BENICAR Film-coated tablet Ref.[49687] Active ingredients: Olmesartan medoxomil
Source: FDA, National Drug Code (US) Revision Year: 2021
12.1. Mechanism of Action
Angiotensin II is formed from angiotensin I in a reaction catalyzed by angiotensin converting enzyme (ACE, kininase II). Angiotensin II is the principal pressor agent of the renin-angiotensin system, with effects that include vasoconstriction, stimulation of synthesis and release of aldosterone, cardiac stimulation and renal reabsorption of sodium. Olmesartan blocks the vasoconstrictor effects of angiotensin II by selectively blocking the binding of angiotensin II to the AT1 receptor in vascular smooth muscle. Its action is, therefore, independent of the pathways for angiotensin II synthesis.
An AT2 receptor is found also in many tissues, but this receptor is not known to be associated with cardiovascular homeostasis. Olmesartan has more than a 12,500-fold greater affinity for the AT1 receptor than for the AT2 receptor.
Blockade of the renin-angiotensin system with ACE inhibitors, which inhibit the biosynthesis of angiotensin II from angiotensin I, is a mechanism of many drugs used to treat hypertension. ACE inhibitors also inhibit the degradation of bradykinin, a reaction also catalyzed by ACE. Because olmesartan medoxomil does not inhibit ACE (kininase II), it does not affect the response to bradykinin. Whether this difference has clinical relevance is not yet known.
Blockade of the angiotensin II receptor inhibits the negative regulatory feedback of angiotensin II on renin secretion, but the resulting increased plasma renin activity and circulating angiotensin II levels do not overcome the effect of olmesartan on blood pressure.
12.2. Pharmacodynamics
Benicar doses of 2.5 mg to 40 mg inhibit the pressor effects of angiotensin I infusion. The duration of the inhibitory effect was related to dose, with doses of Benicar >40 mg giving >90% inhibition at 24 hours.
Plasma concentrations of angiotensin I and angiotensin II and plasma renin activity (PRA) increase after single and repeated administration of Benicar to healthy subjects and hypertensive patients. Repeated administration of up to 80 mg Benicar had minimal influence on aldosterone levels and no effect on serum potassium.
12.3. Pharmacokinetics
Absorption
Olmesartan medoxomil is rapidly and completely bioactivated by ester hydrolysis to olmesartan during absorption from the gastrointestinal tract.
Benicar tablets and the suspension formulation prepared from Benicar tablets are bioequivalent [see Dosage and Administration (2.2)].
The absolute bioavailability of olmesartan is approximately 26%. After oral administration, the peak plasma concentration (Cmax) of olmesartan is reached after 1 to 2 hours. Food does not affect the bioavailability of olmesartan. Benicar may be administered with or without food.
Distribution
The volume of distribution of olmesartan is approximately 17 L. Olmesartan is highly bound to plasma proteins (99%) and does not penetrate red blood cells. The protein binding is constant at plasma olmesartan concentrations well above the range achieved with recommended doses.
In rats, olmesartan crossed the blood-brain barrier poorly, if at all. Olmesartan passed across the placental barrier in rats and was distributed to the fetus. Olmesartan was distributed to milk at low levels in rats.
Metabolism and Excretion
Following the rapid and complete conversion of olmesartan medoxomil to olmesartan during absorption, there is virtually no further metabolism of olmesartan. Total plasma clearance of olmesartan is 1.3 L/h, with a renal clearance of 0.6 L/h. Approximately 35% to 50% of the absorbed dose is recovered in urine while the remainder is eliminated in feces via the bile.
Olmesartan appears to be eliminated in a biphasic manner with a terminal elimination half-life of approximately 13 hours. Olmesartan shows linear pharmacokinetics following single oral doses of up to 320 mg and multiple oral doses of up to 80 mg. Steady-state levels of olmesartan are achieved within 3 to 5 days and no accumulation in plasma occurs with once-daily dosing.
Specific Populations
Geriatric Patients
The pharmacokinetics of olmesartan were studied in the elderly (≥65 years). Overall, maximum plasma concentrations of olmesartan were similar in young adults and the elderly. Modest accumulation of olmesartan was observed in the elderly with repeated dosing; AUCss,τ was 33% higher in elderly patients, corresponding to an approximate 30% reduction in CLR [see Dosage and Administration (2.1) and Use in Specific Populations (8.5)].
