AJOVY Solution for injection Ref.[8745] Active ingredients: Fremanezumab
Source: European Medicines Agency (EU) Revision Year: 2020 Publisher: TEVA GmbH, Graf-Arco-Str. 3, 89079 Ulm, Germany
Pharmacodynamic properties
Pharmacotherapeutic group: Not yet assigned
ATC code: Not yet assigned
Mechanism of action
Fremanezumab is a humanised IgG2Δa/kappa monoclonal antibody derived from a murine precursor. Fremanezumab selectively binds the calcitonin gene-related peptide (CGRP) ligand and blocks both CGRP isoforms (α- and β-CGRP) from binding to the CGRP receptor. While the precise mechanism of action by which fremanezumab prevents migraine attacks is unknown, it is believed that prevention of migraine is obtained by its effect modulating the trigeminal system. CGRP levels have been shown to increase significantly during migraine and return to normal with headache relief.
Fremanezumab is highly specific for CGRP and does not bind to closely related family members (e.g., amylin, calcitonin, intermedin and adrenomedullin).
Clinical efficacy and safety
The efficacy of fremanezumab was assessed in two randomised, 12-week, double-blind, placebocontrolled phase III studies in adult patients with episodic (Study 1) and chronic migraine (Study 2). The patients enrolled had at least a 12-month history of migraine (with and without aura) according to the International Classification of Headache Disorders (ICHD-III) diagnostic criteria. Elderly patients (>70 years), patients using opioids or barbiturates on more than 4 days per month, and patients with pre-existing myocardial infarction, cerebrovascular accident, and thromboembolic events were excluded.
Episodic migraine study (Study 1)
The efficacy of fremanezumab was evaluated in episodic migraine in a randomised, multicentre, 12-week, placebo-controlled, double-blind study (Study 1). Adults with a history of episodic migraine (less than 15 headache days per month) were included in the study. A total of 875 patients (742 females, 133 males) were randomised into one of three arms: 675 mg fremanezumab every three months (quarterly, n=291), 225 mg fremanezumab once a month (monthly, n=290), or monthly administration of placebo (n=294) administered via subcutaneous injection. Demographics and baseline disease characteristics were balanced and comparable between the study arms. Patients had a median age of 42 years (range: 18 to 70 years), 85% were female, and 80% were white. The mean migraine frequency at baseline was approximately 9 migraine days per month. Patients were allowed to use acute headache treatments during the study. A sub-set of patients (21%) was also allowed to use one commonly used concomitant, preventive medicinal product (beta-blockers, calcium channel blocker/benzocycloheptene, antidepressants, anticonvulsants). Overall, 19% of the patients had previously used topiramate. A total of 791 patients completed the 12-week double-blind treatment period.
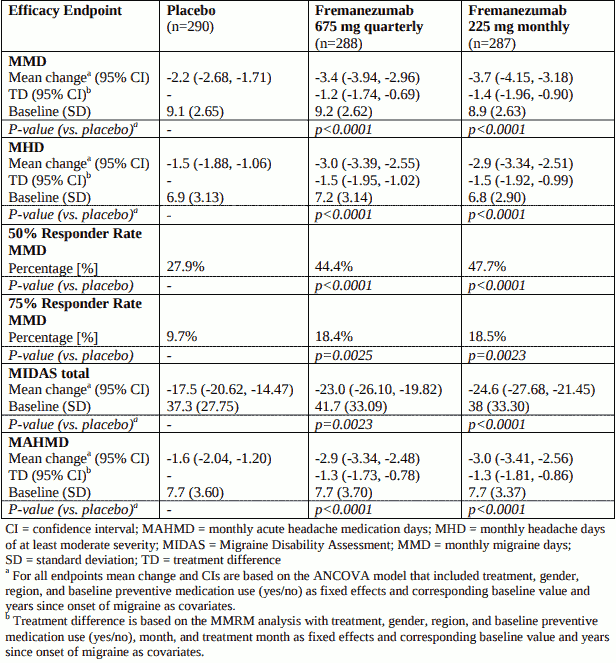
The primary efficacy endpoint was the mean change from baseline in the monthly average number of migraine days during the 12-week treatment period. Key secondary endpoints were the achievement of at least 50% reduction from baseline in monthly migraine days (50% responder rate), mean change from baseline in the patient reported MIDAS score, and change from baseline in monthly average number of days of acute headache medicinal product use. Both monthly and quarterly dosing regimens of fremanezumab demonstrated statistically significant and clinically meaningful improvement from baseline compared to placebo for key endpoints (see Table 2). The effect also occurred from as early as the first month and sustained over the treatment period (see Figure 1).
