Source: European Medicines Agency (EU) Revision Year: 2018 Publisher: Merck Sharp & Dohme B.V., Waarderweg 39, 2031 BN Haarlem, The Netherlands
Pharmacotherapeutic group: Antiemetics and antinauseants
ATC code: A04AD12
Aprepitant is a selective high-affinity antagonist at human substance P neurokinin 1 (NK1) receptors.
In 2 randomised, double-blind studies encompassing a total of 1,094 adult patients receiving chemotherapy that included cisplatin 70 mg/m², aprepitant in combination with an ondansetron/dexamethasone regimen (see section 4.2) was compared with a standard regimen (placebo plus ondansetron 32 mg intravenously administered on Day 1 plus dexamethasone 20 mg orally on Day 1 and 8 mg orally twice daily on Days 2 to 4). Although a 32 mg intravenous dose of ondansetron was used in clinical trials, this is no longer the recommended dose. See the product information for the selected 5-HT3 antagonist for appropriate dosing information.
Efficacy was based on evaluation of the following composite measure: complete response (defined as no emetic episodes and no use of rescue therapy) primarily during Cycle 1. The results were evaluated for each individual study and for the 2 studies combined.
A summary of the key study results from the combined analysis is shown in Table 1.
Table 1. Percent of adult patients receiving Highly Emetogenic Chemotherapy responding by treatment group and phase — Cycle 1:
| <>_.Aprepitant regimen (N=521)†% | Standard therapy (N=524)†% | Differences*% (95% CI) | |
|---|---|---|---|
| COMPOSITE MEASURES | |||
| Complete response (no emesis and no rescue therapy) | |||
| Overall (0-120 hours) | 67.7 | 47.8 | 19.9 (14.0, 25.8) |
| 0-24 hours | 86.0 | 73.2 | 12.7 (7.9, 17.6) |
| 25-120 hours | 71.5 | 51.2 | 20.3 (14.5, 26.1) |
| INDIVIDUAL MEASURES | |||
| No emesis (no emetic episodes regardless of use of rescue therapy) | |||
| Overall (0-120 hours) | 71.9 | 49.7 | 22.2 (16.4, 28.0) |
| 0-24 hours | 86.8 | 74.0 | 12.7 (8.0, 17.5) |
| 25-120 hours | 76.2 | 53.5 | 22.6 (17.0, 28.2) |
| No significant nausea (maximum VAS <25 mm on a scale of 0-100 mm) | |||
| Overall (0-120 hours) | 72.1 | 64.9 | 7.2 (1.6, 12.8) |
| 25-120 hours | 74.0 | 66.9 | 7.1 (1.5, 12.6) |
* The confidence intervals were calculated with no adjustment for gender and concomitant chemotherapy, which were included in the primary analysis of odds ratios and logistic models.
† One patient in the Aprepitant regimen only had data in the acute phase and was excluded from the overall and delayed phase analyses; one patient in the Standard regimen only had data in the delayed phase and was excluded from the overall and acute phase analyses.
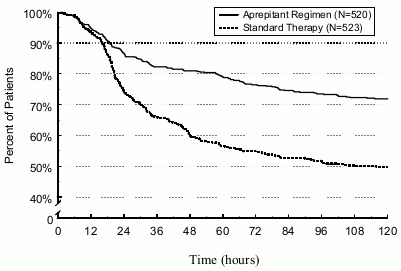
The estimated time to first emesis in the combined analysis is depicted by the Kaplan-Meier plot in Figure 1.
Figure 1. Percent of adult patients receiving Highly Emetogenic Chemotherapy who remain emesis free over time – Cycle 1:
Statistically significant differences in efficacy were also observed in each of the 2 individual studies.
In the same 2 clinical studies, 851 adult patients continued into the Multiple-Cycle extension for up to 5 additional cycles of chemotherapy. The efficacy of the aprepitant regimen was apparently maintained during all cycles.
In a randomised, double-blind study in a total of 866 adult patients (864 females, 2 males) receiving chemotherapy that included cyclophosphamide 750-1,500 mg/m²; or cyclophosphamide 500-1,500 mg/m2and doxorubicin (<60 mg/m²) or epirubicin (<100 mg/m²), aprepitant in combination with an ondansetron/dexamethasone regimen (see section 4.2) was compared with standard therapy (placebo plus ondansetron 8 mg orally (twice on Day 1, and every 12 hours on Days 2 and 3) plus dexamethasone 20 mg orally on Day 1).
