Source: European Medicines Agency (EU) Revision Year: 2020 Publisher: Amgen Europe B.V., Minervum 7061, NL-4817 ZK Breda, The Netherlands
Pharmacotherapeutic group: Antineoplastic agents
ATC code: L01XX45
Carfilzomib is a tetrapeptide epoxyketone proteasome inhibitor that selectively and irreversibly binds to the N terminal threonine containing active sites of the 20S proteasome, the proteolytic core particle within the 26S proteasome, and displays little to no activity against other protease classes. Carfilzomib had antiproliferative and proapoptotic activities in preclinical models in haematologic tumours. In animals, carfilzomib inhibited proteasome activity in blood and tissue and delayed tumour growth in models of multiple myeloma. In vitro, carfilzomib was found to have minimal neurotoxicity and minimal reaction to non-proteasomal proteases.
Intravenous carfilzomib administration resulted in suppression of proteasome chymotrypsin-like (CT-L) activity when measured in blood 1 hour after the first dose. Doses of ≥15 mg/m² consistently induced an (≥80%) inhibition of the CT-L activity of the proteasome. In addition, carfilzomib administration resulted in inhibition of the latent membrane protein 2 (LMP2) and multicatalytic endopeptidase complex-like 1 (MECL1) subunits of the immunoproteasome ranging from 26% to 32% and 41% to 49%, respectively, at 20 mg/m². Proteasome inhibition was maintained for ≥48 hours following the first dose of carfilzomib for each week of dosing. Combination dosing with lenalidomide and dexamethasone did not affect proteasome inhibition.
At the higher dose of 56 mg/m², there was not only a greater inhibition of CT-L subunits (≥90%) compared to those at 15 to 20 mg/m², but also a greater inhibition of other proteasome subunits (LMP7, MECL1, and LMP2). There was an approximately 8%, 23% and 34% increase in the inhibition of LMP7, MECL1, and LMP2 subunits respectively at the dose of 56 mg/m² compared to those at 15 to 20 mg/m². Similar proteasome inhibition by carfilzomib was achieved with 2 to 10 minute and 30 minute infusions at the 2 dose levels (20 and 36 mg/m²) at which it was tested.
The safety and efficacy of Kyprolis were evaluated in a randomised, open-label, multicentre study of 792 patients with relapsed multiple myeloma, which evaluated the combination of Kyprolis with lenalidomide and dexamethasone versus lenalidomide and dexamethasone alone, randomised 1:1.
This study evaluated Kyprolis at an initial dose of 20 mg/m², which was increased to 27 mg/m² on cycle 1, day 8, administered twice weekly for 3 out of 4 weeks as a 10 minute infusion. Kyprolis treatment was administered for a maximum of 18 cycles unless discontinued early for disease progression or unacceptable toxicity. Lenalidomide and dexamethasone administration could continue until progression or unacceptable toxicity.
Patients who had the following were excluded from the trial: creatinine clearance rates <50 mL/min, NYHA Class III to IV congestive heart failure, or myocardial infarction within the last 4 months, disease progression during the treatment with a bortezomib-containing regimen, or progression during the first 3 months of initiating treatment with lenalidomide and dexamethasone, or progression at any time during treatment with lenalidomide and dexamethasone if this was the subject’s most recent line of therapy. Study eligibility criteria allowed a small subset of patients with myeloma refractory to bortezomib (n=118) or lenalidomide (n=57) to be enrolled. Enrolled subjects were defined as refractory to a therapy if they met any of the following 3 criteria: nonresponsive (< minimal response) to any regimen; progression during any regimen; or progression within 60 days of completion of any regimen. This study did not evaluate the benefit/risk ratio in the broader refractory population.
The disease status and other baseline characteristics were well-balanced between the two arms, including age (64 years, range 31-91 years), gender (56% male), ECOG performance status (48% with performance status 1), high-risk genetic mutations, consisting of the genetic subtypes t(4;14), t(14;16), or deletion 17p in ≥60% of plasma cells (13%), unknown-risk genetic mutations, which included subjects with results not collected or not analysed (47%), and baseline ISS stage III disease (20%). Subjects had received 1 to 3 prior lines of therapy (median of 2), including prior treatment with bortezomib (66%), thalidomide (44%) and lenalidomide (20%).
The results of study PX-171-009 are summarised in table 6 and in figure 1 and figure 2.
