Source: Υπουργείο Υγείας (CY) Revision Year: 2019 Publisher: Medochemie Ltd, 1-10 Constantinoupoleos street, 3011 Limassol, Cyprus
Use with caution in acute myocardial infarction complicated by bradycardia, marked hypotension, or left ventricular dysfunction.
Verapamil hydrochloride affects the AV and SA nodes and prolongs AV conduction time. Use with caution as development of second-or third-degree AV block (contraindication) or unifascicular, bifascicular or trifascicular bundle branch block requires discontinuation reduction in subsequent doses or discontinuation of verapamil hydrochloride and institution of appropriate therapy, if needed.
Verapamil hydrochloride affects the AV and SA nodes and rarely may produce second-or third-degree AV block, bradycardia, and, in extreme cases, asystole. This is more likely to occur in patients with a sick sinus syndrome (SA nodal disease), which is more common in older patients.
Asystole in patients other than those with sick sinus syndrome is usually of short duration (few seconds or less), with spontaneous return to AV nodal or normal sinus rhythm. If this does not occur promptly, appropriate treatment should be initiated immediately (see section 4.8).
Patients with heart failure or those who are susceptible to heart failure should be fully digitalised before verapamil therapy as it may aggravate or precipitate cardiac failure.
Great care should be taken in: first degree AV block, bradycardia <50 beats/min, hypotension <90 mmHg systolic and ventricular tachycardias (QRS complex >0.12 sec).
If acute cardiovascular side effects arise, treat as for overdose (see section 4.9).
Although impaired renal function has been shown in robust comparator studies to have no effect on verapamil pharmacokinetics in patients with end stage renal failure, several case reports suggest that verapamil should be used cautiously and with close monitoring in patients with impaired renal function.
There has been a single post marketing report of paralysis (tetraparesis) associated with the combined use of verapamil and colchicine. This may have been caused by colchicine crossing the blood-brain barrier due to CYP3A4 and P-gp inhibition by verapamil. Combined use of verapamil and colchicine is not recommended (see section 4.5).
If verapamil is administered concomitantly with digoxin, reduce digoxin dosage (see section 4.5).
Heart failure patients with ejection fraction higher than 35% should be compensated before starting verapamil treatment and should be adequately treated throughout.
Intravenous verapamil hydrochloride often produces a decrease in blood pressure below baseline levels that is usually transient and asymptomatic but may result in dizziness. HMG-CoA Reductase Inhibitors (“Statins”) – See section 4.5.
Verapamil hydrochloride should be used with caution in the presence of diseases in which neuromuscular transmission is affected (myasthenia gravis, Lambert-Eaton syndrome, advanced Duchenne muscular dystrophy). Respiratory standstill has been reported for one patient with progressive muscular dystrophy following administration of verapamil.
Although impaired renal function has been shown in robust comparator studies to have no effect on verapamil pharmacokinetics in patients with end stage renal failure, several case reports suggest that verapamil should be used cautiously and with close monitoring in patients with impaired renal function. Verapamil cannot be removed by hemodialysis.
Use with caution in patients with severely impaired liver function (see section 4.2).
Akilen 40 mg film-coated tablets contain lactose. Patients with rare hereditary problems of galactose intolerance, the Lapp lactase deficiency or glucose-galactose malabsorption should not take this medicine.
In rare instances, including when patients with severe cardiomyopathy, congestive heart failure or recent myocardial infarction were given intravenous beta-adrenergic blocking agents or disopyramide concomitantly with intravenous verapamil hydrochloride, serious adverse effects have occurred. Concomitant use of verapamil hydrochloride injection with agents that decrease adrenergic function may result in an exaggerated hypotensive response.