Efficacy was based on evaluation of the composite measure: complete response (defined as no emetic episodes and no use of rescue therapy) primarily during Cycle 1.
A summary of the key study results is shown in Table 2.
Table 2. Percent of adult patients responding by treatment group and phase — Cycle 1 Moderately Emetogenic Chemotherapy:
| Aprepitant regimen (Ν=433)+% | Standard therapy (Ν=424)+% | Differences* (95% CI) | |
|---|---|---|---|
| COMPOSITE MEASURES | |||
| Complete response (no emesis and no rescue therapy) | |||
| Overall (0-120 hours) | 50,8 | 42,5 | 8,3 (1,6, 15,0) |
| 0-24 hours | 75,7 | 69,0 | 6,7 (0,7, 12,7) |
| 25-120 hours | 55,4 | 49,1 | 6,3 (-0,4, 13,0) |
| INDIVIDUAL MEASURES | |||
| No emesis (no emetic episodes regardless of use of rescue therapy) | |||
| Overall (0-120 hours) | 75,7 | 58,7 | 17,0 (10,8, 23,2) |
| 0-24 hours | 87,5 | 77,3 | 10,2 (5,1, 15,3) |
| 25-120 hours | 80,8 | 69,1 | 11,7 (5,9, 17,5) |
| No significant nausea (maximum VAS < 25 mm on a scale of 0-100 mm) | |||
| Overall (0-120 hours) | 60,9 | 55,7 | 5,3 (-1,3, 11,9) |
| 0-24 hours | 79,5 | 78,3 | 1,3 (-4,2, 6,8) |
| 25-120 hours | 65,3 | 61,5 | 3,9 (-2,6, 10,3) |
* The confidence intervals were calculated with no adjustment for age category (<55 years, ≥55 years) and investigator group, which were included in the primary analysis of odds ratios and logistic models.
† One patient in the Aprepitant regimen only had data in the acute phase and was excluded from the overall and delayed phase analyses.
In the same clinical study, 744 adult patients continued into the Multiple-Cycle extension for up to 3 additional cycles of chemotherapy. The efficacy of the aprepitant regimen was apparently maintained during all cycles.
In a second multicentre, randomised, double-blind, parallel-group, clinical study, the aprepitant regimen was compared with standard therapy in 848 adult patients (652 females, 196 males) receiving a chemotherapy regimen that included any intravenous dose of oxaliplatin, carboplatin, epirubicin, idarubicin, ifosfamide, irinotecan, daunorubicin, doxorubicin; cyclophosphamide intravenously (<1,500 mg/m²); or cytarabine intravenously (>1 g/m²). Patients receiving the aprepitant regimen were receiving chemotherapy for a variety of tumour types including 52% with breast cancer, 21% with gastrointestinal cancers including colorectal cancer, 13% with lung cancer and 6% with gynaecological cancers. The aprepitant regimen in combination with an ondansetron/dexamethasone regimen (see section 4.2) was compared with standard therapy (placebo in combination with ondansetron 8 mg orally (twice on Day 1, and every 12 hours on Days 2 and 3) plus dexamethasone 20 mg orally on Day 1).
Efficacy was based on the evaluation of the following primary and key secondary endpoints: No vomiting in the overall period (0 to 120 hours post-chemotherapy), evaluation of safety and tolerability of the aprepitant regimen for chemotherapy induced nausea and vomiting (CINV), and complete response (defined as no vomiting and no use of rescue therapy) in the overall period (0 to 120 hours post-chemotherapy). Additionally, no significant nausea in the overall period (0 to 120 hours post-chemotherapy) was evaluated as an exploratory endpoint, and in the acute and delayed phases as a post-hoc analysis.
A summary of the key study results is shown in Table 3.