Table 6. Summary of efficacy analysis in relapsed multiple myeloma study PX-171-009:
| KRd combination therapy | ||
|---|---|---|
| KRd arma (N=396) | Rd arma (N=396) | |
| PFS months median (95% CI) | 26.3 (23.3, 30.5) | 17.6 (15.0, 20.6) |
| HR (95% CI), 1-sided p-valueb | 0.69 (0.57, 0.83); <0.0001 | |
| Διάμεση OS, μήνες (95% CI) | 48.3 (42.4, 52.8) | 40.4 (33.6, 44.4) |
| HR (95% CI), 1-sided p-valueb | 0.79 (0.67, 0.95); 0.0045 | |
| ORR n (%) | 345 (87.1) | 264 (66.7) |
| sCR | 56 (14.1) | 17 (4.3) |
| CR | 70 (17.7) | 20 (5.1) |
| VGPR | 151 (38.1) | 123 (31.1) |
| PR | 68 (17.2) | 104 (26.3) |
| 95% CI of ORR | 83.4, 90.3 | 61.8, 71.3 |
| 1-sided p-value | <0.0001 | |
KRd = Kyprolis, lenalidomide and dexamethasone; Rd = lenalidomide and dexamethasone; PFS = progression-free survival; HR = hazard ratio; CI = confidence interval; OS = overall survival; ORR = overall response rate; sCR = stringent complete response; CR = complete response; VGPR = very good partial response; PR = partial response; IMWG = international myeloma working group; EBMT = European society for blood and marrow transplantation
a As determined by an Independent Review Committee using standard objective IMWG/EBMT response criteria
b Statistically significant
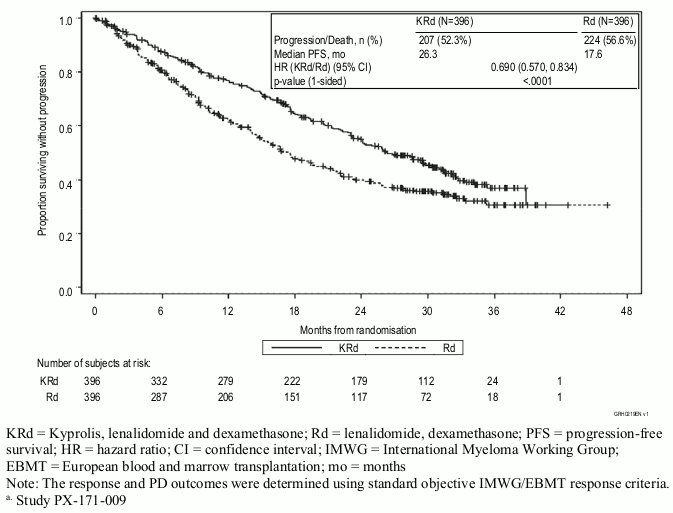
Patients in the Kyprolis, lenalidomide, and dexamethasone (KRd) arm demonstrated improved progression-free survival (PFS) compared with those in the lenalidomide and dexamethasone (Rd) arm, (HR=0.69, with 1-sided p value <0.0001) which represents a 45% improvement in PFS or a 31% reduction in the risk of event as determined using standard objective International Myeloma Working Group (IMWG)/European Blood and Marrow Transplantation (EBMT) response criteria by an Independent Review Committee (IRC).
The PFS benefit of KRd was consistently observed in all subgroups, including patients ≥75 years of age (n=96), patients with high risk (n=100) or unknown (n=375) risk genetic mutations, and patients with baseline creatinine clearance of 30 - <50 mL/min (n=56).
Figure 1. Kaplan-Meier curve of progression-free survival in relapsed multiple myelomaa:
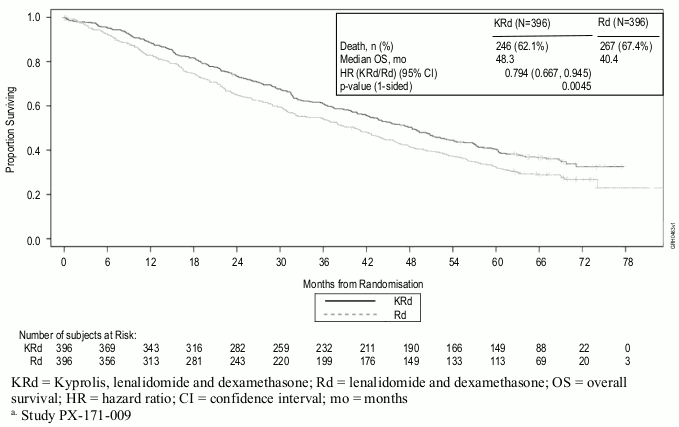
A pre-planned overall survival (OS) analysis was performed after 246 deaths in the KRd arm and 267 deaths in the Rd arm. The median follow-up was approximately 67 months. A statistically significant advantage in OS was observed in patients in the KRd arm compared to patients in the Rd arm. Patients in the KRd arm had a 21% reduction in the risk of death compared with those in the Rd arm (HR=0.79; 95% CI: 0.67, 0.95; p value=0.0045). The median OS improved by 7.9 months in patients in the KRd arm compared with those in the Rd arm (see Table 6 and Figure 2).
