral clearance of ambrisentan). The pharmacokinetics of ambrisentan in patients with hepatic impairment (with or without cirrhosis) has not been studied. Therefore ambrisentan should not be initiated in patients with severe hepatic impairment or clinically significant elevated hepatic aminotransferases (>3xULN) (see sections 4.3 and 4.4).
Due to the class primary pharmacologic effect, a large single dose of ambrisentan (i.e. an overdose) could lower arterial pressure and have the potential for causing hypotension and symptoms related to vasodilation.
Ambrisentan was not shown to be an inhibitor of bile acid transport or to produce overt hepatotoxicity.
Inflammation and changes in the nasal cavity epithelium have been seen in rodents after chronic administration at exposures below the therapeutic levels in humans. In dogs, slight inflammatory responses were observed following chronic high dose administration of ambrisentan at exposures greater than 20–fold that observed in patients.
Nasal bone hyperplasia of the ethmoid turbinates has been observed in the nasal cavity of rats treated with ambrisentan, at exposure levels 3-fold the clinical AUC. Nasal bone hyperplasia has not been observed with ambrisentan in mice or dogs. In the rat, hyperplasia of nasal turbinate bone is a recognised response to nasal inflammation, based on experience with other compounds.
Ambrisentan was clastogenic when tested at high concentrations in mammalian cells in vitro. No evidence for mutagenic or genotoxic effects of ambrisentan were seen in bacteria or in two in vivo rodent studies.
There was no evidence of carcinogenic potential in 2 year oral studies in rats and mice. There was a small increase in mammary fibroadenomas, a benign tumor, in male rats at the highest dose only. Systemic exposure to ambrisentan in male rats at this dose (based on steady-state AUC) was 6-fold that achieved at the 10 mg/day clinical dose.
Testicular tubular atrophy, which was occasionally associated with aspermia, was observed in oral repeat dose toxicity and fertility studies with male rats and mice without safety margin. The testicular changes were not fully recoverable during the off-dose periods evaluated. However no testicular changes were observed in dog studies of up to 39 weeks duration at an exposure 35–fold that seen in humans based on AUC. In male rats, there were no effects of ambrisentan on sperm motility at all doses tested (up to 300 mg/kg/day). A slight (<10%) decrease in the percentage of morphologically normal sperms was noted at 300 mg/kg/day but not at 100 mg/kg/day (>9-fold clinical exposure at 10 mg/day). The effect of ambrisentan on male human fertility is not known.
Ambrisentan has been shown to be teratogenic in rats and rabbits. Abnormalities of the lower jaw, tongue, and/or palate were seen at all doses tested. In addition, the rat study showed an increased incidence of interventricular septal defects, trunk vessel defects, thyroid and thymus abnormalities, ossification of the basisphenoid bone, and the occurrence of the umbilical artery located on the left side of the urinary bladder instead of the right side. Teratogenicity is a suspected class effect of ERAs.
Administration of ambrisentan to female rats from late-pregnancy through lactation caused adverse events on maternal behaviour, reduced pup survival and impairment of the reproductive capability of the offspring (with observation of small testes at necropsy), at exposure 3-fold the AUC at the maximum recommended human dose.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.