Source: European Medicines Agency (EU) Revision Year: 2018 Publisher: Eli Lilly Nederland B.V., Papendorpseweg 83, 3528BJ Utrecht, The Netherlands
Pharmacotherapeutic group: Selective immunosuppressants
ATC code: L04AA37
Baricitinib is a selective and reversible inhibitor of Janus kinase (JAK)1 and JAK2. In isolated enzyme assays, baricitinib inhibited the activities of JAK1, JAK2, Tyrosine Kinase 2 and JAK3 with IC50 values of 5.9, 5.7, 53 and >400 nM, respectively.
Janus kinases (JAKs) are enzymes that transduce intracellular signals from cell surface receptors for a number of cytokines and growth factors involved in haematopoiesis, inflammation and immune function. Within the intracellular signalling pathway, JAKs phosphorylate and activate signal transducers and activators of transcription (STATs), which activate gene expression within the cell. Baricitinib modulates these signalling pathways by partially inhibiting JAK1 and JAK2 enzymatic activity, thereby reducing the phosphorylation and activation of STATs.
Administration of baricitinib resulted in a dose dependent inhibition of IL-6 induced STAT3 phosphorylation in whole blood from healthy subjects with maximal inhibition observed 2 hours after dosing which returned to near baseline by 24 hours.
Mean serum IgG, IgM, and IgA values decreased by 12 weeks after starting treatment with Olumiant, and remained stable at a lower value than baseline through at least 104 weeks. For most patients, changes in immunoglobulins occurred within the normal reference range.
Mean absolute lymphocyte count increased by 1 week after starting treatment with Olumiant, returned to baseline by week 24, and then remained stable through at least 104 weeks. For most patients, changes in lymphocyte count occurred within the normal reference range.
In patients with rheumatoid arthritis, decreases in serum C-reactive protein (CRP) were observed as early as 1 week after starting treatment with Olumiant and were maintained throughout dosing.
Baricitinib induced a mean increase in serum creatinine levels of 3.8 µmol/L after two weeks of treatment, as compared to placebo, which remained stable thereafter during up to 104 weeks of treatment. This may be due to inhibition of creatinine secretion by baricitinib in the renal tubules. Consequently, estimates of the glomerular filtration rate based on serum creatinine may be slightly reduced, without actual loss of renal function or the occurrence of renal adverse events.
The influence of baricitinib on the humoral response to non-live vaccines was evaluated in 106 RA patients under stable treatment with baricitinib 2 or 4 mg, receiving inactivated pneumococcal or tetanus vaccination. The majority of these patients (n = 94) were co-treated with methotrexate. For the total population, pneumococcal vaccination resulted in a satisfactory IgG immune response in 68.0% (95% CI: 58.4%, 76.2%) of the patients. In 43.1% (95% CI: 34.0%, 52.8%) of the patients, a satisfactory IgG immune response to tetanus vaccination was achieved.
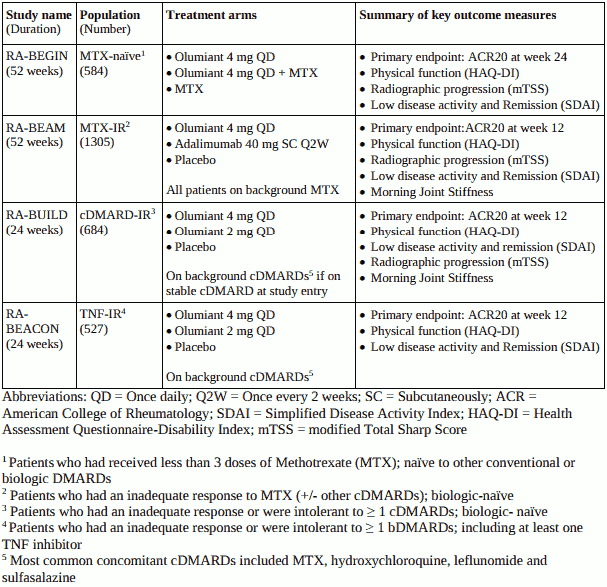
The efficacy and safety of Olumiant once daily was assessed in 4 Phase III randomised, double-blind, multicentre studies in patients with moderate to severe active rheumatoid arthritis diagnosed according to the ACR/EULAR 2010 criteria (see Table 3). Patients over 18 years of age were eligible to participate. The presence of at least 6 tender and 6 swollen joints was required at baseline. All patients who completed these studies were eligible to enrol in a long term extension study for up to 4 years continued treatment.