Figure 2. Kaplan-Meier curve of overall survival in relapsed multiple myelomaa:
Patients treated with KRd reported improved Global Health Status, with higher Global Health Status/Quality of Life (QoL) scores compared with Rd over 18 cycles of treatment (multiplicity unadjusted 1-sided p-value=0.0001) measured with the EORTC QLQ-C30, an instrument validated in multiple myeloma.
The safety and efficacy of Kyprolis were evaluated in a phase 3, randomised, open-label, multicentre study of Kyprolis plus dexamethasone (Kd) versus bortezomib plus dexamethasone (Vd). A total of 929 patients with relapsed or refractory multiple myeloma who had received 1 to 3 prior lines of therapy were enrolled and randomised (464 in the Kd arm; 465 in the Vd arm).
This study evaluated Kyprolis at an initial dose of 20 mg/m², which was increased to 56 mg/m² on cycle 1, day 8, administered twice weekly for 3 out of 4 weeks as a 30 minute infusion until progression or unacceptable toxicity.
Patients randomised to the Vd arm could receive bortezomib either by the intravenous (n=108) or subcutaneous (n=357) route. Patients who had the following were excluded from the trial: creatinine clearance rates <15 mL/min, NYHA Class III to IV congestive heart failure, myocardial infarction within the last 4 months or those with left ventricular ejection fraction (LVEF) <40%. Study eligibility criteria allowed patients previously treated with carfilzomib (n=3) or bortezomib (n=502) to be enrolled as long as patients had at least a partial response (PR) to prior proteasome inhibitor therapy, were not removed from proteasome inhibitor therapy due to toxicity, and had at least a 6-month proteasome inhibitor treatment-free interval from last dose.
The demographics and baseline characteristics for study 2011-003 were well-balanced between the two arms, including prior treatment with bortezomib (54%), prior treatment with lenalidomide (38%), lenalidomide refractory (25%), age (65 years, range 30-89 years), gender (51% male), ECOG performance status (45% with performance status 1), high risk genetic mutations, consisting of the genetic subtypes t(4;14) or t(14;16) in 10% or more of screened plasma cells, or deletion 17p in ≥20% of plasma cells (23%) unknown-risk genetic mutations, which included subjects with results not collected or not analysed (9%) and baseline ISS stage III disease (24%).
The results of study 2011-003 are summarised in table 7.
Table 7. Summary of efficacy analysis in relapsed multiple myeloma study 2011-003:
| Kd Arm (N=464) | Vd Arm (N=465) | |
|---|---|---|
| PFS months median (95% CI)a | 18.7 (15.6, NE) | 9.4 (8.4, 10.4) |
| HR (95% CI); 1-sided p-valueb | 0.533 (0.44, 0.65); <0.0001 | |
| Overall survival months median (95% CI) | 47.6 (42.5, NE) | 40.0 (32.6, 42.3) |
| HR (95% CI); 1-sided p-valueb | 0.791 (0.65, 0.96); 0.010 | |
| ORR n (%)a,c | 357 (76,9) | 291 (62.6) |
| ≥CRd | 58 (12.5) | 29 (6.2) |
| ≥VGPRe | 252 (54.3) | 133 (28.6) |
| 95% CI of ORR | 72.8, 80.7 | 58.0, 67.0 |
| 1-sided p-valueb | <0.0001 | |