Figure 1. Mean Change from Baseline in the Monthly Average Number of Migraine Days for Study 1:
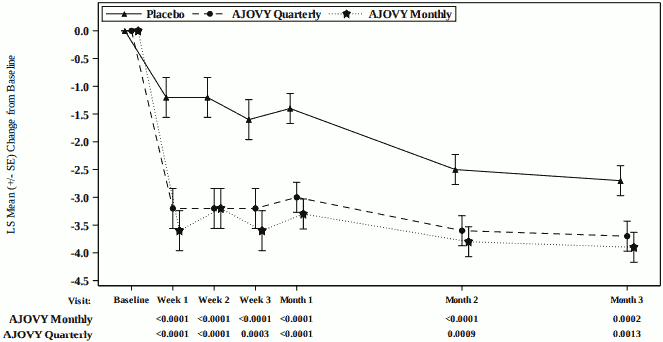
Mean at baseline (monthly average number of migraine days): Placebo: 9.1, AJOVY Quarterly: 9.2, AJOVY Monthly: 8.9.
Table 2. Key Efficacy Outcomes in Study 1 in Episodic Migraine:
In patients on one other concomitant, migraine preventive medicinal product, the treatment difference for the reduction of monthly migraine days (MMD) observed between fremanezumab 675 mg quarterly and placebo was -1.8 days (95% CI: -2.95, -0.55) and between fremanezumab 225 mg monthly and placebo -2.0 days (95% CI: -3.21, -0.86).
In patients who had previously used topiramate the treatment difference for the reduction of monthly migraine days (MMD) observed between fremanezumab 675 mg quarterly and placebo was -2.3 days (95% CI: -3.64, -1.00) and between fremanezumab 225 mg monthly and placebo -2.4 days (95% CI: -3.61, -1.13).
Chronic migraine study (Study 2)
Fremanezumab was evaluated in chronic migraine in a randomised, multicentre, 12-week, placebocontrolled, double-blind study (Study 2). The study population included adults with a history of chronic migraine (15 headache days or higher per month). A total of 1,130 patients (991 females, 139 males) were randomised into one of three arms: 675 mg fremanezumab starting dose followed by 225 mg fremanezumab once a month (monthly, n=379), 675 mg fremanezumab every three months (quarterly, n=376), or monthly administration of placebo (n=375) administered via subcutaneous injection. Demographics and baseline disease characteristics were balanced and comparable between the study arms. Patients had a median age of 41 years (range: 18 to 70 years), 88% were female, and 79% were white. The mean headache frequency at baseline was approximately 21 headache days per month (of which 13 headache days were of at least moderate severity). Patients were allowed to use acute headache treatments during the study. A sub-set of patients (21%) was also allowed to use one commonly used concomitant, preventive medicinal product (beta-blockers, calcium channel blocker/benzocycloheptene, antidepressants, anticonvulsants). Overall, 30% of the patients had previously used topiramate and 15% onabotulinumtoxin A. A total of 1,034 patients completed the 12-week double-blind treatment period.
