Source: European Medicines Agency (EU) Revision Year: 2021 Publisher: Camurus AB, Ideon Science Park, SE-223 70 Lund, Sweden Phone: +800 2577 2577
Treatment of opioid dependence within a framework of medical, social and psychological treatment.
Treatment is intended for use in adults and adolescents aged 16 years or over.
Administration of Buvidal is restricted to healthcare professionals. Appropriate precautions, such as to conduct patient follow-up visits with clinical monitoring according to the patient’s needs, should be taken when prescribing and dispensing buprenorphine. Take-home use or self-administration of the product by patients is not allowed.
To avoid precipitating symptoms of withdrawal, treatment with Buvidal should be started when objective and clear signs of mild to moderate withdrawal are evident (see section 4.4). Consideration should be given to the types of opioid used (that is long- or short-acting opioid), time since last opioid use and the degree of opioid dependence.
Patients not previously exposed to buprenorphine should receive a sublingual buprenorphine 4 mg dose and be observed for an hour before the first administration of weekly Buvidal to confirm tolerability to buprenorphine.
The recommended starting dose of Buvidal is 16 mg, with one or two additional 8 mg doses at least 1 day apart, to a target dose of 24 mg or 32 mg during the first treatment week. The recommended dose for the second treatment week is the total dose administered during the week of initiation.
Treatment with monthly Buvidal can be started after treatment initiation with weekly Buvidal, in accordance with the dose conversion in Table 2 and once patients have been stabilised on weekly treatment (four weeks or more, where practical).
Patients treated with sublingual buprenorphine may be switched directly to weekly or monthly Buvidal, starting on the day after the last daily buprenorphine sublingual treatment dose in accordance with the dosing recommendations in Table 1. Closer monitoring of patients is recommended during the dosing period after the switch.
Table 1. Conventional sublingual buprenorphine daily treatment doses and recommended corresponding doses of weekly and monthly Buvidal:
| Dose of daily sublingual buprenorphine | Dose of weekly Buvidal | Dose of monthly Buvidal |
|---|---|---|
| 2-6 mg | 8 mg | |
| 8-10 mg | 16 mg | 64 mg |
| 12-16 mg | 24 mg | 96 mg |
| 18-24 mg | 32 mg | 128 mg |
Patients may be switched from sublingual buprenorphine 26-32 mg directly to monthly Buvidal 160 mg with close monitoring during the dosing period after the switch.
The dose of buprenorphine in mg can differ between sublingual products, which needs to be taken into consideration on a product-by-product basis. The pharmacokinetic properties of Buvidal are described in section 5.2.
Buvidal can be administered weekly or monthly. Doses may be increased or decreased and patients can be switched between weekly and monthly products according to individual patient’s needs and treating physician’s clinical judgement as per recommendations in Table 1. Following switching, patients may need closer monitoring. Assessment of long-term treatment is based on 48-week data.
A maximum of one supplemental Buvidal 8 mg dose may be administered at an unscheduled visit between regular weekly and monthly doses, based on individual patient’s temporary needs. The maximum dose per week for patients who are on weekly Buvidal treatment is 32 mg with an additional 8 mg dose. The maximum dose per month for patients who are on monthly Buvidal treatment is 160 mg.
To avoid missed doses, the weekly dose may be administered up to 2 days before or after the weekly time point, and the monthly dose may be administered up to 1 week before or after the monthly time point.
If a dose is missed, the next dose should be administered as soon as practically possible.
If Buvidal treatment is discontinued, its prolonged-release characteristics and any withdrawal symptoms experienced by the patient must be considered, see section 4.4. If the patient is switched to treatment with sublingual buprenorphine, this should be done one week after the last weekly dose or one month after the last monthly dose of Buvidal according to the recommendations in Table 1.
The efficacy and safety of buprenorphine in elderly patients >65 years have not been established. No recommendation on posology can be made.
In general, recommended dosing for elderly patients with normal renal function is the same as for younger adult patients with normal renal function. However, because elderly patients may have diminished renal/hepatic function, dose adjustment may be necessary (see Hepatic impairment and Renal impairment below).
Buprenorphine should be used with caution in patients with moderate hepatic impairment (see section 5.2). In patients with severe hepatic impairment, the use of buprenorphine is contraindicated (see section 4.3).
Modification of the buprenorphine dose is not required for patients with renal impairment. Caution is recommended when dosing patients with severe renal impairment (creatinine clearance <30 ml/min) (see sections 4.4 and 5.2).
The safety and efficacy buprenorphine in children and adolescents below 16 years of age have not been established (see section 4.4). No data are available.