Kd = Kyprolis plus dexamethasone; Vd = bortezomib and dexamethasone; CI = confidence interval; NE = not estimable; HR = Hazard Ratio; ORR = overall response rate; CR = complete response; VGPR = very good partial response
a These endpoints were determined by an Independent Review Committee
b Statistically significant
c Overall response is defined as achieving a best overall response of PR, VGPR, CR, or sCR
d Statistically significant, 1-sided p value=0.0005
e Statistically significant, 1-sided p value=0.0001
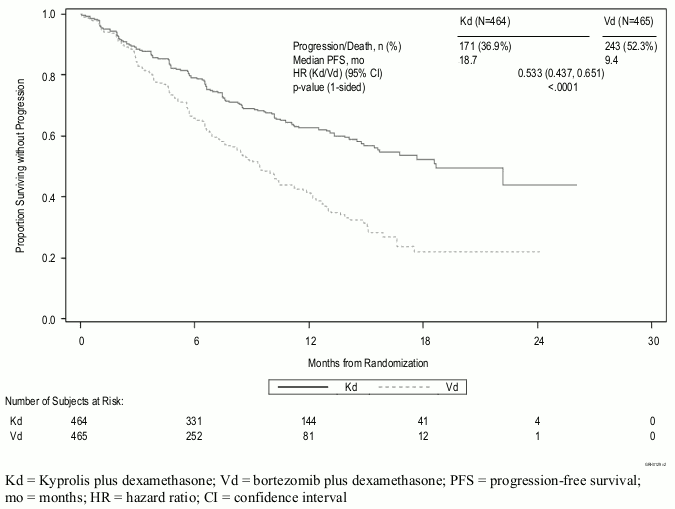
The study showed significant improvement in PFS for patients in the Kd arm over those in the Vd arm (HR: 0.53, 95% CI: 0.44, 0.65 [p value<0.0001]) (see figure 3).
Similar PFS results were observed in patients who had received prior treatment with bortezomib (HR 0.56, 95% CI: 0.44, 0.73) and patients who had not received prior treatment with bortezomib (HR 0.48, 95% CI: 0.36, 0.66).
The PFS benefit of Kd was consistently observed in all subgroups, including patients ≥75 years of age (n=143), patients with high risk (n=210) genetic mutations, and patients with baseline creatinine clearance of 30 - <50 mL/min (n=128).
In patients who received prior bortezomib (54%), median PFS was 15.6 months in the Kd arm versus 8.1 months in the Vd arm (HR=0.56, 95% CI: 0.44, 0.73), ORR was 71.2% versus 60.3%.
In patients who received prior lenalidomide (38%), median PFS was 12.9 months in the Kd arm versus 7.3 months in the Vd arm (HR=0.69, 95% CI: 0.52, 0.92), ORR was 70.1% versus 59.3%. In patients refractory to lenalidomide (25%), median PFS was 8.6 months in the Kd arm versus 6.6 months in the Vd arm (HR=0.80, 95% CI: 0.57, 1.11), ORR was 61.9% versus 54.9%.
Figure 3. Kaplan-Meier plot of progression-free survival as determined by the IRC (intent-to-treat population) study 2011-003:
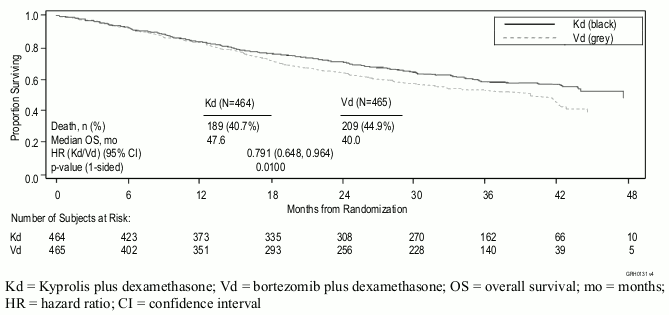
A pre-planned second interim OS analysis was performed after 189 deaths in the Kd arm and 209 deaths in the Vd arm. At the time of the analysis, 80% of the targeted events were registered. The median follow-up was approximately 37 months. A statistically significant advantage in OS was observed in patients in the Kd arm compared to patients in the Vd arm (HR=0.791; 95% CI: 0.65, 0.96; p-value=0.010) (see figure 4).
Figure 4. Kaplan-Meier curve of overall survival in relapsed multiple myeloma study 2011-003:
Additional clinical experience has been generated with Kyprolis monotherapy in patients with relapsed and refractory multiple myeloma. Study PX-171-011 was an open-label randomised phase 3 study (N=315; exposure to ≥3 prior therapies required). Patients enrolled to study PX-171-011 were more heavily pre-treated with lower organ and marrow function as compared to those enrolled in study PX-171-009. PX-171-011 evaluated Kyprolis monotherapy versus a control arm (corticosteroids and cyclophosphamide). The study did not meet its primary efficacy endpoint of demonstrating superiority of Kyprolis monotherapy over the active control arm in overall survival (HR=0.975 [95% CI: 0.760-1.249]). PX-171-003A1 was a single-arm phase 2 study (N=266; exposure to ≥2 prior therapies required), which met its primary efficacy endpoint of IRC-assessed ORR (22.9%).
