AMMONUL Solution for injection Ref.[10164] Active ingredients: Banzoic acid
Source: FDA, National Drug Code (US) Revision Year: 2019
12.1. Mechanism of Action
Urea cycle disorders can result from decreased activity of any of the following enzymes: N-acetylglutamate synthetase (NAGS), carbamyl phosphate synthetase (CPS), argininosuccinate synthetase (ASS), ornithine transcarbamylase (OTC), argininosuccinate lyase (ASL), or arginase (ARG).
Sodium phenylacetate and sodium benzoate are metabolically active compounds that can serve as alternatives to urea for the excretion of waste nitrogen. Figure 2 is a schematic illustrating how the components of AMMONUL, phenylacetate and benzoate, provide an alternative pathway for nitrogen disposal in patients without a fully functioning urea cycle. Phenylacetate conjugates with glutamine in the liver and kidneys to form phenylacetylglutamine, via acetylation. Phenylacetylglutamine is excreted by the kidneys via glomerular filtration and tubular secretion. The nitrogen content of phenylacetylglutamine per mole is identical to that of urea (both contain two moles of nitrogen). Two moles of nitrogen are removed per mole of phenylacetate when it is conjugated with glutamine. Similarly, preceded by acylation, benzoate conjugates with glycine to form hippuric acid, which is rapidly excreted by the kidneys by glomerular filtration and tubular secretion. One mole of hippuric acid contains one mole of waste nitrogen. Thus, one mole of nitrogen is removed per mole of benzoate when it is conjugated with glycine.
Figure 2:
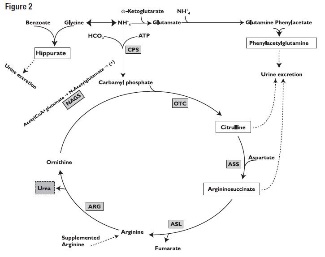
CPS = carbamyl phosphate synthetase;
OTC = ornithine transcarbamylase;
ASS = argininosuccinate synthetase;
ASL = argininosuccinate lyase;
ARG = arginase;
NAGS = N-acetylglutamate synthetase
12.2. Pharmacodynamics
In patients with hyperammonemia due to deficiencies in enzymes of the urea cycle, AMMONUL has been shown to decrease elevated plasma ammonia levels. These effects are considered to be the result of reduction in nitrogen overload through glutamine and glycine scavenging by AMMONUL in combination with appropriate dietary and other supportive measures.
12.3. Pharmacokinetics
The pharmacokinetics of intravenously administered AMMONUL was characterized in healthy adult volunteers. Both benzoate and phenylacetate exhibited nonlinear kinetics. Following 90 minute intravenous infusion mean AUClast for benzoate was 20.3, 114.9, 564.6, 562.8, and 1599.1 mcg/mL following doses of 1, 2, 3.75, 4, and 5.5 g/m², respectively. The total clearance decreased from 5.19 to 3.62 L/h/m² at the 3.75 and 5.5 g/m² doses, respectively.
Similarly, phenylacetate exhibited nonlinear kinetics following the priming dose regimens. AUClast was 175.6, 713.8, 2040.6, 2181.6, and 3829.2 mcg∙h/mL following doses of 1, 2, 3.75, 4, and 5.5 g/m², respectively. The total clearance decreased from 1.82 to 0.89 mcg∙h/mL with increasing dose (3.75 and 4 g/m², respectively).
During the sequence of 90 minute priming infusion followed by a 24 hour maintenance infusion, phenylacetate was detected in the plasma at the end of infusion (Tmax of 2 hr at 3.75 g/m²) whereas, benzoate concentrations declined rapidly (Tmax of 1.5 hr at 3.75 g/m²) and were undetectable at 14 and 26 hours following the 3.75 and 4 g/m² dose, respectively.
A difference in the metabolic rates for phenylacetate and benzoate was noted. The formation of hippurate from benzoate occurred more rapidly than that of phenylacetylglutamine from phenylacetate, and the rate of elimination for hippurate appeared to be more rapid than that for phenylacetylglutamine.
Pharmacokinetic observations have also been reported from twelve episodes of hyperammonemic encephalopathy in seven children diagnosed (age 3 to 26 months) with urea cycle disorders who had been administered AMMONUL intravenously. These data showed peak plasma levels of phenylacetate and benzoate at approximately the same times as were observed in healthy adults. As in healthy adults, the plasma levels of phenylacetate were higher than benzoate and were present for a longer time.
