Source: European Medicines Agency (EU) Revision Year: 2022 Publisher: ViiV Healthcare BV, Van Asch van Wijckstraat 55H, 3811 LP Amersfoort, Netherlands
Hypersensitivity to the active substance or to any of the excipients listed in section 6.1.
Concomitant use with rifampicin, rifapentine, carbamazepine, oxcarbazepine, phenytoin or phenobarbital (see section 4.5).
Before starting the regimen, it should be taken into account that multivariable analyses indicate that a combination of at least 2 of the following baseline factors may be associated with an increased risk of virological failure: archived rilpivirine resistance mutations, HIV-1 subtype A6/A1, or BMI ≥30 kg/m². In patients with an incomplete or uncertain treatment history without pre-treatment resistance analyses, caution is warranted in the presence of either BMI ≥30 kg/m² or HIV-1 A6/A1 subtype (see section 5.1).
Hypersensitivity reactions have been reported in association with integrase inhibitors including cabotegravir. These reactions were characterised by rash, constitutional findings and sometimes organ dysfunction, including liver injury. Vocabria and other suspected medicinal products should be discontinued immediately, should signs or symptoms of hypersensitivity develop (including, but not limited to, severe rash, or rash accompanied by fever, general malaise, fatigue, muscle or joint aches, blisters, oral lesions, conjunctivitis, facial oedema, hepatitis, eosinophilia or angioedema). Clinical status, including liver aminotransferases should be monitored and appropriate therapy initiated. (see sections 4.2 and 5.1).
Hepatotoxicity has been reported in a limited number of patients receiving Vocabria with or without known pre-existing hepatic disease (see section 4.8). Administration of cabotegravir oral lead-in was used in clinical studies to help identify patients who may be at risk of hepatotoxicity. Monitoring of liver chemistries is recommended and treatment with Vocabria should be discontinued if hepatotoxicity is suspected.
Patients with hepatitis B co-infection were excluded from studies with Vocabria. It is not recommended to initiate Vocabria in patients with hepatitis B co-infection. Physicians should refer to current treatment guidelines for the management of HIV infection in patients co-infected with hepatitis B virus. Limited data is available in patients with hepatitis C co-infection. Monitoring of liver function is recommended in patients with hepatitis C co-infection.
Caution should be given to prescribing Vocabria tablets with medicinal products that may reduce its exposure (see section 4.5).
Polyvalent cation containing antacids are recommended to be taken at least 2 hours before and 4 hours after taking Vocabria tablets (see section 4.5).
While effective viral suppression with antiretroviral therapy has been proven to substantially reduce the risk of sexual transmission, a residual risk cannot be excluded. Precautions to prevent transmission should be taken in accordance with national guidelines.
In HIV-infected patients with severe immune deficiency at the time of institution of combination antiretroviral therapy (CART), an inflammatory reaction to asymptomatic or residual opportunistic pathogens may arise and cause serious clinical conditions, or aggravation of symptoms. Typically, such reactions have been observed within the first few weeks or months of initiation of CART. Relevant examples are cytomegalovirus retinitis, generalised and/or focal mycobacterial infections, and Pneumocystis jirovecii pneumonia. Any inflammatory symptoms should be evaluated, and treatment instituted when necessary. Autoimmune disorders (such as Graves' disease and autoimmune hepatitis) have also been reported to occur in the setting of immune reconstitution, however, the reported time to onset is more variable and these events can occur many months after initiation of treatment.
Patients should be advised that Vocabria or any other antiretroviral therapy do not cure HIV infection and that they may still develop opportunistic infections and other complications of HIV infection. Therefore, patients should remain under close clinical observation by physicians experienced in the treatment of these associated HIV diseases.
Patients with rare hereditary problems of galactose intolerance, total lactase deficiency or glucosegalactose malabsorption should not take this medicine.
This medicinal product contains less than 1 mmol sodium (23 mg) per tablet, that is to say essentially ‘sodium-free’.
Vocabria tablets, in combination with rilpivirine tablets, are indicated for the treatment of HIV-1, therefore, the prescribing information for rilpivirine tablets should be consulted for associated interactions.
Cabotegravir is primarily metabolised by uridine diphosphate glucuronosyl transferase (UGT) 1A1 and to a lesser extent by UGT1A9. Medicinal products which are strong inducers of UGT1A1 or UGT1A9 are expected to decrease cabotegravir plasma concentrations leading to lack of efficacy (see section 4.3 and table 5 below). In poor metabolizers of UGT1A1, representing a maximum clinical UGT1A1 inhibition, the mean AUC, Cmax and Ctau of oral cabotegravir increased by up to 1.5-fold. The impact of an UGT1A1 inhibitor may be slightly more pronounced, however, considering the safety margins of cabotegravir, this increase is not expected to be clinically relevant. No dosing adjustments for Vocabria are, therefore, recommended in the presence of UGT1A1 inhibitors (e.g. atazanavir, erlotinib, sorafenib).
