BRILINTA Film-coated tablet Ref.[10761] Active ingredients: Ticagrelor
Source: FDA, National Drug Code (US) Revision Year: 2021
12.1. Mechanism of Action
Ticagrelor and its major metabolite reversibly interact with the platelet P2Y12 ADP-receptor to prevent signal transduction and platelet activation. Ticagrelor and its active metabolite are approximately equipotent.
12.2. Pharmacodynamics
The inhibition of platelet aggregation (IPA) by ticagrelor and clopidogrel was compared in a 6-week study examining both acute and chronic platelet inhibition effects in response to 20 μM ADP as the platelet aggregation agonist.
The onset of IPA was evaluated on Day 1 of the study following loading doses of 180 mg ticagrelor or 600 mg clopidogrel. As shown in Figure 5, IPA was higher in the ticagrelor group at all time points. The maximum IPA effect of ticagrelor was reached at around 2 hours, and was maintained for at least 8 hours.
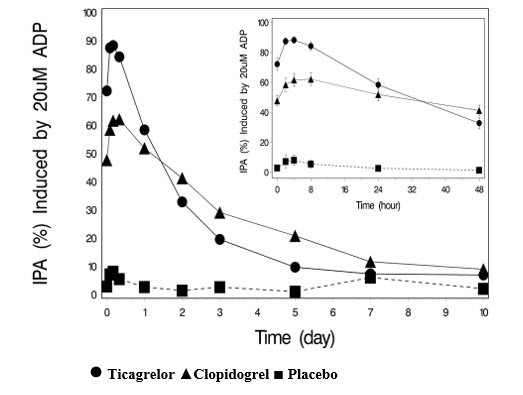
The offset of IPA was examined after 6 weeks on ticagrelor 90 mg twice daily or clopidogrel 75 mg daily, again in response to 20 μM ADP.
As shown in Figure 6, mean maximum IPA following the last dose of ticagrelor was 88% and 62% for clopidogrel. The insert in Figure 6 shows that after 24 hours, IPA in the ticagrelor group (58%) was similar to IPA in clopidogrel group (52%), indicating that patients who miss a dose of ticagrelor would still maintain IPA similar to the trough IPA of patients treated with clopidogrel. After 5 days, IPA in the ticagrelor group was similar to IPA in the placebo group. It is not known how either bleeding risk or thrombotic risk track with IPA, for either ticagrelor or clopidogrel.
Figure 5. Mean inhibition of platelet aggregation (±SE) following single oral doses of placebo, 180 mg ticagrelor or 600 mg clopidogrel:
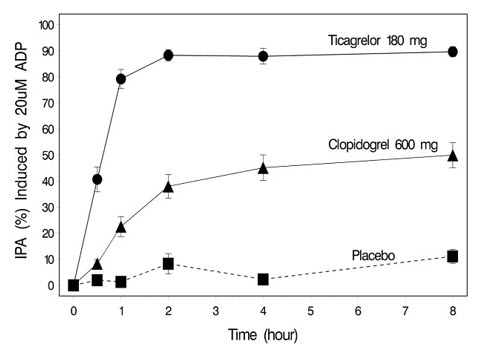
Figure 6. Mean inhibition of platelet aggregation (IPA) following 6 weeks on placebo, ticagrelor 90 mg twice daily, or clopidogrel 75 mg daily:
Transitioning from clopidogrel to BRILINTA resulted in an absolute IPA increase of 26.4% and from BRILINTA to clopidogrel resulted in an absolute IPA decrease of 24.5%. Patients can be transitioned from clopidogrel to BRILINTA without interruption of antiplatelet effect [see Dosage and Administration (2)].
12.3. Pharmacokinetics
Ticagrelor demonstrates dose proportional pharmacokinetics, which are similar in patients and healthy volunteers.
Absorption
BRILINTA can be taken with or without food. Absorption of ticagrelor occurs with a median tmax of 1.5 h (range 1.0–4.0). The formation of the major circulating metabolite AR-C124910XX (active) from ticagrelor occurs with a median tmax of 2.5 h (range 1.5-5.0).
The mean absolute bioavailability of ticagrelor is about 36% (range 30%-42%). Ingestion of a high-fat meal had no effect on ticagrelor Cmax, but resulted in a 21% increase in AUC. The Cmax of its major metabolite was decreased by 22% with no change in AUC.
