Source: European Medicines Agency (EU) Revision Year: 2017 Publisher: Genzyme Europe B.V., Gooimeer 10, NL-1411 DD Naarden, The Netherlands
Life threatening hypersensitivity (anaphylactic reaction) to the active substance or to any of the excipients listed in section 6.1, when rechallenge was unsuccessful (see sections 4.4 and 4.8).
Serious and life-threatening anaphylactic reactions, including anaphylactic shock, have been reported in infantile- and late-onset patients during Myozyme infusions (see section 4.8). Because of the potential for severe infusion associated reactions, appropriate medical support measures, including cardiopulmonary resuscitation equipment, should be readily available when Myozyme is administered. If severe hypersensitivity or anaphylactic reactions occur, immediate discontinuation of Myozyme infusion should be considered and appropriate medical treatment should be initiated. The current medical standards for emergency treatment of anaphylactic reactions are to be observed.
Approximately half of the patients treated with Myozyme in infantile-onset clinical studies and 28% of the patients treated with Myozyme in a late-onset clinical study developed infusion associated reactions (IARs). IARs are defined as any related adverse event occurring during the infusion or during the hours following infusion. Some reactions were severe (see section 4.8). A tendency was observed in infantile patients treated with a higher dose (40 mg/kg) to experience more symptoms when developing IARs. Infantile onset patients who develop high IgG antibody titres appear to be at higher risk for developing more frequent IARs. Patients with an acute illness (e.g. pneumonia, sepsis) at the time of Myozyme infusion appear to be at greater risk for IARs. Careful consideration should be given to the patient’s clinical status prior to administration of Myozyme. Patients should be closely monitored and all cases of IARs, delayed reactions and possible immunological reactions should be reported to the marketing authorisation holder.
Patients who have experienced IARs (and in particular anaphylactic reactions) should be treated with caution when re-administering Myozyme (see sections 4.3 and 4.8). Mild and transient effects may not require medical treatment or discontinuation of the infusion. Reduction of the infusion rate, temporary interruption of the infusion, or pre-treatment, generally with oral antihistamine and/or antipyretics and/or corticosteroids, has effectively managed most reactions. IARs may occur at any time during the infusion of Myozyme or generally up to 2 hours after, and are more likely with higher infusion rates.
Patients with advanced Pompe disease may have compromised cardiac and respiratory function, which may predispose them to a higher risk of severe complications from infusion associated reactions. Therefore, these patients should be monitored more closely during administration of Myozyme.
In clinical studies, the majority of patients developed IgG antibodies to alglucosidase alfa typically within 3 months of treatment. Thus seroconversion is expected to occur in most patients treated with Myozyme. A tendency was observed for infantile-onset patients treated with a higher dose (40 mg/kg) to develop higher titres of IgG antibodies. There does not appear to be a correlation between the onset of IARs and the time of IgG antibody formation. A limited number of the IgG positive patients evaluated tested positive for inhibitory effects on in vitro testing. Due to the rarity of the condition and the limited experience to date, the effect of IgG antibody formation on safety and efficacy is currently not fully established. The probability of a poor outcome and of developing high and sustained IgG antibody titres appears higher among CRIM-negative patients (Cross Reactive Immunologic Material; patients in whom no endogenous GAA protein was detected by Western blot analysis) than among CRIM-positive patients (patients in whom endogenous GAA protein was detected by Western blot analysis). However, high and sustained IgG antibody titres also occur in some CRIM-positive patients. The cause of a poor clinical outcome and of developing high and sustained IgG antibody titres is thought to be multi-factorial. IgG antibody titres should be regularly monitored.
Patients who experience hypersensitivity reactions may also be tested for IgE antibodies to alglucosidase alfa and other mediators of anaphylaxis. Patients who develop IgE antibodies to alglucosidase alfa appear to be at a higher risk for the occurrence of IARs when Myozyme is readministered (see section 4.8). Therefore, these patients should be monitored more closely during administration of Myozyme. Some IgE positive patients were successfully rechallenged with Myozyme using a slower infusion rate at lower initial doses and have continued to receive Myozyme under close clinical supervision.
Severe cutaneous reactions, possibly immune mediated, have been reported with alglucosidase alfa, including ulcerative and necrotizing skin lesions (see section 4.8). Nephrotic syndrome was observed in a few Pompe patients treated with alglucosidase alfa and who had high IgG antibody titres (≥102,400) (see section 4.8). In these patients renal biopsy showed immune complex deposition. Patients improved following treatment interruption. It is therefore recommended to perform periodic urinalysis among patients with high IgG antibody titres.
