Source: FDA, National Drug Code (US) Revision Year: 2020
Endogenous androgens, including testosterone and dihydrotestosterone (DHT), are responsible for the normal growth and development of the male sex organs and for maintenance of secondary sex characteristics. These effects include the growth and maturation of prostate, seminal vesicles, penis and scrotum; the development of male hair distribution, such as facial, pubic, chest and axillary hair; laryngeal enlargement, vocal chord thickening, alterations in body musculature and fat distribution. Testosterone and DHT are necessary for the normal development of secondary sex characteristics.
Male hypogonadism, a clinical syndrome resulting from insufficient secretion of testosterone, has two main etiologies. Primary hypogonadism is caused by defects of the gonads, such as Klinefelter’s syndrome or Leydig cell aplasia, whereas secondary hypogonadism is the failure of the hypothalamus (or pituitary) to produce sufficient gonadotropins (FSH, LH).
No specific pharmacodynamic studies were conducted using AndroGel 1%.
AndroGel 1% delivers physiologic amounts of testosterone, producing circulating testosterone concentrations that approximate normal concentrations (298-1043 ng/dL) seen in healthy men. AndroGel 1% provides continuous transdermal delivery of testosterone for 24 hours following a single application to intact, clean, dry skin of the shoulders, upper arms and/or abdomen.
AndroGel 1% is a hydroalcoholic formulation that dries quickly when applied to the skin surface. The skin serves as a reservoir for the sustained release of testosterone into the systemic circulation. Approximately 10% of the testosterone dose applied on the skin surface from AndroGel is absorbed into systemic circulation. In a study with AndroGel 1% 100 mg, all patients showed an increase in serum testosterone within 30 minutes, and eight of nine patients had a serum testosterone concentration within normal range by 4 hours after the initial application. Absorption of testosterone into the blood continues for the entire 24-hour dosing interval. Serum concentrations approximate the steady-state concentration by the end of the first 24 hours and are at steady state by the second or third day of dosing.
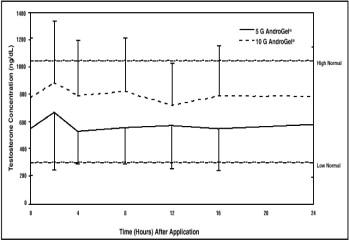
With single daily applications of AndroGel 1%, follow-up measurements 30, 90 and 180 days after starting treatment have confirmed that serum testosterone concentrations are generally maintained within the eugonadal range. Figure 1 summarizes the 24-hour pharmacokinetic profiles of testosterone for hypogonadal men (less than 300 ng/dL) maintained on AndroGel 1% 50 mg or 100 mg for 30 days. The average (± SD) daily testosterone concentration produced by AndroGel 1% 100 mg on Day 30 was 792 (± 294) ng/dL and by AndroGel 1% 50 mg 566 (± 262) ng/dL.
Figure 1. Mean (± SD) Steady-State Serum Testosterone Concentrations on Day 30 in Patients Applying AndroGel 1% Once Daily:
Circulating testosterone is primarily bound in the serum to sex hormone-binding globulin (SHBG) and albumin. Approximately 40% of testosterone in plasma is bound to SHBG, 2% remains unbound (free) and the rest is bound to albumin and other proteins.
Testosterone is metabolized to various 17-keto steroids through two different pathways. The major active metabolites of testosterone are estradiol and dihydrotestosterone (DHT).
DHT concentrations increased in parallel with testosterone concentrations during AndroGel 1% treatment. The mean steady-state DHT/T ratio during 180 days of AndroGel treatment ranged from 0.23 to 0.29 (50 mg of AndroGel 1%/day) and from 0.27 to 0.33 (100 mg of AndroGel 1%/day).
There is considerable variation in the half-life of testosterone concentration as reported in the literature, ranging from 10 to 100 minutes. About 90% of a dose of testosterone given intramuscularly is excreted in the urine as glucuronic and sulfuric acid conjugates of testosterone and its metabolites. About 6% of a dose is excreted in the feces, mostly in the unconjugated form. Inactivation of testosterone occurs primarily in the liver.
When AndroGel 1% treatment is discontinued after achieving steady state, serum testosterone concentrations remain in the normal range for 24 to 48 hours but return to their pretreatment concentrations by the fifth day after the last application.
The potential for dermal testosterone transfer following AndroGel 1% use was evaluated in a clinical study between males dosed with AndroGel 1% and their untreated female partners. Two (2) to 12 hours after application of 100 mg of testosterone administered as AndroGel 1% by the male subjects, the couples (N = 38 couples) engaged in daily, 15-minute sessions of vigorous skin-to-skin contact so that the female partners gained maximum exposure to the AndroGel 1% application sites. Under these study conditions, all unprotected female partners had a serum testosterone concentration >2 times the baseline value at some time during the study. When a shirt covered the application site(s), the transfer of testosterone from the males to the female partners was completely prevented.