Table 3. Percent of adult patients responding by treatment group and phase for Study 2 – Cycle 1 Moderately Emetogenic Chemotherapy:
| Aprepitant regimen (Ν=425)+% | Standard therapy (Ν=406)+% | Differences* (95% CI) | |
|---|---|---|---|
| Complete response (no emesis and no rescue therapy) | |||
| Overall (0-120 hours) | 68,7 | 56,3 | 12,4 (5,9, 18,9) |
| 0-24 hours | 89,2 | 80,3 | 8,9 (4,0, 13,8) |
| 25-120 hours | 70,8 | 60,9 | 9,9 (3,5, 16,3) |
| No emesis (no emetic episodes regardless of use of rescue therapy) | |||
| Overall (0-120 hours) | 76,2 | 62,1 | 14,1 (7,9, 20,3) |
| 0-24 hours | 92,0 | 83,7 | 8,3 (3,9, 12,7) |
| 25-120 hours | 77,9 | 66,8 | 11,1 (5,1, 17,1) |
| No significant nausea (maximum VAS < 25 mm on a scale of 0-100 mm) | |||
| Overall (0-120 hours) | 73,6 | 66,4 | 7,2 (1,0, 13,4) |
| 0-24 hours | 90,9 | 86,3 | 4,6 (0,2, 9,0) |
| 25-120 hours | 74,9 | 69,5 | 5,4 (-0,7, 11,5) |
* The confidence intervals were calculated with no adjustment for gender and region, which were included in the primary analysis using logistic models.
The benefit of aprepitant combination therapy in the full study population was mainly driven by the results observed in patients with poor control with the standard regimen such as in women, even though the results were numerically better regardless of age, tumour type or gender. Complete response to the aprepitant regimen and standard therapy, respectively, was reached in 209/324 (65%) and 161/320 (50%) in women and 83/101 (82%) and 68/87 (78%) of men.
In a randomised, double-blind, active comparator-controlled clinical study that included 302 children and adolescents (aged 6 months to 17 years) receiving moderately or highly emetogenic chemotherapy, the aprepitant regimen was compared to a control regimen for the prevention of CINV. The efficacy of the aprepitant regimen was evaluated in a single cycle (Cycle 1). Patients had the opportunity to receive open-label aprepitant in subsequent cycles (Optional Cycles 2-6); however efficacy was not assessed in these optional cycles. The aprepitant regimen for adolescents aged 12 through 17 years (n=47) consisted of EMEND capsules 125 mg orally on Day 1 and 80 mg/day on Days 2 and 3 in combination with ondansetron on Day 1. The aprepitant regimen for children aged 6 months to less than 12 years (n=105) consisted of EMEND powder for oral suspension 3.0 mg/kg (up to 125 mg) orally on Day 1 and 2.0 mg/kg (up to 80 mg) orally on Days 2 and 3 in combination with ondansetron on Day 1. The control regimen in adolescents aged 12 through 17 years (n=48) and children aged 6 months to less than 12 years (n=102) consisted of placebo for aprepitant on Days 1, 2 and 3 in combination with ondansetron on Day 1. EMEND or placebo and ondansetron were administered 1 hour and 30 minutes prior to initiation of chemotherapy, respectively. Intravenous dexamethasone was permitted as part of the antiemetic regimen for paediatric patients in both age groups, at the discretion of the physician. A dose reduction (50%) of dexamethasone was required for paediatric patients receiving aprepitant. No dose reduction was required for paediatric patients receiving the control regimen. Of the paediatric patients, 29% in the aprepitant regimen and 28% in the control regimen used dexamethasone as part of the regimen in Cycle 1.
The antiemetic activity of EMEND was evaluated over a 5-day (120 hour) period following the initiation of chemotherapy on Day 1. The primary endpoint was complete response in the delayed phase (25 to 120 hours following initiation of chemotherapy) in Cycle 1. A summary of the key study results are shown in Table 4.
Table 4. Number (%) of paediatric patients with complete response and no vomiting by treatment group and phase – Cycle 1 (Intent to treat population):
| Aprepitant regimen n/m (%) | Control regimen n/m (%) | |
|---|---|---|
| PRIMARY ENDPOINT | ||
| Complete response* – Delayed phase | 77/152 (50,7)+ | 39/150 (26,0) |
| OTHER PRESPECIFIED ENDPOINTS | ||
| Complete response* – Acute phase | 101/152 (66,4)# | 78/150 (52,0) |
| Complete response* – Overall phase | 61/152 (40,1)+ | 30/150 (20,0) |
| No vomiting§ – Overall phase | 71/152 (46,7)+ | 32/150 (21,3) |
* Complete response = No vomiting or retching or dry heaves and no use of rescue medication.
† p<0.01 when compared to control regimen
‡ p<0.05 when compared to control regimen
§ No vomiting = No vomiting or retching or dry heaves
n/m = Number of patients with desired response/number of patients included in time point.
