Source: European Medicines Agency (EU) Revision Year: 2019 Publisher: Meda AB, Pipers väg 2A, 170 73, Solna, Sweden
Hypersensitivity to the active substance or to any of the excipients listed in section 6.1.
Avoid contact with the eyes, lips and nostrils.
Imiquimod has the potential to exacerbate inflammatory conditions of the skin.
Imiquimod cream should be used with caution in patients with autoimmune conditions (refer to section 4.5). Consideration should be given to balancing the benefit of imiquimod treatment for these patients with the risk associated with a possible worsening of their autoimmune condition.
Imiquimod cream should be used with caution in organ transplant patients (refer to section 4.5). Consideration should be given to balancing the benefit of imiquimod treatment for these patients with the risk associated with the possibility of organ rejection or graft-versus-host disease.
Imiquimod cream therapy is not recommended until the skin has healed after any previous drug or surgical treatment. Application to broken skin could result in increased systemic absorption of imiquimod leading to a greater risk of adverse events (refer to section 4.8 and 4.9)
The use of an occlusive dressing is not recommended with imiquimod cream therapy.
The excipients methyl hydroxybenzoate (E 218) and propyl hydroxybenzoate (E 216) may cause allergic reactions (possibly delayed). Cetyl alcohol and stearyl alcohol may cause local skin reactions (e.g. contact dermatitis). Benzyl alcohol may cause allergic reactions and mild local irritation.
Rarely, intense local inflammatory reactions including skin weeping or erosion can occur after only a few applications of imiquimod cream. Local inflammatory reactions may be accompanied, or even preceded, by flu-like systemic signs and symptoms including malaise, pyrexia, nausea, myalgias and rigors. An interruption of dosing should be considered.
Imiquimod should be used with caution in patients with reduced haematologic reserve (refer to section 4.8d).
There is limited experience in the use of imiquimod cream in the treatment of men with foreskin- associated warts. The safety database in uncircumcised men treated with imiquimod cream three times weekly and carrying out a daily foreskin hygiene routine is less than 100 patients. In other studies, in which a daily foreskin hygiene routine was not followed, there were two cases of severe phimosis and one case of stricture leading to circumcision. Treatment in this patient population is therefore recommended only in men who are able or willing to follow the daily foreskin hygiene routine. Early signs of stricture may include local skin reactions (e.g. erosion, ulceration, oedema, induration), or increasing difficulty in retracting the foreskin. If these symptoms occur, the treatment should be stopped immediately. Based on current knowledge, treating urethral, intra-vaginal, cervical, rectal or intra-anal warts is not recommended. Imiquimod cream therapy should not be initiated in tissues where open sores or wounds exist until after the area has healed.
Local skin reactions such as erythema, erosion, excoriation, flaking and oedema are common. Other local reactions such as induration, ulceration, scabbing, and vesicles have also been reported. Should an intolerable skin reaction occur, the cream should be removed by washing the area with mild soap and water. Treatment with imiquimod cream can be resumed after the skin reaction has moderated. The risk of severe local skin reactions may be increased when imiquimod is used at higher than recommended doses (see section 4.2). However, in rare cases severe local reactions that have required treatment and/or caused temporary incapacitation have been observed in patients who have used imiquimod according to the instructions. Where such reactions have occurred at the urethral meatus, some women have experienced difficulty in urinating, sometimes requiring emergency catheterisation and treatment of the affected area.
No clinical experience exists with imiquimod cream immediately following treatment with other cutaneously applied drugs for treatment of external genital or perianal warts. Imiquimod cream should be washed from the skin before sexual activity. Imiquimod cream may weaken condoms and diaphragms, therefore concurrent use with imiquimod cream is not recommended. Alternative forms of contraception should be considered.
In immunocompromised patients, repeat treatment with imiquimod cream is not recommended.
While limited data have shown an increased rate of wart reduction in HIV positive patients, imiquimod cream has not been shown to be as effective in terms of wart clearance in this patient group.
Imiquimod has not been evaluated for the treatment of basal cell carcinoma within 1 cm of the eyelids, nose, lips or hairline.
During therapy and until healed, affected skin is likely to appear noticeably different from normal skin. Local skin reactions are common but these reactions generally decrease in intensity during therapy or resolve after cessation of imiquimod cream therapy. There is an association between the complete clearance rate and the intensity of local skin reactions (e.g. erythema). These local skin reactions may be related to the stimulation of local immune response. If required by the patient’s discomfort or the severity of the local skin reaction, a rest period of several days may be taken. Treatment with imiquimod cream can be resumed after the skin reaction has moderated.
