Source: European Medicines Agency (EU) Revision Year: 2019 Publisher: Roche Registration GmbH, Emil-Barell-Strasse 1, 79639, Grenzach-Wyhlen, Germany
Tecentriq as monotherapy is indicated for the treatment of adult patients with locally advanced or metastatic urothelial carcinoma (UC):
Tecentriq, in combination with bevacizumab, paclitaxel and carboplatin, is indicated for the first-line treatment of adult patients with metastatic non-squamous non-small cell lung cancer (NSCLC). In patients with EGFR mutant or ALK-positive NSCLC, Tecentriq, in combination with bevacizumab, paclitaxel and carboplatin, is indicated only after failure of appropriate targeted therapies (see section 5.1).
Tecentriq as monotherapy is indicated for the treatment of adult patients with locally advanced or metastatic NSCLC after prior chemotherapy. Patients with EGFR mutant or ALK-positive NSCLC should also have received targeted therapies before receiving Tecentriq (see section 5.1).
Tecentriq, in combination with nab-paclitaxel and carboplatin, is indicated for the first-line treatment of adult patients with metastatic non-squamous NSCLC who do not have EGFR mutant or ALK-positive NSCLC (see section 5.1).
Tecentriq, in combination with carboplatin and etoposide, is indicated for the first-line treatment of adult patients with extensive-stage small cell lung cancer (ES-SCLC) (see section 5.1).
Tecentriq must be initiated and supervised by physicians experienced in the treatment of cancer.
Patients with previously untreated UC should be selected for treatment based on the tumour expression of PD-L1 confirmed by a validated test (see section 5.1).
The recommended dose of Tecentriq is 1,200 mg administered intravenously every three weeks.
Please also refer to the full prescribing information for the combination products (see also section 5.1).
During the induction phase, the recommended dose of Tecentriq is 1,200 mg administered by intravenous infusion, followed by bevacizumab, paclitaxel, and then carboplatin every three weeks for four or six cycles.
The induction phase is followed by a maintenance phase without chemotherapy in which 1,200 mg Tecentriq followed by bevacizumab, is administered by intravenous infusion every three weeks.
During the induction phase, the recommended dose of Tecentriq is 1,200 mg administered by intravenous infusion, followed by nab-paclitaxel and carboplatin every three weeks for four or six cycles. For each 21-day cycle, Tecentriq, nab-paclitaxel, and carboplatin are administered on day 1. In addition, nab-paclitaxel is administered on days 8 and 15.
The induction phase is followed by a maintenance phase without chemotherapy in which 1,200 mg Tecentriq is administered by intravenous infusion every three weeks.
During the induction phase, the recommended dose of Tecentriq is 1,200 mg administered by intravenous infusion followed by carboplatin, and then etoposide administered by intravenous infusion on day 1. Etoposide is also administered by intravenous infusion on days 2 and 3. This regimen is administered every three weeks for four cycles.
The induction phase is followed by a maintenance phase without chemotherapy in which 1,200 mg Tecentriq is administered by intravenous infusion every three weeks.
It is recommended that patients are treated with Tecentriq until loss of clinical benefit (see section 5.1) or unmanageable toxicity.
For ES-SCLC and for first-line NSCLC, in patients given Tecentriq in combination with carboplatin and nab-paclitaxel, it is recommended that patients are treated with Tecentriq until disease progression or unmanageable toxicity. Treatment beyond disease progression may be considered at the discretion of the physician (see section 5.1).
If a planned dose of Tecentriq is missed, it should be administered as soon as possible. The schedule of administration must be adjusted to maintain a 3-week interval between doses.
Dose reductions of Tecentriq are not recommended.