BRILINTA as crushed tablets mixed in water, given orally or administered through a nasogastric tube into the stomach, is bioequivalent to whole tablets (AUC and Cmax within 80-125% for ticagrelor and AR-C124910XX) with a median tmax of 1.0 hour (range 1.0–4.0) for ticagrelor and 2.0 hours (range 1.0–8.0) for AR-C124910XX.
Distribution
The steady state volume of distribution of ticagrelor is 88 L. Ticagrelor and the active metabolite are extensively bound to human plasma proteins (>99%).
Metabolism
CYP3A4 is the major enzyme responsible for ticagrelor metabolism and the formation of its major active metabolite. Ticagrelor and its major active metabolite are weak P-glycoprotein substrates and inhibitors. The systemic exposure to the active metabolite is approximately 30-40% of the exposure of ticagrelor.
Excretion
The primary route of ticagrelor elimination is hepatic metabolism. When radiolabeled ticagrelor is administered, the mean recovery of radioactivity is approximately 84% (58% in feces, 26% in urine). Recoveries of ticagrelor and the active metabolite in urine were both less than 1% of the dose. The primary route of elimination for the major metabolite of ticagrelor is most likely to be biliary secretion. The mean t1/2 is approximately 7 hours for ticagrelor and 9 hours for the active metabolite.
Specific Populations
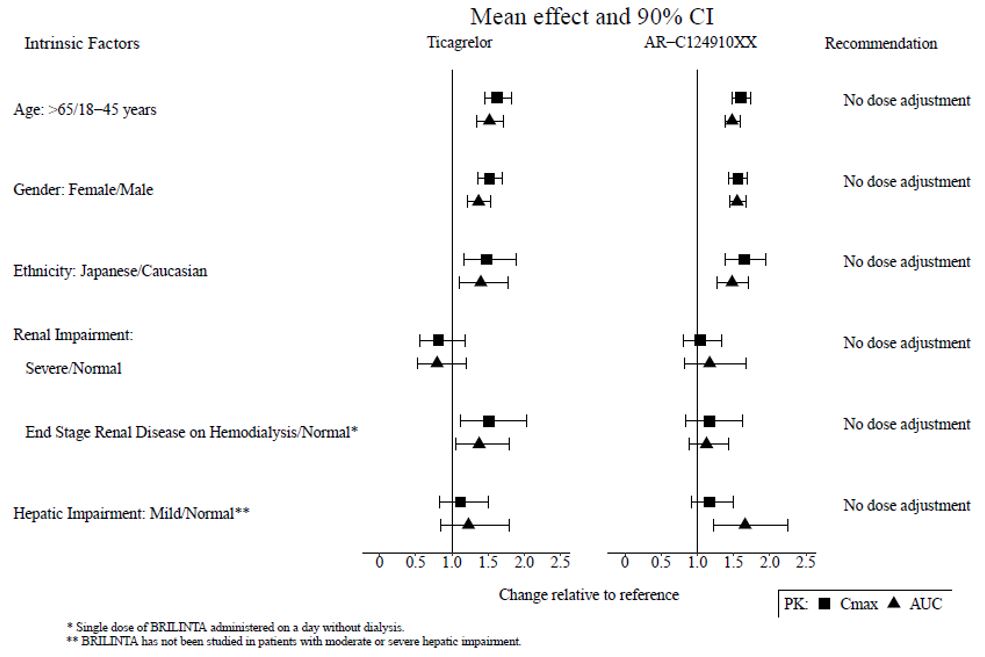
The effects of age, gender, ethnicity, renal impairment and mild hepatic impairment on the pharmacokinetics of ticagrelor are presented in Figure 7. Effects are modest and do not require dose adjustment.
Patients with End-Stage Renal Disease on Hemodialysis
In patients with end stage renal disease on hemodialysis AUC and Cmax of BRILINTA 90 mg administered on a day without dialysis were 38% and 51% higher respectively, compared to subjects with normal renal function. A similar increase in exposure was observed when BRILINTA was administered immediately prior to dialysis showing that BRILINTA is not dialyzable. Exposure of the active metabolite increased to a lesser extent. The IPA effect of BRILINTA was independent of dialysis in patients with end stage renal disease and similar to healthy adults with normal renal function.