Cabotegravir is a substrate of P-glycoprotein (P-gp) and breast cancer resistance protein (BCRP), however, because of its high permeability, no alteration in absorption is expected when coadministered with either P-gp or BCRP inhibitors.
In vivo, cabotegravir did not have an effect on midazolam, a cytochrome P450 (CYP) 3A4 probe. In vitro, cabotegravir did not induce CYP1A2, CYP2B6, or CYP3A4.
In vitro, cabotegravir inhibited the organic anion transporters (OAT) 1 (IC50=0.81 µM) and OAT3 (IC50=0.41 µM). Therefore, caution is advised when co-dosing with narrow therapeutic index OAT1/3 substrate drugs (e.g. methotrexate).
Based on the in vitro and clinical drug interaction profile, cabotegravir is not expected to alter concentrations of other anti-retroviral medications including protease inhibitors, nucleoside reverse transcriptase inhibitors, non-nucleoside reverse transcriptase inhibitors, integrase inhibitors, entry inhibitors and ibalizumab.
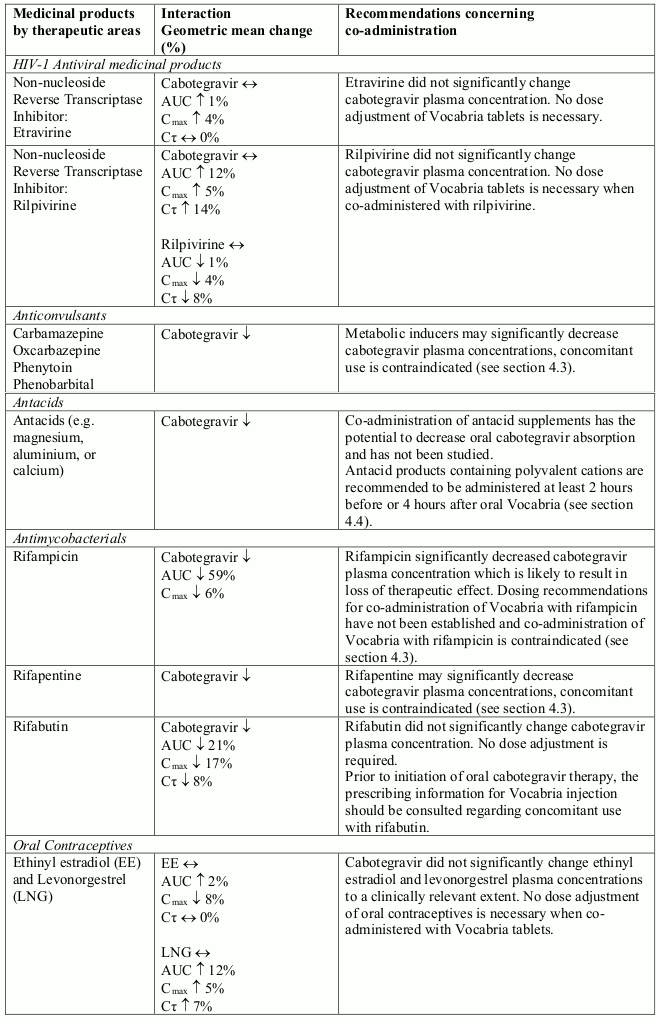
The drug interaction data provided in Table 2 is obtained from studies with oral cabotegravir (increase is indicated as “↑”, decrease as “↓”, no change as “↔”, area under the concentration versus time curve as “AUC”, maximum observed concentration as "Cmax", concentration at end of dosing interval as "Cτ").
Table 2. Drug Interactions:
There are a limited amount of data from the use of cabotegravir in pregnant women. The effect of Vocabria on human pregnancy is unknown.
Cabotegravir was not teratogenic when studied in pregnant rats and rabbits but, exposures higher than the therapeutic dose showed reproductive toxicity in animals (see section 5.3). The relevance to human pregnancy is unknown.
Vocabria tablets are not recommended during pregnancy unless the expected benefit justifies the potential risk to the foetus.
It is expected that cabotegravir will be secreted into human milk based on animal data, although this has not been confirmed in humans.
It is recommended that HIV infected women do not breast-feed their infants under any circumstances in order to avoid transmission of HIV.
There are no data on the effects of cabotegravir on human male or female fertility. Animal studies indicate no effects of cabotegravir on male or female fertility (see section 5.3).