Acute phase: 0 to 24 hours following initiation of chemotherapy.
Delayed phase: 25 to 120 hours following initiation of chemotherapy.
Overall phase: 0 to 120 hours following initiation of chemotherapy.
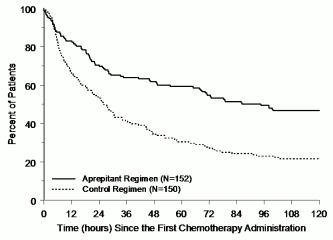
The estimated time to first vomiting after initiation of chemotherapy treatment was longer with the aprepitant regimen (estimated median time to first vomiting was 94.5 hours) compared with the control regimen group (estimated median time to first vomiting was 26.0 hours) as depicted in the Kaplan-Meier curves in Figure 2.
Figure 2. Time to first vomiting episode from start of chemotherapy administration – paediatric patients in the overall phase-Cycle 1 (Intent to treat population):
An analysis of efficacy in subpopulations in Cycle 1 demonstrated that, regardless of age category, gender, use of dexamethasone for antiemetic prophylaxis, and emetogenicity of chemotherapy, the aprepitant regimen provided better control than the control regimen with respect to the complete response endpoints.
Aprepitant displays non-linear pharmacokinetics. Both clearance and absolute bioavailability decrease with increasing dose.
The mean absolute oral bioavailability of aprepitant is 67% for the 80 mg capsule and 59% for the 125 mg capsule. The mean peak plasma concentration (Cmax) of aprepitant occurred at approximately 4 hours (tmax). Oral administration of the capsule with an approximately 800 Kcal standard breakfast resulted in an up to 40% increase in AUC of aprepitant. This increase is not considered clinically relevant.
The pharmacokinetics of aprepitant is non-linear across the clinical dose range. In healthy young adults, the increase in AUC0-∞ was 26% greater than dose proportional between 80 mg and 125 mg single doses administered in the fed state.
Following oral administration of a single 125 mg dose of EMEND on Day 1 and 80 mg once daily on Days 2 and 3, the AUC0-24hr (mean±SD) was 19.6 ± 2.5 μg·h/mL and 21.2 ± 6.3 μg·h/mL on Days 1 and 3, respectively. Cmax was 1.6 ± 0.36 μg/mL and 1.4 ± 0.22 μg/mL on Days 1 and 3, respectively.
Aprepitant is highly protein bound, with a mean of 97%. The geometric mean apparent volume of distribution at steady state (Vdss) is approximately 66 L in humans.
Aprepitant undergoes extensive metabolism. In healthy young adults, aprepitant accounts for approximately 19% of the radioactivity in plasma over 72 hours following a single intravenous administration 100-mg dose of [14C]-fosaprepitant, a prodrug for aprepitant, indicating a substantial presence of metabolites in the plasma. Twelve metabolites of aprepitant have been identified in human plasma. The metabolism of aprepitant occurs largely via oxidation at the morpholine ring and its side chains and the resultant metabolites were only weakly active. In vitro studies using human liver microsomes indicate that aprepitant is metabolised primarily by CYP3A4 and potentially with minor contribution by CYP1A2 and CYP2C19.
Aprepitant is not excreted unchanged in urine. Metabolites are excreted in urine and via biliary excretion in faeces. Following a single intravenously administered 100 mg dose of [14C]-fosaprepitant, a prodrug for aprepitant, to healthy subjects, 57% of the radioactivity was recovered in urine and 45% in faeces.
The plasma clearance of aprepitant is dose-dependent, decreasing with increased dose and ranged from approximately 60 to 72 mL/min in the therapeutic dose range. The terminal half-life ranged from approximately 9 to 13 hours.
Following oral administration of a single 125 mg dose of aprepitant on Day 1 and 80 mg once daily on Days 2 through 5, the AUC0-24hr of aprepitant was 21% higher on Day 1 and 36% higher on Day 5 in elderly (≥65 years) relative to younger adults. The Cmax was 10% higher on Day 1 and 24% higher on Day 5 in elderly relative to younger adults. These differences are not considered clinically meaningful. No dose adjustment for EMEND is necessary in elderly patients.