Figure 7. Impact of intrinsic factors on the pharmacokinetics of ticagrelor:
Effects of Other Drugs on BRILINTA
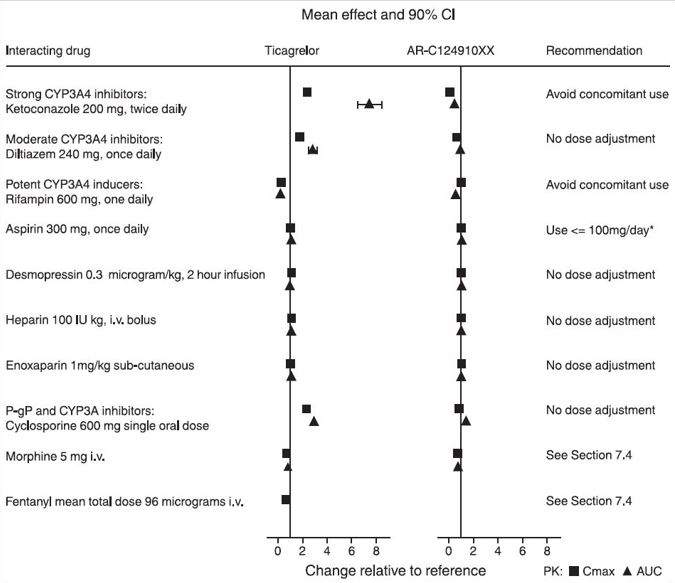
CYP3A4 is the major enzyme responsible for ticagrelor metabolism and the formation of its major active metabolite. The effects of other drugs on the pharmacokinetics of ticagrelor are presented in Figure 8 as change relative to ticagrelor given alone (test/reference). Strong CYP3A inhibitors (e.g., ketoconazole, itraconazole, and clarithromycin) substantially increase ticagrelor exposure. Moderate CYP3A inhibitors have lesser effects (e.g., diltiazem). CYP3A inducers (e.g., rifampin) substantially reduce ticagrelor blood levels. P-gp inhibitors (e.g., cyclosporine) increase ticagrelor exposure.
Co-administration of 5 mg intravenous morphine with 180 mg loading dose of ticagrelor decreased observed mean ticagrelor exposure by up to 25% in healthy adults and up to 36% in ACS patients undergoing PCI. Tmax was delayed by 1-2 hours. Exposure of the active metabolite decreased to a similar extent. Morphine co-administration did not delay or decrease platelet inhibition in healthy adults. Mean platelet aggregation was higher up to 3 hours post loading dose in ACS patients co-administered with morphine.
Co-administration of intravenous fentanyl with 180 mg loading dose of ticagrelor in ACS patients undergoing PCI resulted in similar effects on ticagrelor exposure and platelet inhibition.
Figure 8. Effect of co-administered drugs on the pharmacokinetics of ticagrelor:
* See Dosage and Administration (2)
Effects of BRILINTA on Other Drugs
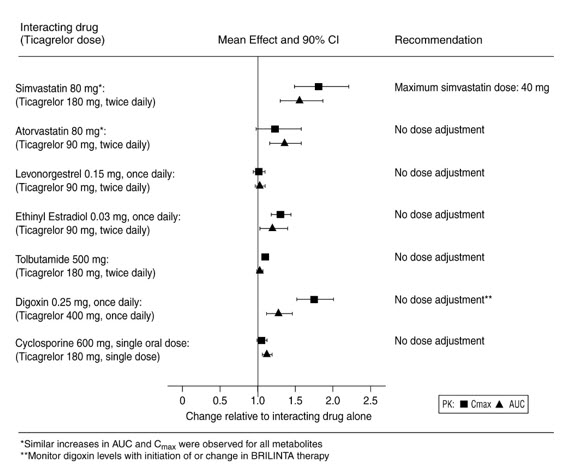
In vitro metabolism studies demonstrate that ticagrelor and its major active metabolite are weak inhibitors of CYP3A4, potential activators of CYP3A5 and inhibitors of the P-gp transporter. Ticagrelor and AR-C124910XX were shown to have no inhibitory effect on human CYP1A2, CYP2C19, and CYP2E1 activity. For specific in vivo effects on the pharmacokinetics of simvastatin, atorvastatin, ethinyl estradiol, levonorgesterol, tolbutamide, digoxin and cyclosporine, see Figure 9.