Patients should be monitored for signs and symptoms of systemic immune-mediated reactions involving skin and other organs while receiving alglucosidase alfa. If immune-mediated reactions occur, discontinuation of the administration of alglucosidase alfa should be considered and appropriate medical treatment initiated. The risks and benefits of re-administering alglucosidase alfa following an immune-mediated reaction should be considered. Some patients have been successfully rechallenged and continued to receive alglucosidase alfa under close clinical supervision.
Patients with Pompe disease are at risk of respiratory infections due to the progressive effects of the disease on the respiratory muscles. Immunosuppressive agents have been administered in experimental settings in a small number of patients, in an attempt to reduce or prevent the development of antibodies to alglucosidase alfa. Fatal and life-threatening respiratory infections have been observed in some of these patients. Therefore, treating patients with Pompe disease with immunosuppressive agents may further increase the risk of developing severe respiratory infections and vigilance is recommended.
No interactions studies have been performed. Because it is a recombinant human protein, alglucosidase alfa is an unlikely candidate for cytochrome P450 mediated drug-drug interactions.
There are no data from the use of alglucosidase alfa in pregnant women. Studies in animals have shown reproductive toxicity (see section 5.3). The potential risk for humans is unknown. Myozyme should not be used during pregnancy unless clearly necessary.
Alglucosidase alfa may be excreted in breast milk. Because there are no data available on effects in neonates exposed to alglucosidase alfa via breast milk, it is recommended to stop breast-feeding when Myozyme is used.
There are no clinical data on the effects of alglucosidase alfa on fertility. Preclinical data did not reveal any significant adverse findings (see section 5.3).
No studies on the effects on the ability to drive and use machines have been performed. Because dizziness has been reported as an infusion associated reaction, this may affect the ability to drive and use machines on the day of the infusion.
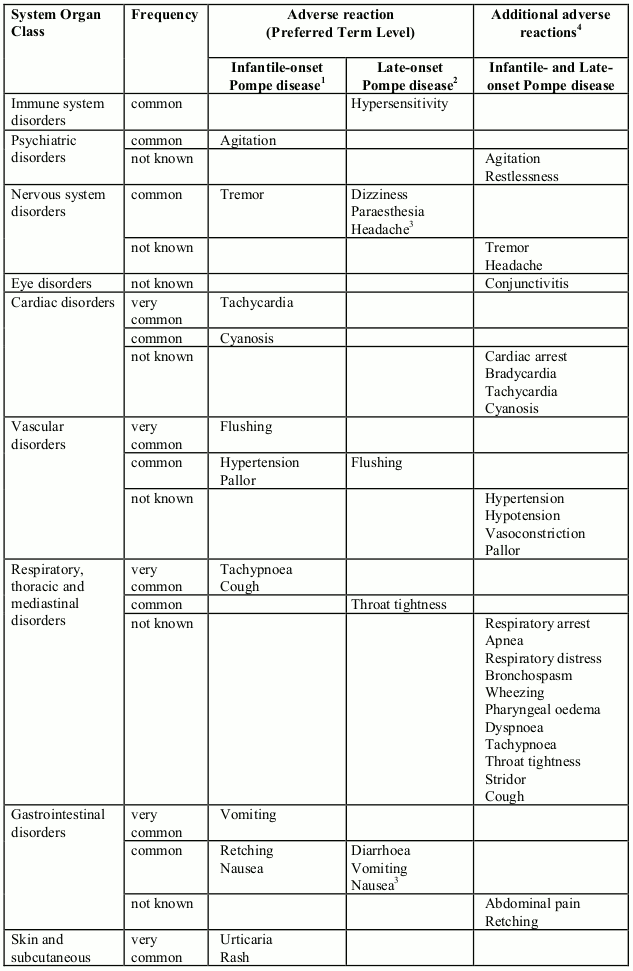
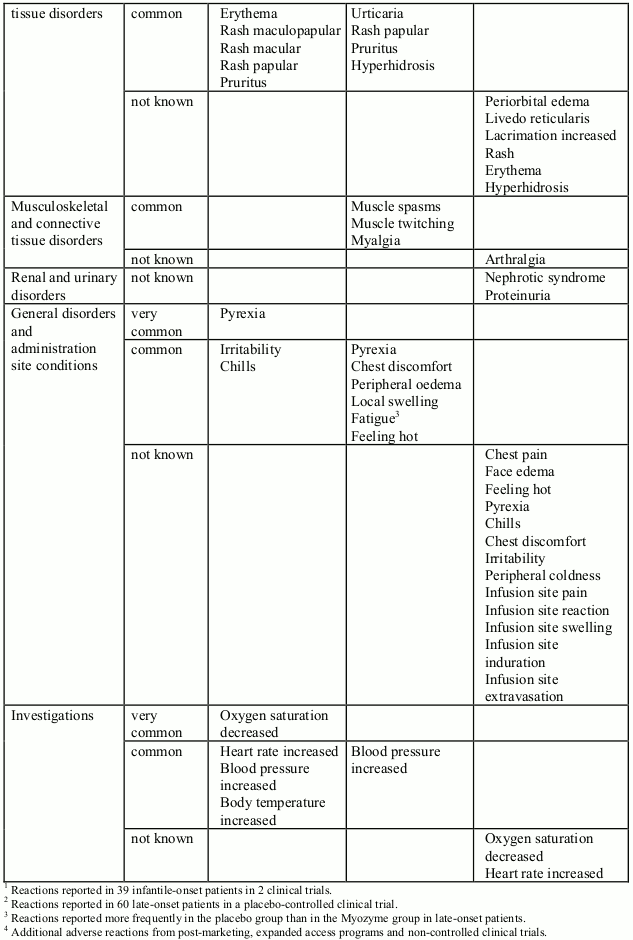
In clinical trials, 39 infantile-onset patients were treated with Myozyme for more than three years (168 weeks with a median of 121 weeks; see section 5.1). Adverse reactions reported in at least 2 patients are listed in Table 1 by System Organ Class. Adverse reactions were mostly mild to moderate in intensity and almost all occurred during the infusion or during the 2 hours following the infusion (infusion associated reactions, IARs). Serious infusion reactions including urticaria, rales, tachycardia, decreased oxygen saturation, bronchospasm, tachypnea, periorbital edema and hypertension have been reported.