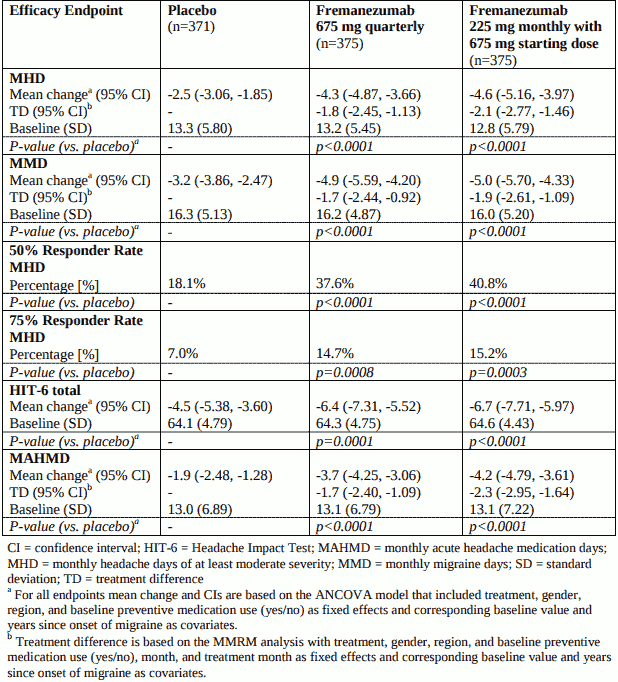
The primary efficacy endpoint was the mean change from baseline in the monthly average number of headache days of at least moderate severity during the 12-week treatment period. Key secondary endpoints were the achievement of at least 50% reduction from baseline in monthly headache days of at least moderate severity (50% responder rate), mean change from baseline in the patient reported HIT-6 score, and change from baseline in monthly average number of days of acute headache medicinal product use. Both monthly and quarterly dosing regimens of fremanezumab demonstrated statistically significant and clinically meaningful improvement from baseline compared to placebo for key endpoints (see Table 3). The effect also occurred from as early as the first month and sustained over the treatment period (see Figure 2).
Figure 2. Mean Change from Baseline in the Monthly Average Number of Headache Days of At Least Moderate Severity for Study 2:
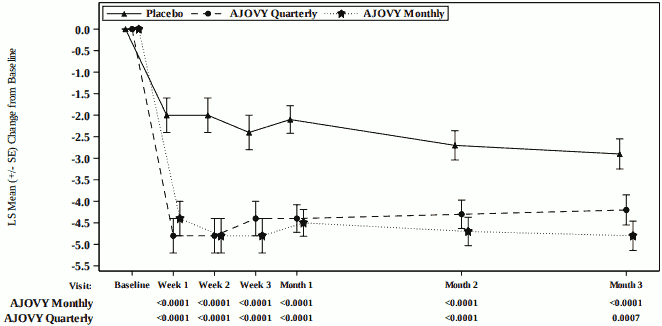
Mean at baseline (monthly average number of headache days of at least moderate severity): Placebo: 13.3, AJOVY Quarterly: 13.2, AJOVY Monthly: 12.8.
Table 3. Key Efficacy Outcomes in Study 2 in Chronic Migraine:
In patients on one other concomitant, migraine preventive medicinal product, the treatment difference for the reduction of monthly headache days (MHD) of at least moderate severity observed between fremanezumab 675 mg quarterly and placebo was -1.3 days (95% CI: -2.66, 0.03) and between fremanezumab 225 mg monthly with 675 mg starting dose and placebo -2.0 days (95% CI: -3.27, -0.67).
In patients who had previously used topiramate the treatment difference for the reduction of monthly headache days (MHD) of at least moderate severity observed between fremanezumab 675 mg quarterly and placebo was -2.7 days (95% CI: -3.88, -1.51) and between fremanezumab 225 mg monthly with 675 mg starting dose and placebo -2.9 days (95% CI: -4.10, -1.78). In patients who had previously used onabotulinumtoxin A the treatment difference for the reduction of monthly headache days (MHD) of at least moderate severity observed between fremanezumab 675 mg quarterly and placebo was -1.3 days (95% CI: -3.01, -0.37) and between fremanezumab 225 mg monthly with 675 mg starting dose and placebo -2.0 days (95% CI: -3.84, -0.22).
Approximately 52% of the patients in the study had acute headache medication overuse. The observed treatment difference for the reduction of monthly headache days (MHD) of at least moderate severity between fremanezumab 675 mg quarterly and placebo in these patients was -2.2 days (95% CI: -3.14, -1.22) and between fremanezumab 225 mg monthly with 675 mg starting dose and placebo -2.7 days (95% CI: -3.71, -1.78).