An evaluation of possible effects of carfilzomib on cardiac function was performed by analysing, via central blind reading, triplicate ECG in 154 subjects with advanced malignancies, including multiple myeloma. The effect of carfilzomib on cardiac repolarisation using the QT interval with Fridericia’s correction (QTcF interval) and the analysis of concentration-QTc relationships show no clear signal of any dose-related effect. The upper bound of one-sided 95% confidence interval (CI) for predicted effect on QTcF at Cmax was 4.8 msec. With Bazett’s correction (QTcB interval), the upper bound of one-sided 95% confidence interval (CI) for predicted effect on QTcB at Cmax was 5.9 msec.
The European Medicines Agency has waived the obligation to submit the results of studies with Kyprolis in all subsets of the paediatric population in multiple myeloma (see section 4.2 for information on paediatric use).
The Cmax and AUC following a 2 to 10 minute intravenous infusion of 27 mg/m² was 4,232 ng/mL and 379 ng•hr/mL, respectively. Following repeated doses of Kyprolis at 15 and 20 mg/m², systemic exposure (AUC) and half-life were similar on days 1 and 15 or 16 of cycle 1, suggesting there was no systemic carfilzomib accumulation. At doses between 20 and 56 mg/m², there was a dose-dependent increase in exposure.
A 30 minute infusion resulted in a similar half-life and AUC, but 2- to 3-fold lower Cmax compared to that observed with a 2 to 10 minute infusion of the same dose. Following a 30 minute infusion of the 56 mg/m² dose, the AUC (948 ng•hr/mL) was approximately 2.5-fold that observed at the 27 mg/m² level, and Cmax (2,079 ng/mL) was lower compared to that of 27 mg/m² over the 2 to 10 minute infusion.
The mean steady-state volume of distribution of a 20 mg/m² dose of carfilzomib was 28 L. When tested in vitro, the binding of carfilzomib to human plasma proteins averaged 97% over the concentration range of 0.4 to 4 micromolar.
Carfilzomib was rapidly and extensively metabolised. The predominant metabolites measured in human plasma and urine, and generated in vitro by human hepatocytes, were peptide fragments and the diol of carfilzomib, suggesting that peptidase cleavage and epoxide hydrolysis were the principal pathways of metabolism. Cytochrome P450 mediated mechanisms played a minor role in overall carfilzomib metabolism. The metabolites have no known biologic activity.
Following intravenous administration of doses ≥15 mg/m², carfilzomib was rapidly cleared from the systemic circulation with a half-life of ≤1 hour on day 1 of cycle 1. The systemic clearance ranged from 151 to 263 L/hour, and exceeded hepatic blood flow, suggesting that carfilzomib was largely cleared extrahepatically. Carfilzomib is eliminated primarily via metabolism with subsequent excretion of its metabolites in urine.
Population pharmacokinetic analyses indicate there are no effects of age, gender or race on the pharmacokinetics of carfilzomib.
A pharmacokinetic study evaluated 33 patients with relapsed or progressive advanced malignancies (solid tumours; n=31 or haematologic malignancies; n=2) who had normal hepatic function (bilirubin ≤ upper limit of normal [ULN]; aspartate aminotransferase [AST] ≤ ULN, n=10), mild hepatic impairment (bilirubin >1-1.5 x ULN or AST > ULN, but bilirubin ≤ ULN, n=14), or moderate hepatic impairment (bilirubin >1.5-3 x ULN; any AST, n=9). The pharmacokinetics of carfilzomib has not been studied in patients with severe hepatic impairment (bilirubin >3 x ULN and any AST). Kyprolis, as a single agent, was administered intravenously over 30 minutes at 20 mg/m² on days 1 and 2 and at 27 mg/m² on days 8, 9, 15 and 16 of cycle 1. If tolerated, patients received 56 mg/m² starting in cycle 2. Baseline hepatic function status had no marked effect on the total systemic exposure (AUClast) of carfilzomib following single or repeat-dose administration (geometric mean ratio in AUClast at the 27 mg/m² dose in cycle 1, day 16 for mild and moderate impairment versus normal hepatic function were 144.4% and 126.1%, respectively; and at the 56 mg/m² dose in cycle 2, day 1 were 144.7% and 121.1%). However, in patients with mild or moderate baseline hepatic impairment, all of whom had solid tumours, there was a higher subject incidence of hepatic function abnormalities, ≥ grade 3 adverse events and serious adverse events compared with subjects with normal hepatic function (see section 4.2).