In a placebo-controlled study lasting 78 weeks, 90 patients with late-onset Pompe disease, aged 10 to 70 years, were treated with Myozyme or placebo randomized in a 2:1 ratio (see section 5.1). Overall, the numbers of patients experiencing adverse reactions and serious adverse reactions were comparable between the two groups. The most common adverse reactions observed were IARs. Slightly more patients in the Myozyme group than in the placebo group experienced IARs (28% versus 23%). The majority of these reactions were non-serious, mild to moderate in intensity and resolved spontaneously. Adverse reactions reported in at least 2 patients are listed in Table 1. Serious adverse reactions reported in 4 patients treated with Myozyme were: angioedema, chest discomfort, throat tightness, non-cardiac chest pain and supraventricular tachycardia. Reactions in 2 of these patients were IgE-mediated hypersensitivity reactions.
Table 1: Adverse reactions (reported in at least 2 patients) and adverse reactions reported in postmarketing setting, expanded access programs and non-controlled clinical trials, per System Organ Class, presented by frequency categories: very common (≥1/10), common (≥1/100 to<1/10), uncommon (≥1/1,000 to <1/100), rare (≥1/10,000 to <1/1,000), very rare (<1/10,000) and not known (cannot be estimated from the available data). Due to the small patient population, an adverse reaction reported in 2 patients is classified as common. Within each frequency grouping, adverse reactions are presented in order of decreasing seriousness.
A small number of patients (<1%) in clinical trials and in the commercial setting developed anaphylactic shock and/or cardiac arrest during Myozyme infusion that required life-support measures. Reactions generally occurred shortly after initiation of the infusion. Patients presented with a constellation of signs and symptoms, primarily respiratory, cardiovascular, edematous and/or cutaneous in nature (see section 4.4).
Recurrent reactions consisting of flu-like illness or a combination of events such as fever, chills, myalgia, arthralgia, pain, or fatigue occurring post-infusion and lasting usually for a few days, have been observed in some patients treated with alglucosidase alfa. The majority of patients were successfully re-challenged with alglucosidase alfa using lower doses and/or pretreatment with antiinflammatory drugs and/or corticosteroids and have continued to receive treatment under close clinical supervision.
Patients with moderate to severe or recurrent IARs have been evaluated for alglucosidase alfa specific IgE antibodies; some patients tested positive including some who experienced an anaphylactic reaction.
Nephrotic syndrome as well as severe cutaneous reactions, possibly immune mediated, have been reported with alglucosidase alfa including ulcerative and necrotizing skin lesions (see section 4.4).
Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via the national reporting system listed in Appendix V.
In the absence of compatibility studies, this medicinal product must not be mixed with other medicinal products.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.