Long-term study (Study 3)
For all episodic and chronic migraine patients, efficacy was sustained for up to 12 additional months in the long-term study (Study 3), in which patients received 225 mg fremanezumab monthly or 675 mg quarterly. 79% of patients completed the 12-month treatment period of Study 3. Pooled across the two dosing regimens, a reduction of 6.6 monthly migraine days was observed after 15 months relative to Study 1 and Study 2 baseline. 61% of patients completing Study 3 achieved a 50% response in the last month of the study. No safety signal was observed during the 15-month combined treatment period.
Intrinsic and extrinsic factors
The efficacy and safety of fremanezumab was demonstrated regardless of age, gender, race, use of concomitant preventive medicinal products (beta-blockers, calcium channel blocker/benzocycloheptene, antidepressants, anticonvulsants), use of topiramate or onabotulinumtoxin A for migraine in the past, and acute headache medication overuse. There is limited data available on the use of fremanezumab in patients ≥65 years of age (2% of the patients).
Paediatric population
The European Medicines Agency has deferred the obligation to submit the results of studies with AJOVY in one or more subsets of the paediatric population in prevention of migraine headaches (see section 4.2 for information on paediatric use).
Pharmacokinetic properties
Absorption
After single subcutaneous administrations of 225 mg and 675 mg fremanezumab, median time to maximum concentrations (tmax) in healthy subjects was 5 to 7 days. The absolute bioavailability of fremanezumab after subcutaneous administration of 225 mg and 900 mg in healthy subjects was 55% (±SD of 23%) to 66% (±SD of 26%). Dose proportionality, based on population pharmacokinetics, was observed between 225 mg to 675 mg. Steady state was achieved by approximately 168 days (about 6 months) following 225 mg monthly and 675 mg quarterly dosing regimens. Median accumulation ratio, based on once monthly and once quarterly dosing regimens, is approximately 2.4 and 1.2, respectively.
Distribution
Assuming the model-derived estimated bioavailability of 66% (±SD of 26%) holds for the patient population, the volume of distribution for a typical patient was 3.6 L (35.1% CV) following subcutaneous administration of 225 mg, 675 mg and 900 mg of fremanezumab.
Biotransformation
Similar to other monoclonal antibodies, fremanezumab is expected to be degraded by enzymatic proteolysis into small peptides and amino acids.
Elimination
Assuming the model-derived estimated bioavailability of 66% (±SD of 26%) holds for the patient population, central clearance for a typical patient was 0.09 L/day (23.4% CV) following subcutaneous administration of 225 mg, 675 mg and 900 mg of fremanezumab. The formed small peptides and amino acids may be re-used in the body for de novo synthesis of proteins or are excreted by the kidney. Fremanezumab has an estimated half-life of 30 days.
Special populations
A population pharmacokinetic analysis looking at age, race, gender, and weight was conducted on data from 2,546 subjects. Approximately twice as much exposure is expected in the lowest body weight quartile (43.5 to 60.5 kg) compared to the highest body weight quartile (84.4 to131.8 kg). However, body weight did not have an observed effect on the clinical efficacy based on the exposure-response analyses in episodic and chronic migraine patients. No dose adjustments are required for fremanezumab. No data on exposure-efficacy relationship in subjects with body weight >132 kg is available.
Renal or hepatic impairment
Since monoclonal antibodies are not known to be eliminated via renal pathways or metabolised in the liver, renal and hepatic impairment are not expected to impact the pharmacokinetics of fremanezumab. Patients with severe renal impairment (eGFR <30 mL/min/1.73 m²) have not been studied. Population pharmacokinetic analysis of integrated data from the AJOVY clinical studies did not reveal a difference in the pharmacokinetics of fremanezumab in patients with mild to moderate renal impairment or hepatic impairment relative to those with normal renal or hepatic function (see section 4.2).
Preclinical safety data
Non-clinical data reveal no special hazard for humans based on conventional studies of safety pharmacology, repeated dose toxicity, toxicity to reproduction and development.
As fremanezumab is a monoclonal antibody, no genotoxicity or carcinogenicity studies have been conducted.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.