The RA-BEGIN Study in MTX-naïve patients is supportive for the target population of patients with an inadequate response to, or intolerance to, other DMARDs (section 4.1).
Table 3. Clinical Trial Summary:
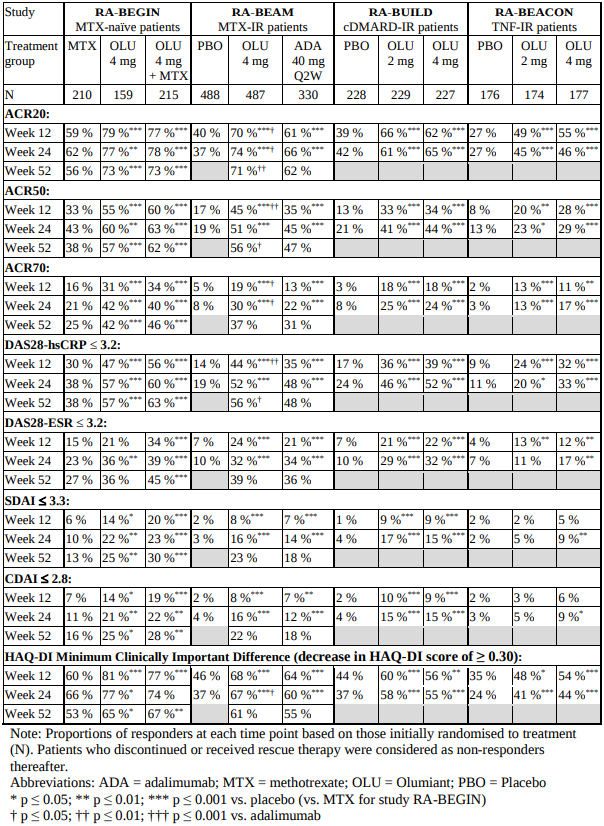
In all studies, patients treated with Olumiant 4 mg once daily had statistically significantly higher ACR20, ACR50 and ACR70 response at 12 weeks compared to placebo, MTX or adalimumab (see Table 4).Time to onset of efficacy was rapid across measures with significantly greater responses seen as early as week 1. Continued, durable response rates were observed, with ACR20/50/70 responses maintained for at least 2 years including the long-term extension study.
Treatment with Olumiant 4 mg, alone or in combination with cDMARDs, resulted in significant improvements in all individual ACR components, including tender and swollen joint counts, patient and physician global assessments, HAQ-DI, pain assessment and CRP, compared to placebo or MTX monotherapy. In RA-BEAM, treatment with Olumiant resulted in significant improvement in patient and physician global assessments, HAQ-DI, pain assessment and CRP at Weeks 12, 24 and 52 compared to adalimumab.
In placebo-controlled trials in which MTX was not required, 501 subjects randomized to baricitinib 2 mg or 4 mg received MTX as background therapy, and 303 received conventional DMARDs other than MTX (approximately half with MTX and half without). The most common concomitant DMARDs in these subjects were MTX (79% of patients), hydroxychloroquine (19%), leflunomide (11%), and sulphasalazine (9%). No relevant differences regarding efficacy and safety were observed in subgroups defined by types of concomitant DMARDs used in combination with baricitinib.
A statistically significantly greater proportion of patients treated with Olumiant 4 mg compared to placebo or MTX achieved remission, as defined by SDAI ≤3.3 and CDAI ≤2.8, at weeks 12 and 24 (Table 4).
In all 4 studies, a significantly higher proportion of patients treated with Olumiant 4 mg compared to placebo or MTX achieved low disease activity or remission (DAS28-ESR or DAS28-hsCRP ≤3.2 and DAS28-ESR or DAS28-hsCRP <2.6) at Weeks 12 and 24.
Greater rates of remission compared to placebo were observed as early as week 4. Including data from a long-term extension study, remission and low disease activity rates were maintained for at least 2 years.