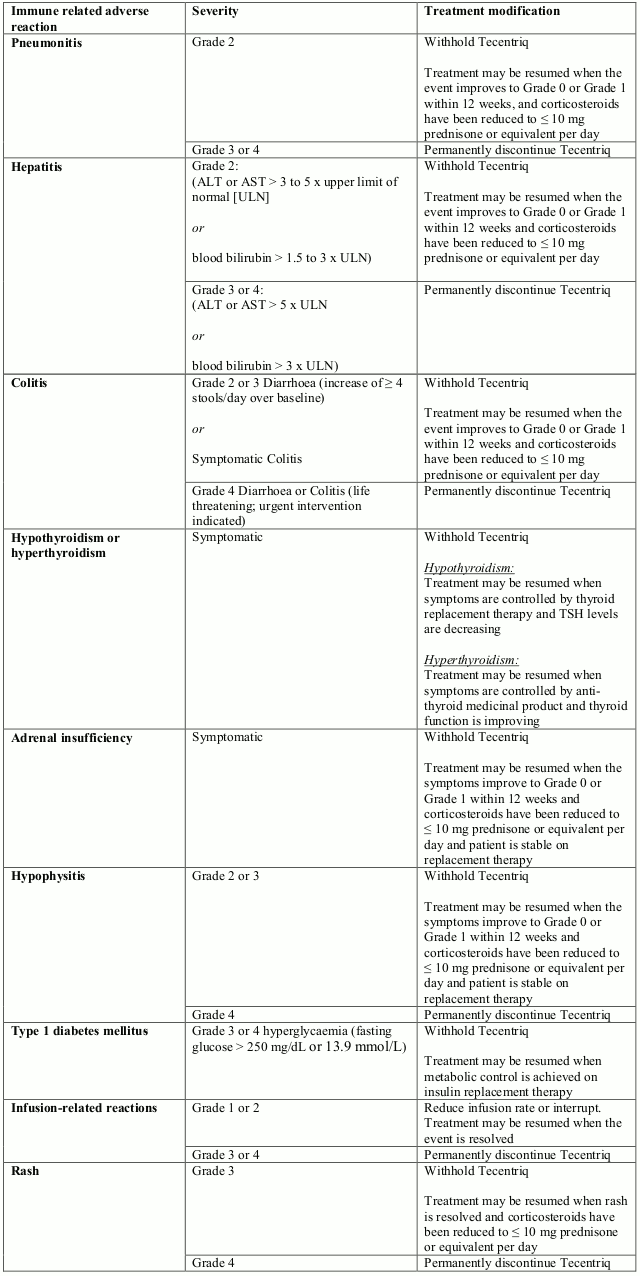
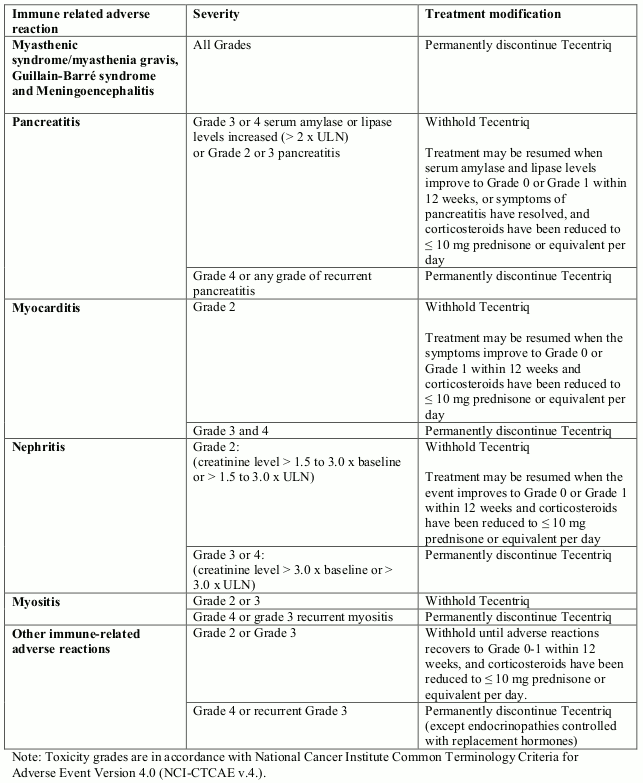
Table 1. Dose modification advice for Tecentriq:
The safety and efficacy of Tecentriq in children and adolescents aged below 18 years have not been established. No data are available.