The clinical outcome of therapy can be determined after regeneration of the treated skin, approximately 12 weeks after the end of treatment.
No clinical experience exists with the use of imiquimod cream in immunocompromised patients.
No clinical experience exists in patients with recurrent and previously treated BCCs, therefore use for previously treated tumours is not recommended.
Data from an open label clinical trial suggest that large tumours (>7.25 cm²) are less likely to respond to imiquimod therapy.
The skin surface area treated should be protected from solar exposure.
Lesions clinically atypical for AK or suspicious for malignancy should be biopsied to determine appropriate treatment.
Imiquimod has not been evaluated for the treatment of actinic keratoses on the eyelids, the inside of the nostrils or ears, or the lip area inside the vermilion border.
There are very limited data available on the use of imiquimod for the treatment of actinic keratoses in anatomical locations other than the face and scalp. The available data on actinic keratosis on the forearms and hands do not support efficacy in this indication and therefore such use is not recommended.
Imiquimod is not recommended for the treatment of AK lesions with marked hyperkeratosis or hypertrophy as seen in cutaneous horns.
During therapy and until healed, affected skin is likely to appear noticeably different from normal skin. Local skin reactions are common but these reactions generally decrease in intensity during therapy or resolve after cessation of imiquimod cream therapy. There is an association between the complete clearance rate and the intensity of local skin reactions (e.g. erythema). These local skin reactions may be related to the stimulation of local immune response. If required by the patient’s discomfort or the intensity of the local skin reaction, a rest period of several days may be taken. Treatment with imiquimod cream can be resumed after the skin reaction has moderated.
Each treatment period should not be extended beyond 4 weeks due to missed doses or rest periods.
The clinical outcome of therapy can be determined after regeneration of the treated skin, approximately 4-8 weeks after the end of treatment.
No clinical experience exists with the use of imiquimod cream in immunocompromised patients.
Information on re-treating actinic keratosis lesions that have cleared after one or two courses of treatment and subsequently recur is given in section 4.2 and 5.1.
Data from an open-label clinical trial suggest that subjects with more than 8 AK lesions showed a decreased rate of complete clearance compared to patients with less than 8 lesions.
The skin surface area treated should be protected from solar exposure.
No interaction studies have been performed. This includes studies with immunosuppressive drugs. Interactions with systemic drugs would be limited by the minimal percutaneous absorption of imiquimod cream.
Due to its immunostimulating properties, imiquimod cream should be used with caution in patients who are receiving immunosuppressive medication (see section 4.4).
For imiquimod no clinical data on exposed pregnancies are available. Animal studies do not indicate direct or indirect harmful effects with respect to pregnancy, embryonal/foetal development, parturition or postnatal development (see section 5.3). Caution should be exercised when prescribing to pregnant women.
As no quantifiable levels (>5 ng/ml) of imiquimod are detected in the serum after single and multiple topical doses, no specific advice can be given on whether to use or not in lactating mothers.
Aldara cream has no or negligible influence on the ability to drive and use machines.
