CARDURA XL Extended-release tablet Ref.[10543] Active ingredients: Doxazosin
Source: FDA, National Drug Code (US) Revision Year: 2019
12.1. Mechanism of Action
The symptoms associated with benign prostatic hyperplasia (BPH), such as urinary frequency, nocturia, weak stream, hesitancy, and incomplete emptying are related to two components, anatomical (static) and functional (dynamic). The static component is related to an increase in prostate size caused, in part, by a proliferation of smooth muscle cells in the prostatic stroma. However, the severity of BPH symptoms and the degree of urethral obstruction do not correlate well with the size of the prostate. The dynamic component of BPH is associated with an increase in smooth muscle tone in the prostate and bladder neck. The degree of tone in this area is mediated by the alpha1 adrenoceptor, which is present in high density in the prostatic stroma, prostatic capsule, and bladder neck. Blockade of the alpha1 receptor decreases urethral resistance and may relieve the BPH symptoms and improve urine flow. Doxazosin mesylate is a selective inhibitor of the alpha1-subtype of alpha adrenergic receptors. In the human prostate, doxazosin mesylate antagonizes phenylephrine (alpha1 agonist)-induced contractions, in vitro, and binds with high affinity to the alpha1A adrenoceptor.
12.2. Pharmacodynamics
Administration of CARDURA XL to patients with symptomatic BPH resulted in a statistically significant improvement in maximum urinary flow rate [see Clinical Studies (14.1)].
12.3. Pharmacokinetics
The pharmacokinetics of CARDURA XL is different from that of doxazosin IR. CARDURA XL provides a controlled release of doxazosin over a 24-hour period.
Absorption
Pharmacokinetic parameters describing absorption following 4 and 8 mg CARDURA XL daily doses are reported in Table 2 below. The relative bioavailability of CARDURA XL compared with doxazosin IR was 54% at the 4 mg dose and 59% for the 8 mg dose.
TABLE 2. Mean (±SD) Plasma Concentration of Doxazosin at Steady State in Healthy Volunteers: Pharmacokinetic Parameters:
| Parameter | CARDURA XL (4 mg) | CARDURA XL (8 mg) |
|---|---|---|
| Cmax(ng/mL) | 10.1 ± 5.6 | 25.8 ± 12.1 |
| AUC(0–∞) | 183 ± 85.5 | 472 ± 170.8 |
| Tmax(h) | 8 ± 3.7 | 9 ± 4.7 |
Food Effect
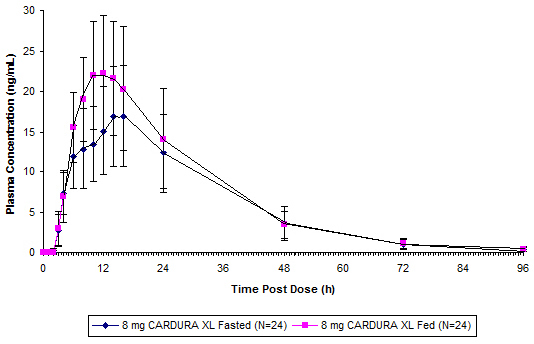
As illustrated in Figure 1, the plasma Cmax and AUC were approximately 32% and 18% higher, respectively, after CARDURA XL was administered in the fed state compared with the fasted state. In order to provide the most consistent exposure, CARDURA XL should be administered with breakfast [see Dosage and Administration (2.1)].
Figure 1. Mean (+SD) Plasma Concentration of Doxazosin Following Single Oral Doses of 8 mg CARDURA XL (Fed and Fasted):
GI Retention Time Effect
Markedly reduced GI retention times (e.g., short bowel syndrome) may influence the pharmacokinetics of CARDURA XL and possibly result in lower plasma concentrations. Conversely, markedly prolonged GI retention times (e.g., chronic constipation) can increase systemic exposure to doxazosin and potentially result in increased adverse reactions [see Warnings and Precautions (5.3)].
Distribution
At the plasma concentrations achieved by therapeutic doses, approximately 98% of the circulating drug is bound to plasma proteins.
Metabolism
Doxazosin is extensively metabolized in the liver. In vitro studies suggest that the primary pathway for elimination is via CYP 3A4; however, CYP 2D6 and CYP 2C9 metabolic pathways also exist to a lesser extent. No in vivo drug interaction studies have been performed with CARDURA XL. Although several active metabolites of doxazosin have been identified, the pharmacokinetics of these metabolites has not been characterized [see Drug Interactions (7)].
Excretion
In a study of two subjects administered radiolabeled doxazosin IR 2 mg orally and 1 mg intravenously on two separate occasions, approximately 63% of the dose was eliminated in the feces and 9% of the dose was found in the urine. On average, only 4.8% of the dose was excreted as unchanged drug in the feces and only a trace of the total radioactivity in the urine was attributed to unchanged drug. The apparent elimination half-life of CARDURA XL is 15–19 hours.