Pediatric Patients
The pharmacokinetics of olmesartan were studied in pediatric hypertensive patients aged 1 to 16 years. The clearance of olmesartan in pediatric patients was similar to that in adult patients when adjusted by the body weight [see Use in Specific Populations (8.4)].
Olmesartan pharmacokinetics have not been investigated in pediatric patients less than 1 year of age [see Warnings and Precautions (5.2) and Use in Specific Populations (8.4)].
Male and Female Patients
Minor differences were observed in the pharmacokinetics of olmesartan in women compared to men. AUC and Cmax were 10-15% higher in women than in men.
Patients with Hepatic Impairment
Increases in AUC0-∞ and Cmax were observed in patients with moderate hepatic impairment compared to those in matched controls, with an increase in AUC of about 60% [see Dosage and Administration (2.1) and Use in Specific Populations (8.6)].
Patients with Renal Impairment
In patients with renal insufficiency, serum concentrations of olmesartan were elevated compared to subjects with normal renal function. After repeated dosing, the AUC was approximately tripled in patients with severe renal impairment (creatinine clearance <20 mL/min). The pharmacokinetics of olmesartan in patients undergoing hemodialysis has not been studied [see Dosage and Administration (2.1), Warnings and Precautions (5.4) and Use in Specific Populations (8.7)].
Drug Interaction Studies
Bile Acid Sequestering Agent Colesevelam
Concomitant administration of 40 mg olmesartan medoxomil and 3750 mg colesevelam hydrochloride in healthy subjects resulted in 28% reduction in Cmax and 39% reduction in AUC of olmesartan. Lesser effects, 4% and 15% reduction in Cmax and AUC respectively, were observed when olmesartan medoxomil was administered 4 hours prior to colesevelam hydrochloride [see Drug Interactions (7.5)].
Other Studies
No significant drug interactions were reported in studies in which olmesartan medoxomil was co-administered with digoxin or warfarin in healthy volunteers.
The bioavailability of olmesartan was not significantly altered by the co-administration of antacids [Al(OH)3/Mg(OH)2].
Olmesartan medoxomil is not metabolized by the cytochrome P450 system and has no effects on P450 enzymes; thus, interactions with drugs that inhibit, induce, or are metabolized by those enzymes are not expected.
13.1. Carcinogenesis, Mutagenesis, Impairment of Fertility
Olmesartan medoxomil was not carcinogenic when administered by dietary administration to rats for up to 2 years. The highest dose tested (2000 mg/kg/day) was, on a mg/m2 basis, about 480 times the maximum recommended human dose (MRHD) of 40 mg/day. Two carcinogenicity studies conducted in mice, a 6-month gavage study in the p53 knockout mouse and a 6-month dietary administration study in the Hras2 transgenic mouse, at doses of up to 1000 mg/kg/day (about 120 times the MRHD), revealed no evidence of a carcinogenic effect of olmesartan medoxomil.
Both olmesartan medoxomil and olmesartan tested negative in the in vitro Syrian hamster embryo cell transformation assay and showed no evidence of genetic toxicity in the Ames (bacterial mutagenicity) test. However, both were shown to induce chromosomal aberrations in cultured cells in vitro (Chinese hamster lung) and tested positive for thymidine kinase mutations in the in vitro mouse lymphoma assay. Olmesartan medoxomil tested negative in vivo for mutations in the MutaMouse intestine and kidney and for clastogenicity in mouse bone marrow (micronucleus test) at oral doses of up to 2000 mg/kg (olmesartan not tested).
Fertility of rats was unaffected by administration of olmesartan medoxomil at dose levels as high as 1000 mg/kg/day (240 times the MRHD) in a study in which dosing was begun 2 (female) or 9 (male) weeks prior to mating.