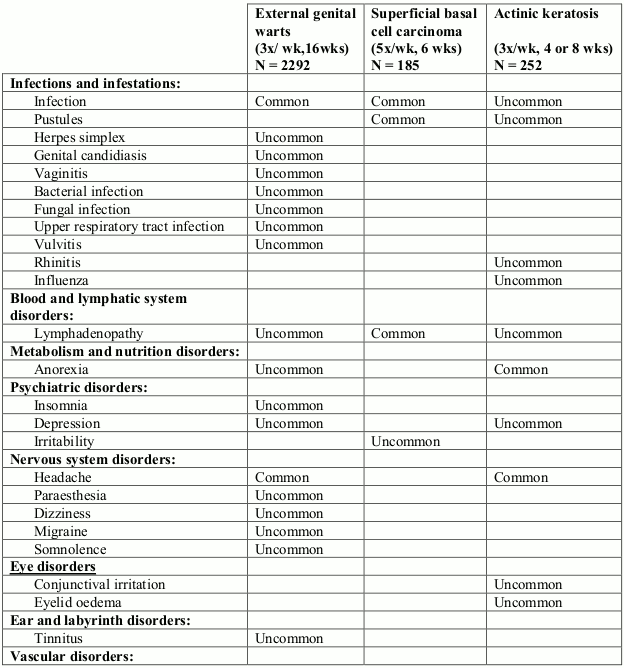
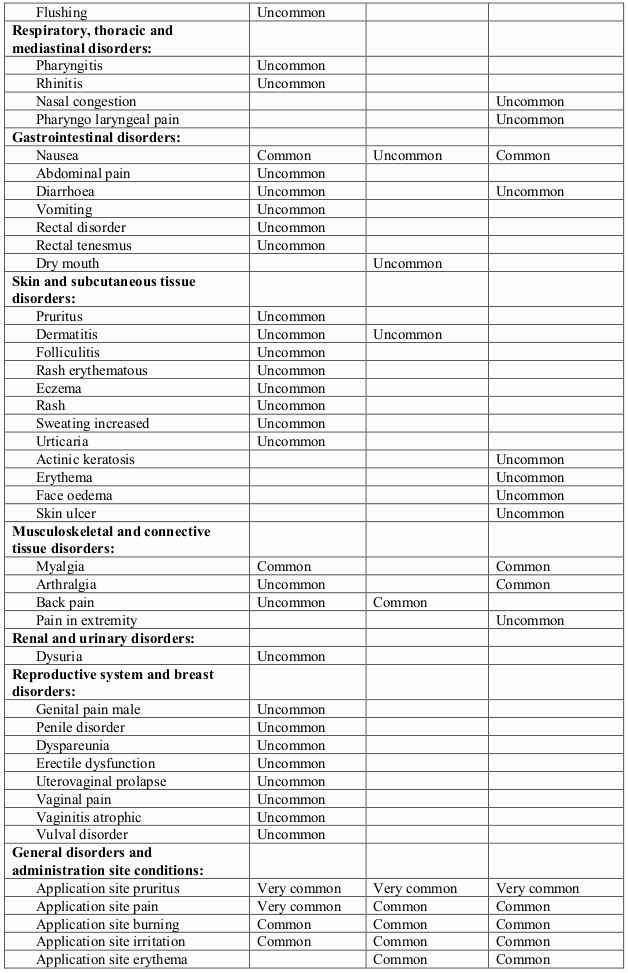
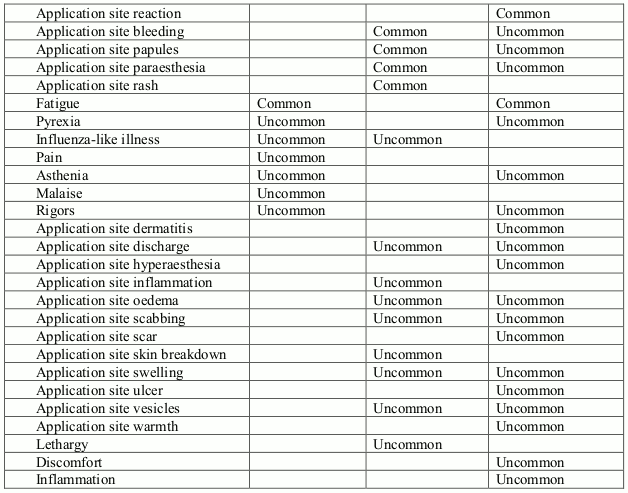
In the pivotal trials with 3 times a week dosing, the most frequently reported adverse drug reactions judged to be probably or possibly related to imiquimod cream treatment were application site reactions at the wart treatment site (33.7% of imiquimod treated patients). Some systemic adverse reactions, including headache (3.7%), influenza-like symptoms (1.1%), and myalgia (1.5%) were also reported.
Patient reported adverse reactions from 2292 patients treated with imiquimod cream in placebo controlled and open clinical studies are presented below. These adverse events are considered at least possibly causally related to treatment with imiquimod.
In trials with 5 times per week dosing 58% of patients experienced at least one adverse event. The most frequently reported adverse events from the trials judged probably or possibly related to imiquimod cream are application site disorders, with a frequency of 28.1%. Some systemic adverse reactions, including back pain (1.1%) and influenza-like symptoms (0.5%) were reported by imiquimod cream patients.
Patient reported adverse reactions from 185 patients treated with imiquimod cream in placebo controlled phase III clinical studies for superficial basal cell carcinoma are presented below. These adverse events are considered at least possibly causally related to treatment with imiquimod.