Patients should be informed that dizziness, fatigue and somnolence has been reported during treatment with Vocabria. The clinical status of the patient and the adverse reaction profile of Vocabria should be borne in mind when considering the patient’s ability to drive or operate machinery.
The most frequently reported adverse reaction (ARs) from monthly dosing studies were headache (up to 12%) and pyrexia4 (10%).
The most frequently reported ARs, considered by the investigator as causally related, from ATLAS2M every 2 month dosing were headache (7%) and pyrexia4 (7%).
The ARs identified for cabotegravir and rilpivirine are listed in Table 3 by body system organ class and frequency. Frequencies are defined as very common (≥1/10), common (≥1/100 to <1/10), uncommon (≥1/1,000 to <1/100), rare (≥1/10,000 to <1/1,000), very rare (<1/10,000).
Table 3. Tabulated summary of adverse reactions1:
| MedDRA System Organ Class (SOC) | Frequency Category | ARs for Vocabria + rilpivirine regimen |
|---|---|---|
| Immune system disorders | Uncommon | Type I hypersensitivity* |
| Psychiatric disorders | Common | Depression Anxiety Abnormal dreams Insomnia |
| Uncommon | Suicide attempt; Suicidal ideation (particularly in patients with a pre-existing history of psychiatric illness) | |
| Nervous system disorders | Very common | Headache |
| Common | Dizziness | |
| Uncommon | Somnolence | |
| Gastrointestinal disorders | Common | Nausea Vomiting Abdominal pain2 Flatulence Diarrhoea |
| Hepatobiliary Disorders | Uncommon | Hepatotoxicity |
| Skin and subcutaneous tissue disorders | Common | Rash3 |
| Uncommon | Urticaria* Angioedema* | |
| Musculoskeletal and connective tissue disorders | Common | Myalgia |
| General disorders and administrative site conditions | Very common | Pyrexia4 |
| Common | Fatigue Asthenia Malaise | |
| Investigations | Common | Weight increased |
| Uncommon | Transaminase increased Blood bilirubin increased |
1 The frequency of the identified ARs are based on all reported occurrences of the events and are not limited to those considered at least possibly related by the investigator.
2 Abdominal pain includes the following grouped MedDRA preferred term: upper abdominal pain.
3 Rash includes the following grouped MedDRA preferred terms: rash, rash erythematous, rash generalised, rash macular, rash maculo-papular, rash morbilliform, rash papular, rash pruritic.
4 Pyrexia includes the following grouped MedDRA preferred terms: feeling hot, body temperature increased. The majority of pyrexia events were reported within one week of injections.
* Please refer to section 4.4.
The overall safety profile at Week 96 and Week 124 in the FLAIR study was consistent with that observed at Week 48, with no new safety findings identified. In the extension phase of the FLAIR study, initiating the CAB LA + RPV LA regimen with Direct to Injection did not identify any new safety concerns related to omitting the oral lead-in phase (see section 5.1).
At the Week 48 time point, subjects in studies FLAIR and ATLAS, who received Vocabria plus rilpivirine gained a median of 1.5 kg in weight; subjects continuing on their current antiretroviral therapy (CAR) gained a median of 1.0 kg (pooled analysis). In the individual studies FLAIR and ATLAS, the median weight gains in the Vocabria plus rilpivirine arms were 1.3 kg and 1.8 kg respectively, compared to 1.5 kg and 0.3 kg in the CAR arms.
At the 48 week timepoint, in ATLAS-2M the median weight gain in both the monthly and 2-monthly Vocabria plus rilpivirine dosing arms was 1.0 kg.
Small, non-progressive increases in total bilirubin (without clinical jaundice) were observed with treatment with Vocabria plus rilpivirine. These changes are not considered clinically relevant as they likely reflect competition between cabotegravir and unconjugated bilirubin for a common clearance pathway (UGT1A1).
Elevated transaminases (ALT/AST) were observed in subjects receiving Vocabria plus rilpivirine during clinical studies. These elevations were primarily attributed to acute viral hepatitis. A few subjects on oral therapy had transaminase elevations attributed to suspected drug-related hepatotoxicity; these changes were reversible upon discontinuation of treatment (see section 4.4).
Elevated lipases were observed during clinical trials with Vocabria plus rilpivirine; Grade 3 and 4 lipase increases occurred at a higher incidence with Vocabria plus rilpivirine compared with CAR. These elevations were generally asymptomatic and did not lead to Vocabria plus rilpivirine discontinuation. One case of fatal pancreatitis with Grade 4 lipase and confounding factors (including history of pancreatitis) has been reported in study ATLAS-2M, for which causality to the injection regimen could not be ruled out.
Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via the national reporting system listed in Appendix V.
Not applicable.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.