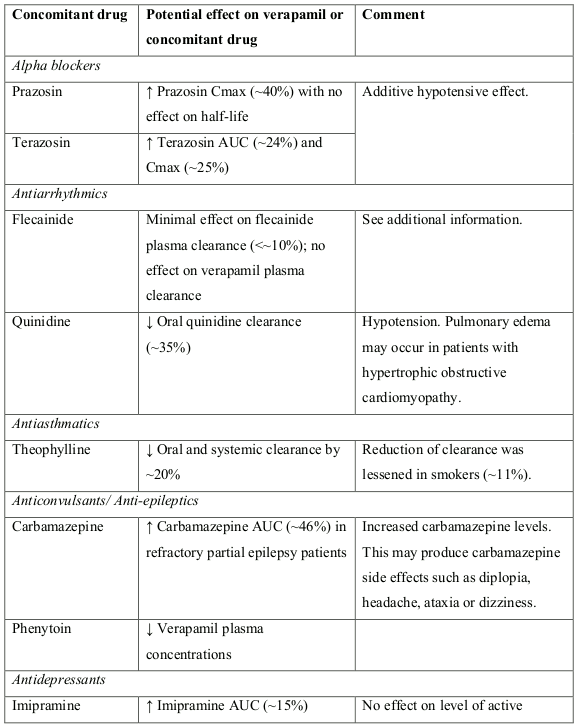
In vitro metabolic studies indicate that verapamil hydrochloride is metabolized by cytochrome P450 CYP3A4, CYP1A2, CYP2C8, CYP2C9 and CYP2C18. Verapamil has been shown to be an inhibitor of CYP3A4 enzymes and Pglycoprotein (P-gp). Clinically significant interactions have been reported with inhibitors of CYP3A4 causing elevation of plasma levels of verapamil hydrochloride while inducers of CYP3A4 have caused a lowering of plasma levels of verapamil hydrochloride, therefore, patients should be monitored for drug interactions.
When oral verapamil was co-administered with dabigatran etexilate (150 mg), a P-gp substrate, the Cmax and AUC of dabigatran were increased but magnitude of this change differs depending on time between administration and the formulation of verapamil. When verapamil 120 mg immediate-release was co-administered one hour before a single dose of dabigatran etexilate, the dabigatran Cmax was increased by about 180% and AUC by about 150%. No meaningful interaction was observed when verapamil was administered 2 hours after dabigatran etexilate (increase of Cmax by about 10% and AUC by about 20%).
Close clinical surveillance is recommended when verapamil is combined with dabigatran etexilate and particularly in the occurrence of bleeding, notably in patients having a mild to moderate renal impairment.
Concomitant use with ivabradine is contraindicated due to the additional heart rate lowering effect of verapamil to ivabradine (see section 4.3).
Potentiation of the hypotensive effect.
Due to the metabolic inhibitory potential of some of the HIV antiviral agents, such as ritonavir, plasma concentrations of verapamil may increase. Caution should be used or dose of verapamil may be decreased.
Increased sensitivity to the effects of lithium (neurotoxicity) has been reported during concomitant verapamil hydrochloride-lithium therapy with either no change or an increase in serum lithium levels. The addition of verapamil hydrochloride, however, has also resulted in the lowering of the serum lithium levels in patients receiving chronic stable oral lithium. Patients receiving both drugs should be monitored carefully.
Clinical data and animal studies suggest that verapamil hydrochloride may potentiate the activity of neuromuscular blocking agents (curare-like and depolarizing). It may be necessary to decrease the dose of verapamil hydrochloride and/or the dose of the neuromuscular blocking agent when the drugs are used concomitantly.
Increased tendency to bleed.
Elevation of ethanol plasma levels.
Treatment with HMG CoA reductase inhibitors (e.g., simvastatin, atorvastatin or lovastatin) in a patient taking verapamil should be started at the lowest possible dose and titrated upwards. If verapamil treatment is to be added to patients already taking an HMG CoA reductase inhibitor (e.g., simvastatin, atorvastatin or lovastatin), consider a reduction in the statin dose and retitrate against serum cholesterol concentrations.
Fluvastatin, pravastatin and rosuvastatin are not metabolized by CYP3A4 and are less likely to interact with verapamil.