Figure 9. Impact of BRILINTA on the pharmacokinetics of co-administered drugs:
12.5. Pharmacogenomics
In a genetic substudy cohort of PLATO, the rate of thrombotic CV events in the BRILINTA arm did not depend on CYP2C19 loss of function status.
13.1. Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
Ticagrelor was not carcinogenic in the mouse at doses up to 250 mg/kg/day or in the male rat at doses up to 120 mg/kg/day (19 and 15 times the MRHD of 90 mg twice daily on the basis of AUC, respectively). Uterine carcinomas, uterine adenocarcinomas and hepatocellular adenomas were seen in female rats at doses of 180 mg/kg/day (29‑fold the maximally recommended dose of 90 mg twice daily on the basis of AUC), whereas 60 mg/kg/day (8‑fold the MRHD based on AUC) was not carcinogenic in female rats.
Mutagenesis
Ticagrelor did not demonstrate genotoxicity when tested in the Ames bacterial mutagenicity test, mouse lymphoma assay and the rat micronucleus test. The active O-demethylated metabolite did not demonstrate genotoxicity in the Ames assay and mouse lymphoma assay.
Impairment of Fertility
Ticagrelor had no effect on male fertility at doses up to 180 mg/kg/day or on female fertility at doses up to 200 mg/kg/day (>15-fold the MRHD on the basis of AUC). Doses of ≥10 mg/kg/day given to female rats caused an increased incidence of irregular duration estrus cycles (1.5-fold the MRHD based on AUC).
14. Clinical Studies
14.1 Acute Coronary Syndromes and Secondary Prevention after Myocardial Infarction
PLATO
PLATO (NCT00391872) was a randomized double-blind study comparing BRILINTA (N=9333) to clopidogrel (N=9291), both given in combination with aspirin and other standard therapy, in patients with acute coronary syndromes (ACS), who presented within 24 hours of onset of the most recent episode of chest pain or symptoms. The study's primary endpoint was the composite of first occurrence of cardiovascular death, non-fatal MI (excluding silent MI), or non-fatal stroke.
Patients who had already been treated with clopidogrel could be enrolled and randomized to either study treatment. Patients with previous intracranial hemorrhage, gastrointestinal bleeding within the past 6 months, or with known bleeding diathesis or coagulation disorder were excluded. Patients taking anticoagulants were excluded from participating and patients who developed an indication for anticoagulation during the trial were discontinued from study drug. Patients could be included whether there was intent to manage the ACS medically or invasively, but patient randomization was not stratified by this intent.
All patients randomized to BRILINTA received a loading dose of 180 mg followed by a maintenance dose of 90 mg twice daily. Patients in the clopidogrel arm were treated with an initial loading dose of clopidogrel 300 mg, if clopidogrel therapy had not already been given. Patients undergoing PCI could receive an additional 300 mg of clopidogrel at investigator discretion. A daily maintenance dose of aspirin 75-100 mg was recommended, but higher maintenance doses of aspirin were allowed according to local judgment. Patients were treated for at least 6 months and for up to 12 months.
PLATO patients were predominantly male (72%) and Caucasian (92%). About 43% of patients were >65 years and 15% were >75 years. Median exposure to study drug was 276 days. About half of the patients received pre-study clopidogrel and about 99% of the patients received aspirin at some time during PLATO. About 35% of patients were receiving a statin at baseline and 93% received a statin sometime during PLATO.
Table 7 shows the study results for the primary composite endpoint and the contribution of each component to the primary endpoint. Separate secondary endpoint analyses are shown for the overall occurrence of CV death, MI, and stroke and overall mortality.
Table 7. Patients with outcome events (PLATO):
| BRILINTA* N=9333 | Clopidogrel N=9291 | Hazard Ratio (95% CI) | p-value | |
|---|---|---|---|---|
| Events / 1000 patient years | Events / 1000 patient years | |||
| Composite of CV death, MI, or stroke | 111 | 131 | 0.84 (0.77, 0.92) | 0.0003 |
| CV death | 32 | 43 | 0.74 | |
| Non-fatal MI | 64 | 76 | 0.84 | |
| Non-fatal stroke | 15 | 12 | 1.24 | |
| Secondary endpoints† | ||||
| CV death | 45 | 57 | 0.79 (0.69, 0.91) | 0.0013 |
| MI‡ | 65 | 76 | 0.84 (0.75, 0.95) | 0.0045 |
| Stroke‡ | 16 | 14 | 1.17 (0.91, 1.52) | 0.22 |
| All-cause mortality | 51 | 65 | 0.78 (0.69, 0.89) | 0.0003 |
* Dosed at 90 mg bid.