Table 4. Response, Remission and Physical Function:
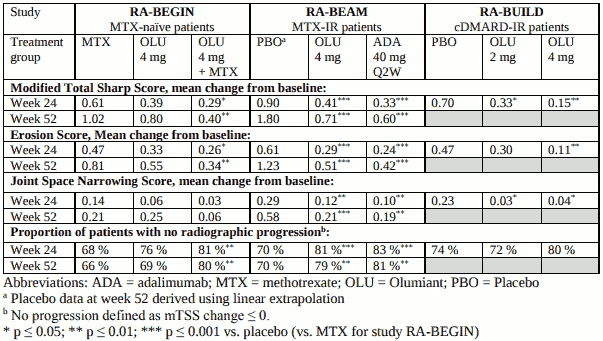
The effect of Olumiant on progression of structural joint damage was evaluated radiographically in studies RA-BEGIN, RA-BEAM and RA-BUILD and assessed using the modified Total Sharp Score (mTSS) and its components, the erosion score and joint space narrowing score.
Treatment with Olumiant 4 mg resulted in a statistically significant inhibition of progression of structural joint damage (Table 5). Analyses of erosion and joint space narrowing scores were consistent with the overall scores. The proportion of patients with no radiographic progression (mTSS change ≤0) was significantly higher with Olumiant 4 mg compared to placebo at weeks 24 and 52.
Table 5. Radiographic Changes:
Treatment with Olumiant 4 mg, alone or in combination with cDMARDs, resulted in a significant improvement in physical function compared to all comparators (placebo, MTX, adalimumab), as measured by HAQ-DI, at 12, 24 and 52 weeks. The proportion of patients achieving a clinically significant improvement (HAQ-DI ≥0.30) was also higher with Olumiant compared to placebo or MTX at week 12 (Table 4). Improvements were seen as early as Week 1 and, in studies RA-BEGIN and RA-BEAM, this was maintained for up to 52 weeks.
Treatment with Olumiant 4 mg, alone or in combination with cDMARDs, resulted in a significant improvement in pain compared to all comparators (placebo, MTX, adalimumab), as measured on a 0-100 visual analogue scale, at 12 weeks. Statistically significant pain reduction was seen as early as Week 1 and in studies RA-BEGIN and RA-BEAM this was maintained for up to 52 weeks.
In RA-BEAM and RA-BUILD, treatment with Olumiant 4 mg resulted in a significant improvement in the mean duration and severity of morning joint stiffness compared to placebo or adalimumab as assessed using daily electronic patient diaries for 12 weeks.
In all studies, Olumiant-treated patients reported improvements in patient-reported quality of life, as measured by the Short Form (36) Health Survey (SF-36) Physical Component Score and fatigue, as measured by the Functional Assessment of Chronic Illness Therapy-Fatigue score (FACIT-F).
Differences in efficacy between the 4 mg and the 2 mg doses were most notable in the bDMARD-IR population (RA-BEACON), in which statistically significant improvements in the ACR components of swollen joint count, tender joint count and ESR were shown for Olumiant 4 mg compared to placebo at Week 24 but not for Olumiant 2 mg compared to placebo. In addition, for both study RA-BEACON and RA-BUILD, onset of efficacy was faster and the effect size was generally larger for the 4 mg dose groups compared to 2 mg.
In a long-term extension study, patients from Studies RA-BEAM, RA-BUILD and RA-BEACON who achieved sustained low disease activity or remission (CDAI ≤10) after at least 15 months of treatment with Olumiant 4 mg once daily were re-randomized 1:1 in a double-blind manner to continue 4 mg once daily or reduce dose to 2 mg once daily. The majority of patients maintained low disease activity or remission based on CDAI score:
The majority of patients who lost their low disease activity or remission status after dose reduction could regain disease control after the dose was returned to 4 mg.
The European Medicines Agency has deferred the obligation to submit the results of studies with Olumiant in one or more subsets of the paediatric population in chronic idiopathic arthritis (see section 4.2 for information on paediatric use).
Following oral administration of baricitinib, a dose-proportional increase in systemic exposure was observed in the therapeutic dose range. The PK of baricitinib is linear with respect to time.
Following oral administration, baricitinib is rapidly absorbed with a median tmax of approximately 1 hour (range 0.5-3.0 h) and an absolute bioavailability of approximately 79% (CV = 3.94%). Food intake led to a decreased exposure by up to 14%, a decrease in Cmax by up to 18% and delayed tmax by 0.5 hours. Administration with meals was not associated with a clinically relevant effect on exposure.