Drug-Drug Interactions
No in vivo drug-drug interaction studies have been performed to assess the effect of concomitant medications on the pharmacokinetics of CARDURA XL or to assess the effect of CARDURA XL on the pharmacokinetics of other drugs. In vitro studies suggest that doxazosin is a substrate of CYP 3A4. Caution should be exercised when concomitantly administering CARDURA XL with a strong CYP 3A4 inhibitor, such as atanazavir, clarithromycin, indinavir, itraconazole, ketoconazole, nefazodone, nelfinavir, ritonavir, saquinavir, telithromycin, or voriconazole
In one placebo-controlled trial in normal volunteers, the administration of a single 1 mg dose of doxazosin IR on day 1 of a four day regimen of cimetidine (400 mg twice daily) resulted in a 10% increase in the mean AUC of doxazosin, a 6% increase in mean Cmax of doxazosin, and no significant change in mean half-life of doxazosin. Based upon the differences in dose and formulation, the applicability of these results to CARDURA XL is unknown. Otherwise, the interaction potential with other inhibitors or substrates of CYP enzymes has not been determined. Pharmacodynamic interactions between CARDURA XL and anti-hypertensive medications or other vasodilating agents have also not been determined. Finally, drugs which reduce gastrointestinal motility leading to markedly prolonged GI retention times (e.g., anticholinergic agents) may increase systemic exposure to doxazosin.
Use in Specific Populations
Geriatric
In a study to assess the effect of age on the pharmacokinetics of CARDURA XL, increases of 27% in plasma Cmax and 34% in the plasma AUC were seen at steady state in the elderly (>65 years old) compared to the young [see Use in Specific Populations (8.5)].
Hepatic Impairment
Administration of a single 2 mg dose of doxazosin IR to patients with mild hepatic impairment (Child-Pugh Class A) showed a 40% increase in exposure to doxazosin compared to patients without hepatic impairment. No studies have been performed to assess the effect of hepatic impairment on the pharmacokinetics of CARDURA XL. Use in patients with severe hepatic impairment is not recommended. CARDURA XL should be administered with caution to patients with evidence of mild or moderately impaired hepatic function or to patients receiving drugs known to influence hepatic metabolism.
13.1. Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis and Mutagenesis
Doxazosin mesylate was not carcinogenic to rats or mice when administered daily for 2 years at doses up to 40 mg/kg/day or 120 mg/kg/day, respectively. Systemic drug exposures, as measured by AUC, were approximately 34-fold in rats and 16-fold in mice above the exposures at the maximum human recommended dose (MHRD) of 8 mg CARDURA XL.
Doxazosin base was not mutagenic in the in vitro bacterial Ames assays, the chromosomal aberration assay in human lymphocytes, or the mouse lymphoma assay. Doxazosin was not clastogenic in the in vivo mouse micronucleus assay. Doxazosin mesylate has not been evaluated for genotoxicity.
Fertility in Males
Studies in rats after oral administration of doxazosin base showed reduced fertility in males, which was reversible after two weeks of treatment termination at doxazosin base exposure of 13-fold above the human exposure (AUC) at the MHRD of 8 mg CARDURA XL. There have been no reports of any effects of doxazosin on male fertility in humans.
13.2. Animal Toxicology and/or Pharmacology
Studies in Sprague-Dawley rats after 6, 12, and 18 months, and in CD-1 mice after 18 months of dietary administration, showed an increased incidence of myocardial necrosis or fibrosis at doxazosin base exposure of 26-fold above the human exposure (AUC) at the MHRD of 8 mg CARDURA XL. No cardiotoxicity was observed in dogs or Wistar rats after 12 months of oral dosing at doxazosin base exposures of 65- and 85-fold, respectively, above the human exposure (Cmax) at the MHRD of 8 mg CARDURA XL. There is no evidence that similar lesions occur in humans.
14. Clinical Studies
14.1 Studies in Patients with BPH
Two controlled clinical studies were conducted with CARDURA XL in BPH patients, followed by an open-label extension study. Study 1 was a randomized, double-blind, parallel-group, placebo- and active-controlled study that compared the safety and efficacy of CARDURA XL (4 or 8 mg/day) with that of doxazosin IR (1, 2, 4, or 8 mg/day) and placebo over 13 weeks in 795 BPH patients, of whom 317 were randomized to CARDURA XL. Study 2 was a randomized, double-blind, parallel-group, active-controlled study that compared the safety and efficacy of CARDURA XL (4 or 8 mg/day) with that of doxazosin IR (1, 2, 4, or 8 mg/day) over 13 weeks in 680 BPH patients, of whom 350 were randomized to CARDURA XL.
In both studies, men aged 50–80 years with symptomatic benign prostatic hyperplasia (BPH) were enrolled. Symptomatic BPH was defined as a total score of at least 12 points on the 35-point International Prostate Symptom Score (IPSS) and a maximum urinary flow rate of ≤ 15 mL/sec but no less than 5 mL/sec (total voided volume ≥ 150 mL). In these two studies, conducted in a total of 1475 patients, the mean age was 64 years (range 47–83 years). Patients were Caucasian (96%), Black (1.5%), Asian (1.5%), and of Other ethnicity (1%).