14. Clinical Studies
14.1 Adult Hypertension
The antihypertensive effects of Benicar have been demonstrated in seven placebo-controlled studies at doses ranging from 2.5 mg to 80 mg for 6 to 12 weeks, each showing statistically significant reductions in peak and trough blood pressure. A total of 2693 patients (2145 Benicar; 548 placebo) with essential hypertension were studied. Benicar once daily lowered diastolic and systolic blood pressure. The response was dose related, as shown in the following graph. A Benicar dose of 20 mg daily produces a trough sitting blood pressure (BP) reduction over placebo of about 10/6 mmHg and a dose of 40 mg daily produces a trough sitting BP reduction over placebo of about 12/7 mmHg. Benicar doses greater than 40 mg had little additional effect. The onset of the antihypertensive effect occurred within 1 week and was largely manifest after 2 weeks.
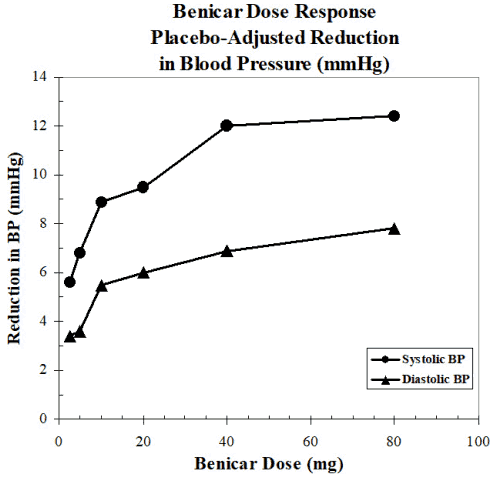
Data above are from seven placebo-controlled studies (2145 Benicar patients, 548 placebo patients). The blood pressure lowering effect was maintained throughout the 24-hour period with Benicar once daily, with trough-to-peak ratios for systolic and diastolic response between 60 and 80%.
The blood pressure lowering effect of Benicar, with and without hydrochlorothiazide, was maintained in patients treated for up to 1 year. There was no evidence of tachyphylaxis during long-term treatment with Benicar or rebound effect following abrupt withdrawal of olmesartan medoxomil after 1 year of treatment.
The antihypertensive effect of Benicar was similar in men and women and in patients older and younger than 65 years. The effect was smaller in black patients (usually a low-renin population), as has been seen with ACE inhibitors, beta-blockers and other angiotensin receptor blockers. Benicar had an additional blood pressure lowering effect when added to hydrochlorothiazide.
There are no trials of Benicar demonstrating reductions in cardiovascular risk in patients with hypertension, but at least one pharmacologically similar drug has demonstrated such benefits.
14.2 Pediatric Hypertension
The antihypertensive effects of Benicar in the pediatric population were evaluated in a randomized, double-blind study involving 302 hypertensive patients aged 6 to 16 years. The study population consisted of an all-black cohort of 112 patients and a mixed racial cohort of 190 patients, including 38 black patients. The etiology of the hypertension was predominantly essential hypertension (87% of the black cohort and 67% of the mixed cohort). Patients who weighed 20 to <35 kg were randomized to 2.5 or 20 mg of Benicar once daily and patients who weighed ≥35 kg were randomized to 5 or 40 mg of Benicar once daily. At the end of 3 weeks, patients were re-randomized to continuing Benicar or to taking placebo for up to 2 weeks. During the initial dose-response phase, Benicar significantly reduced both systolic and diastolic blood pressure in a weight-adjusted, dose-dependent manner. Overall, the two dose levels of Benicar (low and high) significantly reduced systolic blood pressure by 6.6 and 11.9 mmHg from the baseline, respectively. These reductions in systolic blood pressure included both drug and placebo effect. During the randomized withdrawal to placebo phase, mean systolic blood pressure at trough was 3.2 mmHg lower and mean diastolic blood pressure at trough was 2.8 mmHg lower in patients continuing Benicar than in patients withdrawn to placebo. These differences were statistically different. As observed in adult populations, the blood pressure reductions were smaller in black patients.
In the same study, 59 patients aged 1 to 5 years who weighed ≥5 kg received 0.3 mg/kg of Benicar once daily for three weeks in an open-label phase and then were randomized to receiving Benicar or placebo in a double-blind phase. At the end of the second week of withdrawal, the mean systolic/diastolic blood pressure at trough was 3/3 mmHg lower in the group randomized to Benicar; this difference in blood pressure was not statistically significant (95% C.I. -2 to 7/-1 to 7).
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.