Mean volume of distribution following intravenous infusion administration was 76 L, indicating distribution of baricitinib into tissues. Baricitinib is approximately 50% bound to plasma proteins.
Baricitinib metabolism is mediated by CYP3A4, with less than 10% of the dose identified as undergoing biotransformation. No metabolites were quantifiable in plasma. In a clinical pharmacology study, baricitinib was excreted predominately as the unchanged active substance in urine (69%) and faeces (15%) and only 4 minor oxidative metabolites were identified (3 in urine; 1 in faeces) constituting approximately 5% and 1% of the dose, respectively. In vitro, baricitinib is a substrate for CYP3A4, OAT3, Pgp, BCRP and MATE2-K, and may be a clinically relevant inhibitor of the transporter OCT1 (see section 4.5). Baricitinib is not an inhibitor of the transporters OAT1, OAT2, OAT3, OCT2, OATP1B1, OATP1B3, BCRP, MATE1 and MATE2-K at clinically relevant concentrations.
Renal elimination is the principal mechanism for baricitinib’s clearance through glomerular filtration and active secretion via OAT3, Pgp, BCRP and MATE2-K. In a clinical pharmacology study, approximately 75% of the administered dose was eliminated in the urine, while about 20% of the dose was eliminated in the faeces. Mean apparent clearance (CL/F) and half-life in patients with rheumatoid arthritis was 9.42 L/hr (CV = 34.3%) and 12.5 hrs (CV = 27.4%), respectively. Cmax and AUC at steady state are 1.4- and 2.0–fold higher, respectively, in subjects with rheumatoid arthritis compared to healthy subjects.
Renal function was found to significantly affect baricitinib exposure. The mean ratios of AUC in patients with mild and moderate renal impairment to patients with normal renal function are 1.41 (90% CI: 1.15-1.74) and 2.22 (90% CI: 1.81-2.73), respectively. The mean ratios of Cmax in patients with mild and moderate renal impairment to patients with normal renal function are 1.16 (90% CI: 0.92-1.45) and 1.46 (90% CI: 1.17-1.83), respectively. See section 4.2 for dose recommendations.
There was no clinically relevant effect on the PK of baricitinib in patients with mild or moderate hepatic impairment. The use of baricitinib has not been studied in patients with severe hepatic impairment.
Age ≥65 years or ≥75 years has no effect on baricitinib exposure (Cmax and AUC).
The safety, efficacy and pharmacokinetics of baricitinib have not yet been established in a paediatric population (see section 4.2).
Body weight, sex, race, and ethnicity did not have a clinically relevant effect on the PK of baricitinib. The mean effects of intrinsic factors on PK parameters (AUC and Cmax) were generally within the inter-subject PK variability of baricitinib. Therefore, no dose adjustment is needed based on these patient factors.
Non-clinical data reveal no special hazard for humans based on conventional studies of safety pharmacology, genotoxicity and carcinogenic potential.
Decreases in lymphocytes, eosinophils and basophils as well as lymphoid depletion in organs/tissues of the immune system were observed in mice, rats and dogs. Opportunistic infections related to demodicosis (mange) were observed in dogs at exposures approximately 7 times the human exposure. Decreases in red blood cell parameters were observed in mice, rats and dogs at exposures approximately 6 to 36 times the human exposure. Degeneration of the sternal growth plate was observed in some dogs, at low incidence and also in control animals, but with a dose-effect relationship regarding severity. At present it is not known whether this is clinically relevant.
In rat and rabbit reproductive toxicology studies, baricitinib was shown to reduce foetal growth/weight and produce skeletal malformations (at exposures of approximately 10 and 39 times the human exposure, respectively). No adverse foetal effects were observed at exposures 2 times the human exposure based on AUC.
In a combined male/female rat fertility study, baricitinib decreased overall mating performance (decreased fertility and conception indices). In female rats there were decreased numbers of corpora lutea and implantation sites, increased pre-implantation loss, and/or adverse effects on intrauterine survival of the embryos. Since there were no effects on spermatogenesis (as assessed by histopathology) or semen/sperm endpoints in male rats, the decreased overall mating performance was likely the result of these female effects.
Baricitinib was detected in the milk of lactating rats. In a pre- and postnatal development study, decreased pup weights and decreased postnatal survival were observed at exposures 4 and 21 times, respectively, the human exposure.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.