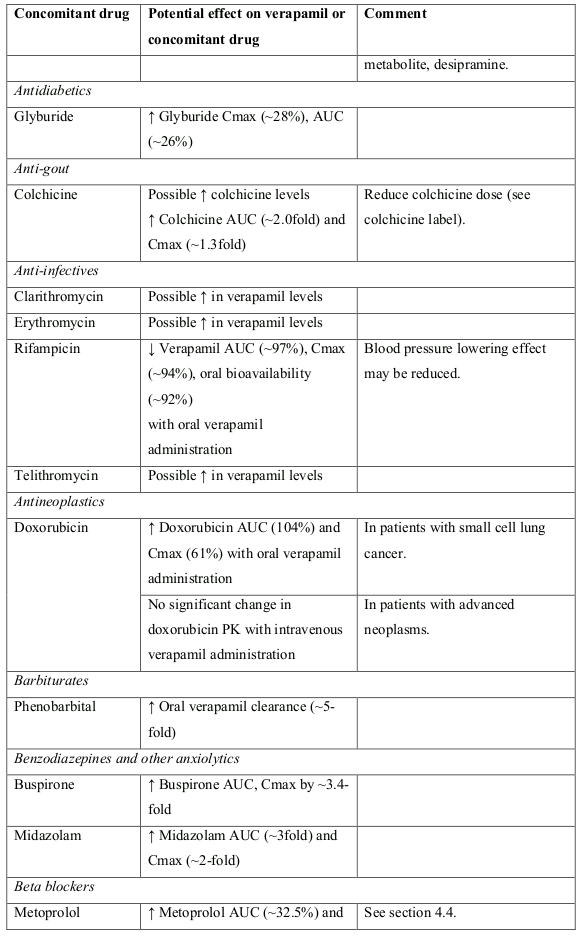
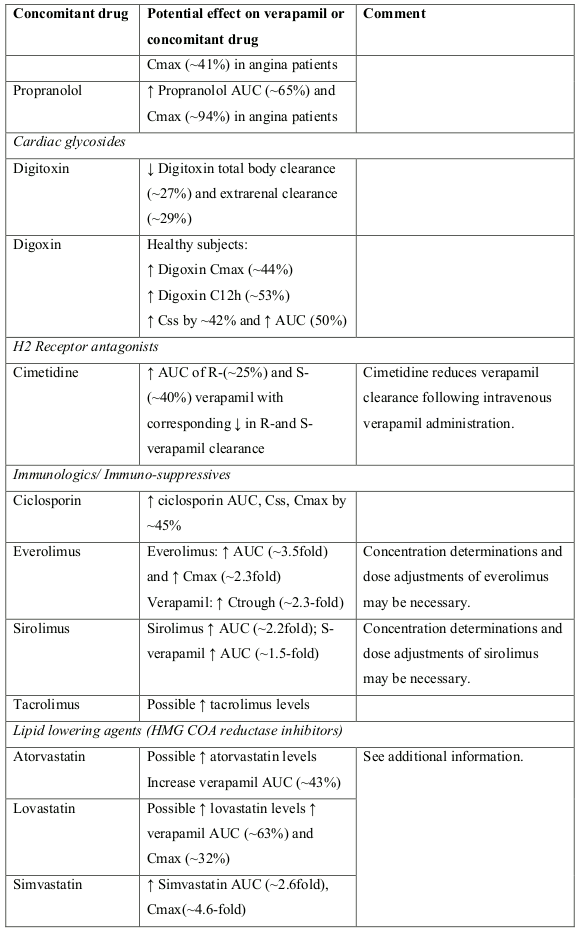
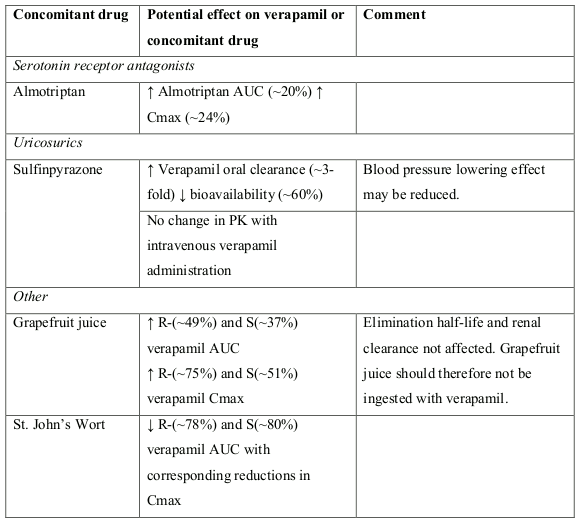
The following table provides a list of potential drug interactions with verapamil:
There are no adequate and well-controlled study data in pregnant women. Animal studies do not indicate direct or indirect harmful effects with respect to reproductive toxicity. Because animal reproduction studies are not always predictive of human response, during pregnancy (especially in the first trimester), verapamil should only be used if considered essential by the physician.