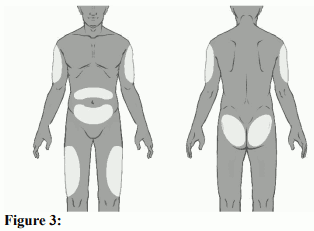
Buvidal is intended for subcutaneous administration only. It should be injected slowly and completely into the subcutaneous tissue of different areas (buttock, thigh, abdomen, or upper arm), provided there is enough subcutaneous tissue. Each area can have multiple injection sites. Injection sites should be rotated for both weekly and monthly injections. A minimum of 8 weeks should be left before reinjecting a previously used injection site with the weekly dose. There is no clinical data supporting reinjection of the monthly dose into the same site. This is unlikely to be a safety concern.The decision to reinject at the same site should also be guided by the attending physicians' clinical judgement. Administered dose should be as a single injection and not divided. The dose must not be administered intravascularly (intravenously), intramuscularly or intradermally (into the skin) (see section 4.4). See section 6.6 for administration instructions.
Respiratory depression, as a result of central nervous system depression, is the primary symptom requiring intervention in the case of buprenorphine overdose because it may lead to respiratory arrest and death. Preliminary symptoms of overdose may also include excessive sweating, somnolence, amblyopia, miosis, hypotension, nausea, vomiting and/or speech disorders.
General supportive measures should be instituted, including close monitoring of respiratory and cardiac status of the patient. Symptomatic treatment of respiratory depression, following standard intensive care measures, should be instituted. A patent airway and assisted or controlled ventilation must be assured. The patient should be transferred to an environment within which full resuscitation facilities are available. If the patient vomits, precautions must be taken to prevent aspiration. Use of an opioid antagonist (i.e. naloxone) is recommended, despite the modest effect it may have in reversing the respiratory symptoms of buprenorphine compared with its effects on full agonist opioids.
The long duration of action of buprenorphine and the prolonged release from Buvidal, should be taken into consideration when determining length of treatment needed to reverse the effects of an overdose, (see section 4.4). Naloxone can be cleared more rapidly than buprenorphine, allowing for a return of previously controlled buprenorphine overdose symptoms.
3 years.
Do not refrigerate or freeze.
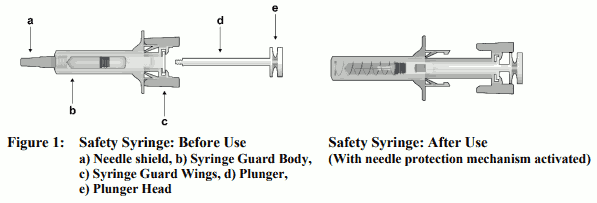
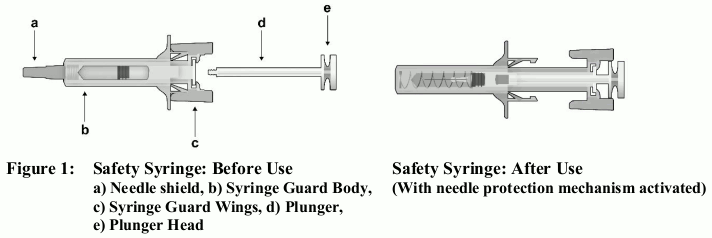
A 1 mL pre-filled syringe (glass, Type I) with plunger stopper (fluoropolymer-coated bromobutyl rubber) with needle (½-inch, 23 gauge, 12 mm) and needle shield (styrene butadiene rubber). The prefilled syringe is assembled in a safety device for post-injection needlestick prevention. The needle shield of the safety syringe may contain rubber latex that may cause allergic reactions in latexsensitive individuals.
Pack sizes: Pack contains 1 pre-filled syringe with stopper, needle, needle shield, safety device and 1 plunger rod.
Important information:
Before administration:
Safety syringe parts:
Please note that the smallest injection volume is barely visible in the viewing window as the spring of the safety device is “covering” part of the glass cylinder close to the needle.
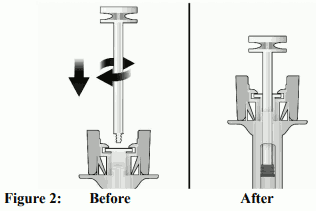
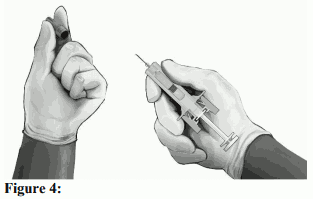
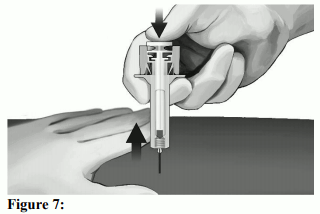
Administration (see also section 4.2):
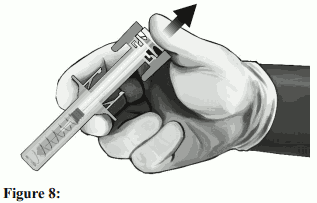
Disposing of the syringe:
Any unused medicinal product or waste material should be disposed of in accordance with local requirements.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.