In both studies, CARDURA XL dosing was initiated after a 2 week placebo run-in period at 4 mg per day increasing to 8 mg per day after 7 weeks of treatment if adequate response (defined as having both an increase in maximum urinary flow rate of at least 3 mL/sec and a decrease in total IPSS of at least 30% from baseline) was not seen. Doxazosin IR was titrated from an initial dose of 1 mg daily to 2 mg daily after 1 week with the option to increase to 4 mg daily after 3 weeks and then to a maximum of 8 mg daily after 7 weeks if an adequate response was not seen. The final daily dose of CARDURA XL was 4 mg in 43% of patients and 8 mg in 57% of patients. The final daily dose of doxazosin IR was 1 mg in 1%, 2 mg in 12%, 4 mg in 30%, and 8 mg in 57% of patients.
There were two primary efficacy variables in each of these two controlled clinical studies: the total International Prostate Symptom Score (IPSS) and the peak urinary flow rate (Qmax). The IPSS consists of seven questions that assess the severity of both irritative (frequency, urgency, nocturia) and obstructive (incomplete emptying, stopping and starting, weak stream, and pushing or straining) symptoms, with possible total scores ranging from 0 to 35. The Qmax was measured in both studies just prior to the next dose. The results for total symptom score are given in Table 3, and for maximum urinary flow rate in Table 4.
TABLE 3. TOTAL INTERNATIONAL PROSTATE SYMPTOM SCORE (IPSS)*:
| N | MEAN BASELINE (±SD) | MEAN CHANGE (±SE)† | |
|---|---|---|---|
| STUDY 1 | |||
| Placebo | 151 | 17.9 ± 4.3 | -6.1 ± 0.41 |
| CARDURA XL | 310 | 17.7 ± 4.3 | -8.0 ± 0.30‡ |
| Doxazosin IR | 311 | 17.8 ± 4.5 | -8.4 ± 0.29‡ |
| STUDY 2 | |||
| CARDURA XL | 330 | 18.4 ± 5.0 | -8.1 ± 0.30 |
| Doxazosin IR | 313 | 18.4 ± 4.8 | -7.9 ± 0.31 |
* Derived from IPSS questionnaire (range 0–35)
† Mean change from baseline to Week 13
‡ Statistically significant difference (p<0.001) vs. placebo
TABLE 4. MAXIMUM FLOW RATE (mL/sec):
| N | MEAN BASELINE (±SD) | MEAN CHANGE (±SE)* | |
|---|---|---|---|
| STUDY 1 | |||
| Placebo | 151 | 9.8 ± 2.6 | 0.8 ± 0.32 |
| CARDURA XL | 300 | 10.3 ± 2.6 | 2.6 ± 0.24† |
| Doxazosin IR | 303 | 10.1 ± 2.7 | 2.2 ± 0.23† |
| STUDY 2 | |||
| CARDURA XL | 322 | 10.5 ± 2.6 | 2.7 ± 0.27 |
| Doxazosin IR | 314 | 10.6 ± 2.6 | 2.7 ± 0.27 |
* Mean change from baseline to Week 13
† Statistically significant difference (p <0.001) vs. placebo
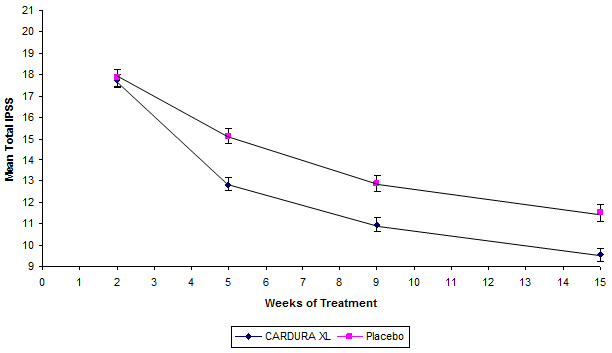
Mean changes in IPSS scores for CARDURA XL and placebo in Study 1 are summarized in Figure 2.
Figure 2. Mean Total IPSS (±SE) by Week in Study 1:
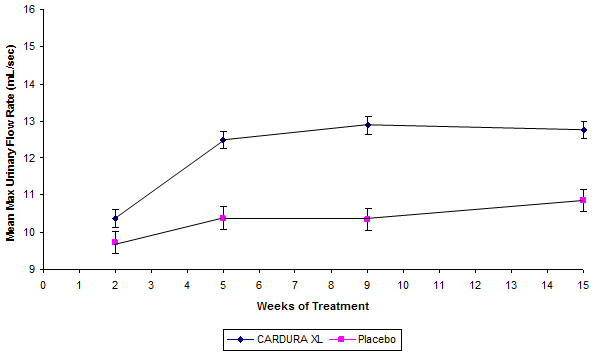
Mean changes in maximum urinary flow rate (Qmax) for both CARDURA XL and placebo in Study 1 are summarized in Figure 3.
Figure 3. Mean Maximum Urinary Flow Rate (mL/sec) (±SE) by Week in Study 1:
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.