Testosterone has been tested by subcutaneous injection and implantation in mice and rats. In mice, the implant induced cervical-uterine tumors which metastasized in some cases. There is suggestive evidence that injection of testosterone into some strains of female mice increases their susceptibility to hepatoma. Testosterone is also known to increase the number of tumors and decrease the degree of differentiation of chemically induced carcinomas of the liver in rats.
Testosterone was negative in the in vitro Ames and in the in vivo mouse micronucleus assays.
The administration of exogenous testosterone has been reported to suppress spermatogenesis in rats, dogs, and non-human primates, which was reversible on cessation of the treatment.
AndroGel 1% was evaluated in a multi-center, randomized, parallel-group, active-controlled, 180-day trial in 227 hypogonadal men. The study was conducted in 2 phases. During the Initial Treatment Period (Days 1-90), 73 patients were randomized to AndroGel 1% 50 mg daily, 78 patients to AndroGel 1% 100 mg daily, and 76 patients to a non-scrotal testosterone transdermal system. The study was double-blind for dose of AndroGel 1% but open-label for active control. Patients who were originally randomized to AndroGel 1% and who had single-sample serum testosterone concentrations above or below the normal range on Day 60 were titrated to 75 mg daily on Day 91. During the Extended Treatment Period (Days 91-180), 51 patients continued on AndroGel 1% 50 mg daily, 52 patients continued on AndroGel 1% 100 mg daily, 41 patients continued on a non-scrotal testosterone transdermal system (5 mg daily), and 40 patients received AndroGel 1% 75 mg daily. Upon completion of the initial study, 163 enrolled and 162 patients received treatment in an open-label extension study of AndroGel 1% for an additional period of up to 3 years.
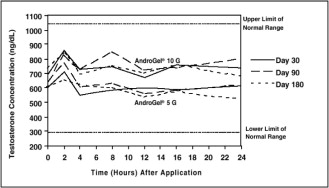
Mean peak, trough and average serum testosterone concentrations within the normal range (298-1043 ng/dL) were achieved on the first day of treatment with doses of 50 mg and 100 mg of AndroGel 1%. In patients continuing on AndroGel 1% 50 mg and 100 mg, these mean testosterone concentrations were maintained within the normal range for the 180-day duration of the original study. Figure 2 summarizes the 24-hour pharmacokinetic profiles of testosterone administered as AndroGel 1% for 30, 90 and 180 days. Testosterone concentrations were maintained as long as the patient continued to properly apply the prescribed AndroGel 1% treatment.
Figure 2. Mean Steady-State Testosterone Concentrations in Patients with Once-Daily AndroGel 1% Therapy:
Table 4 summarizes the mean testosterone concentrations on Treatment Day 180 for patients receiving 50 mg, 75 mg, or 100 mg of AndroGel 1%. The 75 mg dose produced mean concentrations intermediate to those produced by 50 mg and 100 mg of AndroGel 1%.
Table 4. Mean (± SD) Steady-State Serum Testosterone Concentrations During Therapy (Day 180):
| 50 mg | 75 mg | 100 mg | |
|---|---|---|---|
| N=44 | N=37 | N=48 | |
| Cavg | 555 ± 225 | 601 ± 309 | 713 ± 209 |
| Cmax | 830 ± 347 | 901 ± 471 | 1083 ± 434 |
| Cmin | 371 ± 165 | 406 ± 220 | 485 ± 156 |
Of 129 hypogonadal men who were appropriately titrated with AndroGel 1% and who had sufficient data for analysis, 87% achieved an average serum testosterone concentration within the normal range on Treatment Day 180.
In patients treated with AndroGel 1%, there were no observed differences in the average daily serum testosterone concentrations at steady-state based on age, cause of hypogonadism, or body mass index.
DHT concentrations increased in parallel with testosterone concentrations at AndroGel 1% doses of 50 mg/day and 100 mg/day, but the DHT/T ratio stayed within the normal range, indicating enhanced availability of the major physiologically active androgen. Serum estradiol (E2) concentrations increased significantly within 30 days of starting treatment with AndroGel 1% 50 or 100 mg/day and remained elevated throughout the treatment period but remained within the normal range for eugonadal men. Serum levels of SHBG decreased very slightly (1 to 11%) during AndroGel 1% treatment. In men with hypergonadotropic hypogonadism, serum levels of LH and FSH fell in a dose- and time-dependent manner during treatment with AndroGel 1%.
The phototoxic potential of AndroGel 1% was evaluated in a double-blind, single-dose study in 27 subjects with photosensitive skin types. The Minimal Erythema Dose (MED) of ultraviolet radiation was determined for each subject. A single 24 (+1) hour application of duplicate patches containing test articles (placebo gel, testosterone gel, or saline) was made to naive skin sites on Day 1. On Day 2, each subject received five exposure times of ultraviolet radiation, each exposure being 25% greater than the previous one. Skin evaluations were made on Days 2 to 5. Exposure of test and control article application sites to ultraviolet light did not produce increased inflammation relative to non-irradiated sites, indicating no phototoxic effect.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.