Based on a population pharmacokinetic analysis, no dose adjustment of Tecentriq is required in patients ≥65 years of age (see sections 4.8 and 5.1).
Due to increased haematologic toxicities observed in Asian patients in IMpower150, it is recommended that the starting dose of paclitaxel should be 175 mg/m² every three weeks.
Based on a population pharmacokinetic analysis, no dose adjustment is required in patients with mild or moderate renal impairment (see section 5.2). Data from patients with severe renal impairment are too limited to draw conclusions on this population.
Based on a population pharmacokinetic analysis, no dose adjustment is required for patients with mild hepatic impairment. Tecentriq has not been studied in patients with moderate or severe hepatic impairment (see section 5.2).
Patients with ECOG performance status ≥2 were excluded from the clinical trials in NSCLC, ES-SCLC and 2nd line UC (see sections 4.4 and 5.1).
Tecentriq is for intravenous use. The infusions must not be administered as an intravenous push or bolus.
The initial dose of Tecentriq must be administered over 60 minutes. If the first infusion is well tolerated, all subsequent infusions may be administered over 30 minutes.
For instructions on dilution and handling of the medicinal product before administration, see section 6.6.
There is no information on overdose with atezolizumab.
In case of overdose, patients should be closely monitored for signs or symptoms of adverse reactions, and appropriate symptomatic treatment instituted.
Unopened vial: 3 years.
Diluted solution: Chemical and physical in-use stability has been demonstrated for up to 24 hours at ≤30°C and for up to 30 days at 2°C to 8°C from the time of preparation.
From a microbiological point of view, the prepared solution for infusion should be used immediately. If not used immediately, in-use storage times and conditions prior to use are the responsibility of the user and would normally not be longer than 24 hours at 2°C to 8°C or 8 hours at ambient temperature (≤25°C) unless dilution has taken place in controlled and validated aseptic conditions.
Store in a refrigerator (2°C–8°C).
Do not freeze.
Keep the vial in the outer carton in order to protect from light.
For storage conditions after dilution of the medicinal product, see section 6.3.
Type I glass vial with a butyl rubber stopper and an aluminium seal with a plastic aqua flip-off cap containing 20 mL of concentrate solution for infusion.
Pack of one vial.
Tecentriq does not contain any antimicrobial preservative or bacteriostatic agents and should be prepared by a healthcare professional using aseptic technique to ensure the sterility of prepared solutions.
Aseptic handling must be ensured when preparing the infusion. Preparation should be:
Do not shake.
Twenty mL of Tecentriq concentrate should be withdrawn from the vial and diluted into a 250 mL polyvinyl chloride (PVC), polyolefin (PO), polyethylene (PE) or polypropylene (PP) infusion bag containing sodium chloride 9 mg/mL (0.9%) solution for injection. After dilution, one mL of solution should contain approximately 4.4 mg of Tecentriq (1,200 mg/270 mL). The bag should be gently inverted to mix the solution in order to avoid foaming. Once the infusion is prepared it should be administered immediately (see section 6.3).
Parenteral medicinal products should be inspected visually for particulates and discolouration prior to administration. If particulates or discoloration are observed, the solution should not be used.
No incompatibilities have been observed between Tecentriq and intravenous bags with product-contacting surfaces of polyvinyl chloride (PVC), polyolefin (PO), polyethylene (PE), or polypropylene (PP). In addition, no incompatibilities have been observed with in-line filter membranes composed of polyethersulfone or polysulfone, and infusion sets and other infusion aids composed of PVC, PE, polybutadiene, or polyetherurethane. The use of in-line filter membranes is optional.
Do not co-administer other medicinal products through the same infusion line.
The release of Tecentriq in the environment should be minimised. Any unused medicinal product or waste material should be disposed of in accordance with local requirements.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.