† Note: rates of first events for the components CV Death, MI and Stroke are the actual rates for first events for each component and do not add up to the overall rate of events in the composite endpoint.
‡ Including patients who could have had other non-fatal events or died.
The Kaplan-Meier curve (Figure 10) shows time to first occurrence of the primary composite endpoint of CV death, non-fatal MI or non-fatal stroke in the overall study.
Figure 10. Time to first occurrence of CV death, MI, or stroke (PLATO):
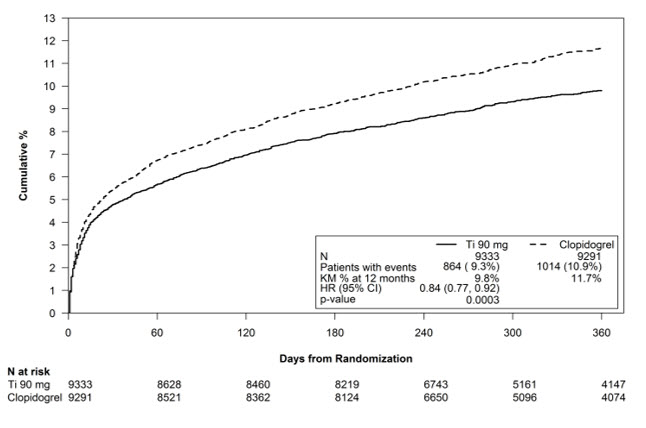
The curves separate by 30 days [relative risk reduction (RRR) 12%] and continue to diverge throughout the 12‑month treatment period (RRR 16%).
Among 11,289 patients with PCI receiving any stent during PLATO, there was a lower risk of stent thrombosis (1.3% for adjudicated "definite") than with clopidogrel (1.9%) (HR 0.67, 95% CI 0.50-0.91; p=0.009). The results were similar for drug-eluting and bare metal stents.
A wide range of demographic, concurrent baseline medications, and other treatment differences were examined for their influence on outcome. Some of these are shown in Figure 11. Such analyses must be interpreted cautiously, as differences can reflect the play of chance among a large number of analyses. Most of the analyses show effects consistent with the overall results, but there are two exceptions: a finding of heterogeneity by region and a strong influence of the maintenance dose of aspirin. These are considered further below.
Most of the characteristics shown are baseline characteristics, but some reflect post-randomization determinations (e.g., aspirin maintenance dose, use of PCI).
Figure 11. Subgroup analyses of (PLATO):
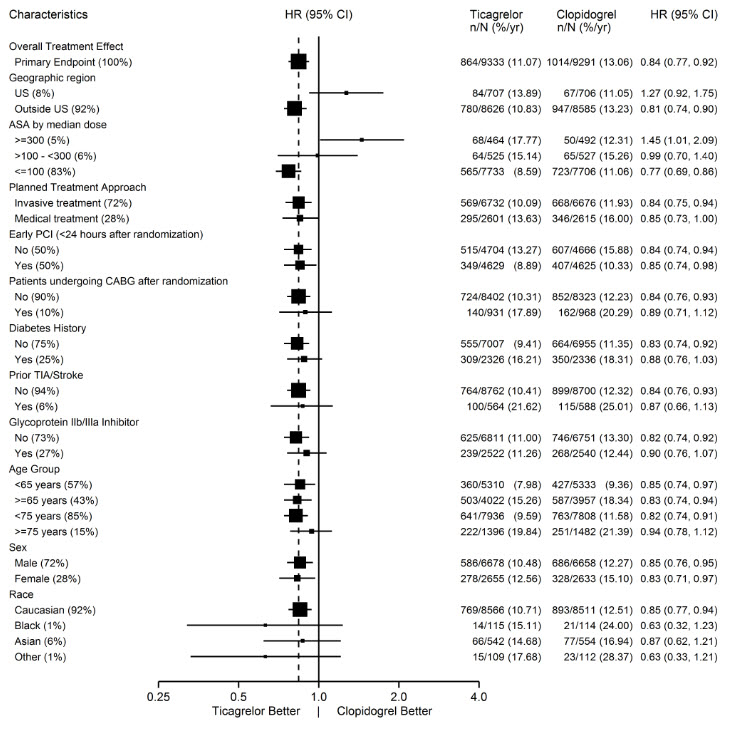
Note: The figure above presents effects in various subgroups most of which are baseline characteristics and most of which were pre-specified. The 95% confidence limits that are shown do not take into account how many comparisons were made, nor do they reflect the effect of a particular factor after adjustment for all other factors. Apparent homogeneity or heterogeneity among groups should not be over-interpreted.