Following oral administration of a single 125 mg dose of aprepitant, the Cmax for aprepitant is 16% higher in females as compared with males. The half-life of aprepitant is 25% lower in females as compared with males and its tmax occurs at approximately the same time. These differences are not considered clinically meaningful. No dose adjustment for EMEND is necessary based on gender.
Mild hepatic impairment (Child-Pugh class A) does not affect the pharmacokinetics of aprepitant to a clinically relevant extent. No dose adjustment is necessary for patients with mild hepatic impairment. Conclusions regarding the influence of moderate hepatic impairment (Child-Pugh class B) on aprepitant pharmacokinetics cannot be drawn from available data.
There are no clinical or pharmacokinetic data in patients with severe hepatic impairment (Child-Pugh class C).
A single 240 mg dose of aprepitant was administered to patients with severe renal impairment (CrCl<30 mL/min) and to patients with end stage renal disease (ESRD) requiring haemodialysis.
In patients with severe renal impairment, the AUC0-∞ of total aprepitant (unbound and protein bound) decreased by 21% and Cmax decreased by 32%, relative to healthy subjects. In patients with ESRD undergoing haemodialysis, the AUC0- of total aprepitant decreased by 42% and Cmax decreased by 32%. Due to modest decreases in protein binding of aprepitant in patients with renal disease, the AUC of pharmacologically active unbound aprepitant was not significantly affected in patients with renal impairment compared with healthy subjects. Haemodialysis conducted 4 or 48 hours after dosing had no significant effect on the pharmacokinetics of aprepitant; less than 0.2% of the dose was recovered in the dialysate.
No dose adjustment for EMEND is necessary for patients with renal impairment or for patients with ESRD undergoing haemodialysis.
As part of a 3-day regimen, dosing of aprepitant capsules (125/80/80-mg) in adolescent patients (aged 12 through 17 years) achieved an AUC0-24hr above 17 µg•hr/mL on Day 1 with concentrations (Cmin) at the end of Days 2 and 3 above 0.4 µg/mL in a majority of patients. The median peak plasma concentration (Cmax) was approximately 1.3 µg/mL on Day 1, occurring at approximately 4 hours. As part of a 3-day regimen, dosing of aprepitant powder for oral suspension (3/2/2-mg/kg) in patients aged 6 months to less than12 years achieved an AUC0-24hr above 17 µg•hr/mL on Day 1 with concentrations (Cmin) at the end of Days 2 and 3 above 0.1 µg/mL in a majority of patients. The median peak plasma concentration (Cmax) was approximately 1.2 µg/mL on Day 1, occurring between 5 and 7 hours.
A population pharmacokinetic analysis of aprepitant in paediatric patients (aged 6 months through 17 years) suggests that gender and race have no clinically meaningful effect on the pharmacokinetics of aprepitant.
Using a highly specific NK1-receptor tracer, positron emission tomography (PET) studies in healthy young men have shown that aprepitant penetrates into the brain and occupies NK1 receptors in a doseand plasma-concentration-dependent manner. Aprepitant plasma concentrations achieved with the 3-day regimen of EMEND in adults are predicted to provide greater than 95% occupancy of brain NK1 receptors.
Pre-clinical data reveal no special hazard for humans based on conventional studies of single and repeated dose toxicity, genotoxicity, carcinogenic potential, toxicity to reproduction and development. However, it should be noted that systemic exposure in rodents was similar or even lower than therapeutic exposure in humans at the 125 mg/80 mg dose. In particular, although no adverse effects were noted in reproduction studies at human exposure levels, the animal exposures are not sufficient to make an adequate risk assessment in man.
In a juvenile toxicity study in rats treated from post natal day 10 to day 63 aprepitant led to an earlier vaginal opening in females from 250 mg/kg b.i.d. and to a delayed preputial separation in males, from 10 mg/kg b.i.d. There were no margins to clinically relevant exposure. There were no treatment-related effects on mating, fertility or embryonic/foetal survival, and no pathological changes in the reproductive organs. In a juvenile toxicity study in dogs treated from post natal day 14 to day 42, a decreased testicular weight and Leydig cell size were seen in the males at 6 mg/kg/day and increased uterine weight, hypertrophy of the uterus and cervix, and oedema of vaginal tissues were seen in females from 4 mg/kg/day. There were no margins to clinically relevant exposure of aprepitant. For short term treatment according to recommended dose regimen these findings are considered unlikely to be clinically relevant.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.