In the pivotal trials with 3 times per week dosing for up to 2 courses each of 4 weeks, 56% of imiquimod patients reported at least one adverse event. The most frequently reported adverse event from these trials judged probably or possibly related to imiquimod cream was application site reactions (22% of imiquimod treated patients). Some systemic adverse reactions, including myalgia (2%) were reported by imiquimod treated patients.
Patient reported adverse reactions from 252 patients treated with imiquimod cream in vehicle controlled phase III clinical studies for actinic keratosis are presented below. These adverse events are considered at least possibly causally related to treatment with imiquimod.
Frequencies are defined as Very common (>1/10), Common (>1/100 to <1/10) and Uncommon (>1/1,000 to <1/100). Lower frequencies from clinical trials are not reported here.
Investigators of placebo controlled trials were required to evaluate protocol mandated clinical signs (skin reactions). These protocol mandated clinical sign assessments indicate that local skin reactions including erythema (61%), erosion (30%), excoriation/flaking/scaling (23%) and oedema (14%) were common in these placebo controlled clinical trials with imiquimod cream applied three times weekly (see section 4.4). Local skin reactions, such as erythema, are probably an extension of the pharmacologic effects of imiquimod cream.
Remote site skin reactions, mainly erythema (44%), were also reported in the placebo controlled trials. These reactions were at non-wart sites which may have been in contact with imiquimod cream. Most skin reactions were mild to moderate in severity and resolved within 2 weeks of treatment discontinuation. However, in some cases these reactions have been severe, requiring treatment and/or causing incapacitation. In very rare cases, severe reactions at the urethral meatus have resulted in dysuria in women (see section 4.4).
Investigators of the placebo controlled clinical trials were required to evaluate protocol mandated clinical signs (skin reactions). These protocol mandated clinical sign assessments indicate that severe erythema (31%) severe erosions (13%) and severe scabbing and crusting (19%) were very common in these trials with imiquimod cream applied 5 times weekly. Local skin reactions, such as erythema, are probably an extension of the pharmacologic effect of imiquimod cream.
Skin infections during treatment with imiquimod have been observed. While serious sequelae have not resulted, the possibility of infection in broken skin should always be considered.
In clinical trials of imiquimod cream 3 times weekly for 4 or 8 weeks the most frequently occurring application site reactions were itching at the target site (14%) and burning at the target site (5%). Severe erythema (24%) and severe scabbing and crusting (20%) were very common. Local skin reactions, such as erythema, are probably an extension of the pharmacologic effect of imiquimod cream. See 4.2 and 4.4 for information on rest periods.
Skin infections during treatment with imiquimod have been observed. While serious sequelae have not resulted, the possibility of infection in broken skin should always be considered.
Reports have been received of localised hypopigmentation and hyperpigmentation following imiquimod cream use. Follow-up information suggests that these skin colour changes may be permanent in some patients. In a follow-up of 162 patients five years after treatment for sBCC a mild hypopigmentation was observed in 37% of the patients and a moderate hypopigmentation was observed in 6% of the patients. 56% of the patients have been free of hypopigmentation; hyperpigmentation has not been reported.
Clinical studies investigating the use of imiquimod for the treatment of actinic keratosis have detected a 0.4% (5/1214) frequency of alopecia at the treatment site or surrounding area. Postmarketing reports of suspected alopecia occurring during the treatment of sBCC and EGW have been received.
Reductions in haemoglobin, white blood cell count, absolute neutrophils and platelets have been observed in clinical trials. These reductions are not considered to be clinically significant in patients with normal haematologic reserve. Patients with reduced haematologic reserve have not been studied in clinical trials. Reductions in haematological parameters requiring clinical intervention have been reported from postmarketing experience. There have been postmarketing reports of elevated liver enzymes.
Rare reports have been received of exacerbation of autoimmune conditions.
Rare cases of remote site dermatologic drug reactions, including erythema multiforme, have been reported from clinical trials. Serious skin reactions reported from postmarketing experience include erythema multiforme, Stevens Johnson syndrome and cutaneous lupus erythematosus.
Imiquimod was investigated in controlled clinical studies with paediatric patients (see sections 4.2 and 5.1). There was no evidence for systemic reactions. Application site reactions occurred more frequently after imiquimod than after vehicle, however, incidence and intensity of these reactions were not different from that seen in the licensed indications in adults. There was no evidence for serious adverse reaction caused by imiquimod in paediatric patients.
Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via the national reporting system listed in Appendix V.
Not applicable.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.