Regional Differences
Results in the rest of the world compared to effects in North America (US and Canada) show a smaller effect in North America, numerically inferior to the control and driven by the US subset. The statistical test for the US/non-US comparison is statistically significant (p=0.009), and the same trend is present for both CV death and non-fatal MI. The individual results and nominal p-values, like all subset analyses, need cautious interpretation, and they could represent chance findings. The consistency of the differences in both the CV mortality and non-fatal MI components, however, supports the possibility that the finding is reliable.
A wide variety of baseline and procedural differences between the US and non-US (including intended invasive vs. planned medical management, use of GPIIb/IIIa inhibitors, use of drug eluting vs. bare-metal stents) were examined to see if they could account for regional differences, but with one exception, aspirin maintenance dose, these differences did not appear to lead to differences in outcome.
Aspirin Dose
The PLATO protocol left the choice of aspirin maintenance dose up to the investigator and use patterns were different in US sites from sites outside of the US. About 8% of non-US investigators administered aspirin doses above 100 mg, and about 2% administered doses above 300 mg. In the US, 57% of patients received doses above 100 mg and 54% received doses above 300 mg. Overall results favored BRILINTA when used with low maintenance doses (≤100 mg) of aspirin, and results analyzed by aspirin dose were similar in the US and elsewhere. Figure 10 shows overall results by median aspirin dose. Figure 12 shows results by region and dose.
Figure 12. CV death, MI, stroke by maintenance aspirin dose in the US and outside the US (PLATO):
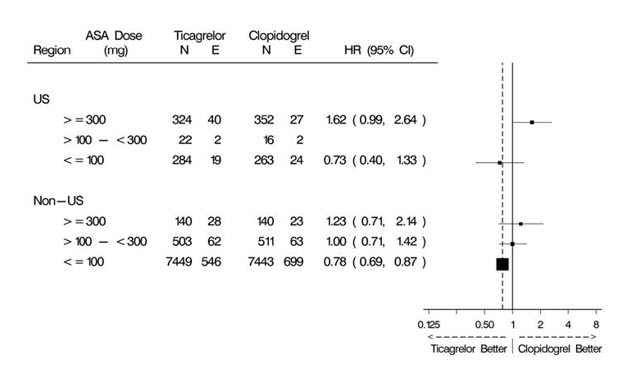
Like any unplanned subset analysis, especially one where the characteristic is not a true baseline characteristic (but may be determined by usual investigator practice), the above analyses must be treated with caution. It is notable, however, that aspirin dose predicts outcome in both regions with a similar pattern, and that the pattern is similar for the two major components of the primary endpoint, CV death and non-fatal MI.
Despite the need to treat such results cautiously, there appears to be good reason to restrict aspirin maintenance dosage accompanying ticagrelor to 100 mg. Higher doses do not have an established benefit in the ACS setting, and there is a strong suggestion that use of such doses reduces the effectiveness of BRILINTA.
PEGASUS
The PEGASUS TIMI-54 study (NCT01225562) was a 21,162-patient, randomized, double-blind, placebo-controlled, parallel-group study. Two doses of ticagrelor, either 90 mg twice daily or 60 mg twice daily, co-administered with 75-150 mg of aspirin, were compared to aspirin therapy alone in patients with history of MI. The primary endpoint was the composite of first occurrence of CV death, non-fatal MI and non-fatal stroke. CV death and all-cause mortality were assessed as secondary endpoints.