Verapamil crosses the placental barrier and can be detected in umbilical vein blood at delivery.
Verapamil hydrochloride/metabolites are excreted in human milk. Limited human data from oral administration has shown that the infant relative dose of verapamil is low (0.1-1% of the mother’s oral dose) and that verapamil use may be compatible with breastfeeding.
A risk to the newborns/infants cannot be excluded. Due to the potential for serious adverse reactions in nursing infants, verapamil should only be used during lactation if it is essential for the welfare of the mother.
Due to its antihypertensive effect, depending on the individual response, verapamil hydrochloride may affect the ability to react to the point of impairing the ability to drive a vehicle, operate machinery or work under hazardous conditions. This applies all the more at the start of treatment, when the dose is raised, when switching from another drug and in conjunction with alcohol. Verapamil may increase the blood levels of alcohol and slow its elimination. Therefore, the effects of alcohol may be exaggerated.
The following adverse events reactions have been reported with verapamil from clinical studies, post marketing surveillance or Phase IV clinical trials and are listed below by system organ class.
Frequencies are defined as: Very common (≥1/10), Common (≥1/100 to <1/10), Uncommon (≥1/1,000 to <1/100), Rare (≥1/10,000 to <1/1,000), Very rare (<1/10,000), Not known (cannot be estimated from the available data).
The most commonly reported ADRs were:
Adverse reactions reported from clinical studies with verapamil and post-marketing surveillance activities:
| MedDRA System Organ Class | Common | Uncommon | Rare | Not known |
|---|---|---|---|---|
| Immune system disorders | Hypersensitivity | |||
| Nervous system disorders | Dizziness Headache | Paresthesia Tremor | Extrapyramidal disorder Paralysis (tetraparesis)1 Seizures | |
| Metabolism and nutrition disorders | Hyperkalaemia | |||
| Psychiatric disorders | Somnolence | Nervousness | ||
| Ear and labyrinth disorders | Tinnitus | Vertigo | ||
| Cardiac disorders | Bradycardia | Palpitations Tachycardia | Atrioventricular block (1°, 2°, 3°) Cardiac failure Cardiac arrest Brady arrhythmia Sinus arrest Sinus bradycardia Asystole | |
| Vascular disorders | Flushing Hypotension | Vasodilation Erythromelalgia | ||
| Respiratory, thoracic and mediastinal disorders | Bronchospasm Dyspnea | |||
| Gastrointestinal disorders | Constipation Nausea | Abdominal pain | Vomiting | Abdominal discomfort Gingival hyperplasia Ileus |
| Skin and subcutaneous tissue disorders | Hyperhidrosis | Angioedema Stevens-Johnson syndrome Erythema multiforme Alopecia Itching Pruritus Purpura Rash maculopapular Urticaria Rash Erythema | ||
| Musculoskeletal and connective tissue disorders | Arthralgia Muscular weakness Myalgia | |||
| Renal and urinary disorders | Renal failure | |||
| Reproductive system and breast disorders | Erectile dysfunction Galactorrhea Gynecomastia | |||
| General disorders and administration site conditions | Edema peripheral | Fatigue | ||
| Investigations | Blood prolactin increased Transaminases increased Blood alkaline phosphatase increased Hepatic enzymes increased |
1 There has been a single post marketing report of paralysis (tetraparesis) associated with the combined use of verapamil and colchicine. This may have been caused by colchicine crossing the blood-brain barrier due to CYP3A4 and P-gp inhibition by verapamil. See Interactions with other medicinal products and other forms of interaction section.
Reporting suspected adverse reactions after authorization of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via the national reporting system: The Medicines Authority, Post-Licensing Directorate, 203 Level 3, Rue D’Argens, GŻR-1368 Gżira, website: www.medicinesauthority.gov.mt, e-mail: postlicensing.medicinesauthority@gov.mt.
None known.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.