The pharmacokinetics of intravenous phenylacetate have been reported following administration to adult patients with advanced solid tumors. The decline in serum phenylacetate concentrations following a loading infusion of 150 mg/kg was consistent with saturable enzyme kinetics. Ninety-nine percent of administered phenylacetate was excreted as phenylacetylglutamine.
13.1. Carcinogensis, Mutagenesis, Impairment of Fertility
Long-term studies in animals have not been performed to evaluate the carcinogenic potential of AMMONUL. Studies to evaluate the possible impairment of fertility or mutagenic potential of AMMONUL have not been performed. Results indicate that sodium benzoate is not mutagenic or carcinogenic, and does not impair fertility.
13.2. Animal Toxicology and/or Pharmacology
In animal studies, subcutaneous administration to rat pups of 190–474 mg/kg of phenylacetate caused decreased proliferation and increased loss of neurons, and reduced central nervous system (CNS) myelin. Cerebral synapse maturation was retarded, and the number of functioning nerve terminals in the cerebrum was reduced, which resulted in impaired brain growth. Pregnant rats were given phenylacetate at 3.5 µmol/g/day subcutaneously from gestation day 7 through normal delivery. Prenatal exposure of rat pups to phenylacetate produced lesions in layer 5 cortical pyramidal cells; dendritic spines were longer and thinner than normal and reduced in number.
14. Clinical Studies
The efficacy of AMMONUL in improving patient survival of acute hyperammonemic episodes was demonstrated in an analysis of 316 patients (1,045 episodes of hospitalization) treated between 1981 and 2003.
The demographic characteristics and diagnoses of the patient population are shown in Table 3.
Table 3. Baseline Characteristics and Diagnoses of Study Population:
| Patients N=316 | ||
|---|---|---|
| Gender | Male | 158 (51%) |
| Female | 150 (49%) | |
| Age (years) | N | 310 |
| Mean (SD) | 6.2 (8.54) | |
| Min–Max | 0.0–53.0 | |
| Age groups | 0–30 days | 104 (34%) |
| 31 days–2 years | 55 (18%) | |
| >2–12 years | 90 (29%) | |
| >12–16 years | 30 (10%) | |
| >16 years | 31 (10%) | |
| Enzyme deficiency | OTC | 146 (46%) |
| ASS | 71 (22%) | |
| CPS | 38 (12%) | |
| ASL | 7 (2%) | |
| ARG | 2 (<1%) | |
| THN | 2 (<1%) | |
| Other | 56 (18%) |
OTC = ornithine transcarbamylase deficiency
ASS = argininosuccinate synthetase deficiency
CPS = carbamyl phosphate synthetase deficiency
ASL = argininosuccinate lyase deficiency
ARG = arginase deficiency
THN = transient hyperammonemia of the newborn
On admission to the hospital, patients with hyperammonemia and a suspected or confirmed urea cycle disorder (UCD) diagnosis were treated with a bolus dose of 0.25 g/kg (or 5.5 g/m²) sodium phenylacetate + 0.25 g/kg (or 5.5 g/m²) sodium benzoate over a period of 90 minutes to 6 hours, depending on the specific UCD. Infusions also contained arginine; the dose of arginine depended on the specific UCD. After completion of the bolus dose, maintenance infusions of the same dose over 24 hours were continued until the patient was no longer hyperammonemic or oral therapy could be tolerated. The mean (SD) duration of treatment was 4.6 (6.45) days per episode, and ranged from 1 to 72 days.
Survival was substantially improved after AMMONUL treatment compared with historical values (estimated 14% 1-year survival rate with dietary therapy alone) and with dialysis (estimated 43% survival of acute hyperammonemia).
Eighty percent of patients (252 of 316) survived their last episode. Of the 64 patients who died, 53 (83%) died during their first hyperammonemic episode. Of the 104 neonates (<30d) treated with AMMONUL, 34 (33%) died during the first hyperammonemic episode.
Ammonia levels decreased from very high levels (>4 times the upper limit of normal [ULN]) to lower levels in 91% of episodes after treatment. In patients responding to therapy, mean ammonia concentrations decreased from 200.9 µmol/L at hour zero to 101.6 µmol/L within four hours of initiation of AMMONUL therapy and were maintained. Hemodialysis is recommended for those patients whose plasma ammonia levels fail to fall below 150 µmol/L or by more than 40% within 4 to 8 hours after receiving AMMONUL. A shift from high (≤4 times ULN) to very high (>4 times ULN) levels was observed in only 4% of the episodes.
Overall, investigators rated neurological status as improved, much improved, or the same in 93% of episodes, and overall status in response to treatment as improved, much improved, or the same in 97% of episodes. Recovery from coma was observed in 97% of episodes where coma was present at admission (111 of 114 episodes).
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.