The pharmacokinetics of carfilzomib was studied in two dedicated renal impairment studies.
The first study was conducted in 50 multiple myeloma patients with normal renal function (CrCL >80 mL/min, n=12), mild (CrCL 50-80 mL/min, n=12), moderate (CrCL 30-49 mL/min, n=10), and severe (CrCL <30 mL/min, n=8) renal impairment, and patients on chronic dialysis (n=8). Kyprolis, as a single agent, was administered intravenously over 2 to 10 minutes at doses up to 20 mg/m². Pharmacokinetic data were collected from patients following the 15 mg/m² dose in cycle 1 and the 20 mg/m² dose in cycle 2. The second study was conducted in 23 relapsed multiple myeloma patients with creatinine clearance ≥75 mL/min (n=13) and patients with end stage renal disease (ESRD) requiring dialysis (n=10). Pharmacokinetic data were collected from patients following administration of a 27 mg/m² dose as a 30 minute infusion on cycle 1, day 16 and the 56 mg/m² dose on cycle 2, day 1.
Results from both studies show that renal function status had no marked effect on the exposure of carfilzomib following single or repeat-dose administration. The geometric mean ratio in AUClast at the 15 mg/m² dose cycle 1, day 1 for mild, moderate, severe renal impairment and chronic dialysis versus normal renal function were 124.36%, 111.07%, 84.73% and 121.72%, respectively. The geometric mean ratios in AUClast at the 27 mg/m² dose cycle 1, day 16 and at the 56 mg/m² dose cycle 2, day 1 for ESRD versus normal renal function were 139.72% and 132.75%, respectively. In the first study the M14 metabolite, a peptide fragment and the most abundant circulating metabolite, increased 2- and 3-fold in patients with moderate and severe renal impairment, respectively, and 7-fold in patients requiring dialysis (based on AUClast). In the second study, the exposures for M14 were greater (approximately 4-fold) in subjects with ESRD than in subjects with normal renal function. This metabolite has no known biological activities. Serious adverse events related to worsening renal function were more common in subjects with baseline renal dysfunction (see section 4.2).
Carfilzomib was clastogenic in the in vitro chromosomal aberration test in peripheral blood lymphocytes. Carfilzomib was not mutagenic in the in vitro bacterial reverse mutation (Ames) test and was not clastogenic in the in vivo mouse bone marrow micronucleus assay.
Monkeys administered a single bolus intravenous dose of carfilzomib at 3 mg/kg (which corresponds to 36 mg/m² and is similar to the recommended dose in humans of 27 mg/m² based on BSA) experienced hypotension, increased heart rate, and increased serum levels of troponin T. The repeated bolus intravenous administration of carfilzomib at ≥2 mg/kg/dose in rats and 2 mg/kg/dose in monkeys using dosing schedules similar to those used clinically resulted in mortalities that were due to toxicities occurring in the cardiovascular (cardiac failure, cardiac fibrosis, pericardial fluid accumulation, cardiac haemorrhage/degeneration), gastrointestinal (necrosis/haemorrhage), renal (glomerulonephropathy, tubular necrosis, dysfunction), and pulmonary (haemorrhage/inflammation) systems. The dose of 2 mg/kg/dose in rats is approximately half the recommended dose in humans of 27 mg/m² based on BSA. The highest non-severely toxic dose of 0.5 mg/kg in monkeys resulted in interstitial inflammation in the kidney along with slight glomerulopathy and slight heart inflammation. Those findings were reported at 6 mg/m 2 which are below the recommended dose in humans of 27 mg/m².
Fertility studies with carfilzomib have not been conducted. No effects on reproductive tissues were noted during 28-day repeat-dose rat and monkey toxicity studies or in 6-month rat and 9-month monkey chronic toxicity studies. Carfilzomib caused embryo-foetal toxicity in pregnant rabbits at doses that were lower than in patients receiving the recommended dose. Carfilzomib administered to pregnant rats during the period of organogenesis was not teratogenic at doses up to 2 mg/kg/day, which is approximately half the recommended dose in humans of 27 mg/m² based on BSA.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.