Patients were eligible to participate if they were ≥50 years old, with a history of MI 1 to 3 years prior to randomization, and had at least one of the following risk factors for thrombotic cardiovascular events: age ≥65 years, diabetes mellitus requiring medication, at least one other prior MI, evidence of multivessel coronary artery disease, or creatinine clearance <60 mL/min. Patients could be randomized regardless of their prior ADP receptor blocker therapy or a lapse in therapy. Patients requiring or who were expected to require renal dialysis during the study were excluded. Patients with any previous intracranial hemorrhage, gastrointestinal bleeding within the past 6 months, or with known bleeding diathesis or coagulation disorder were excluded. Patients taking anticoagulants were excluded from participating and patients who developed an indication for anticoagulation during the trial were discontinued from study drug. A small number of patients with a history of stroke were included. Based on information external to PEGASUS, 102 patients with a history of stroke (90 of whom received study drug) were terminated early and no further such patients were enrolled.
Patients were treated for at least 12 months and up to 48 months with a median follow up time of 33 months.
Patients were predominantly male (76%) Caucasian (87%) with a mean age of 65 years, and 99.8% of patients received prior aspirin therapy.
The Kaplan-Meier curve (Figure 13) shows time to first occurrence of the primary composite endpoint of CV death, non-fatal MI or non-fatal stroke.
Figure 13. Time to First Occurrence of CV death, MI or Stroke (PEGASUS):
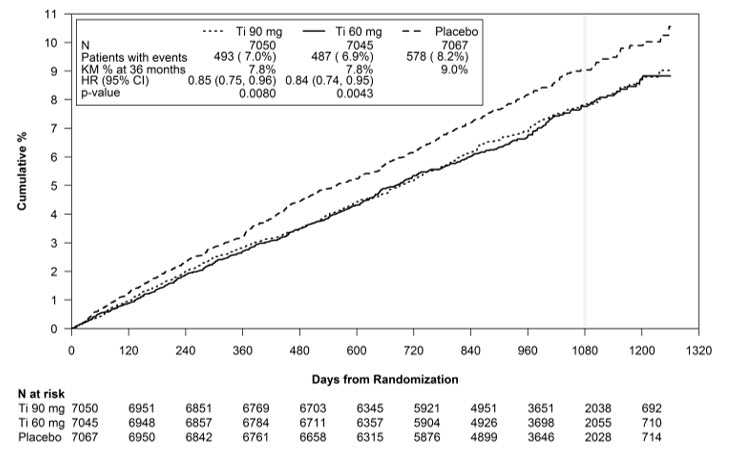
Ti = Ticagrelor BID, CI = Confidence interval; HR = Hazard ratio; KM = Kaplan-Meier; N = Number of patients.
Both the 60 mg and 90 mg regimens of BRILINTA in combination with aspirin were superior to aspirin alone in reducing the incidence of CV death, MI or stroke. The absolute risk reductions for BRILINTA plus aspirin vs. aspirin alone were 1.27% and 1.19% for the 60 and 90 mg regimens, respectively. Although the efficacy profiles of the two regimens were similar, the lower dose had lower risks of bleeding and dyspnea.
Table 8 shows the results for the 60 mg plus aspirin regimen vs. aspirin alone.
Table 8. Incidences of the primary composite endpoint, primary composite endpoint components, and secondary endpoints (PEGASUS):
| BRILINTA* N=7045 | Placebo N=7067 | HR (95% CI) | p-value | |
|---|---|---|---|---|
| Events / 1000 patient years | Events / 1000 patient years | |||
| Time to first CV death, MI, or stroke† | 26 | 31 | 0.84 (0.74, 0.95) | 0.0043 |
| CV Deathठ| 9 | 11 | 0.83 (0.68, 1.01) | |
| Myocardial infarction§ | 15 | 18 | 0.84 (0.72, 0.98) | |
| Stroke§ | 5 | 7 | 0.75 (0.57, 0.98) | |
| All-cause mortality‡ | 16 | 18 | 0.89 (0.76, 1.04) |
CI = Confidence interval; CV = Cardiovascular; HR = Hazard ratio; MI = Myocardial infarction; N = Number of patients.
* 60 mg BID
† Primary composite endpoint
‡ Secondary endpoints
§ The event rate for the components CV death, MI and stroke are calculated from the actual number of first events for each component.
In PEGASUS, the relative risk reduction (RRR) for the composite endpoint from 1 to 360 days (17% RRR) and from 361 days and onwards (16% RRR) were similar.
The treatment effect of BRILINTA 60 mg over aspirin appeared similar across most pre-defined subgroups, see Figure 14.
Figure 14. Subgroup analyses of ticagrelor 60 mg (PEGASUS):
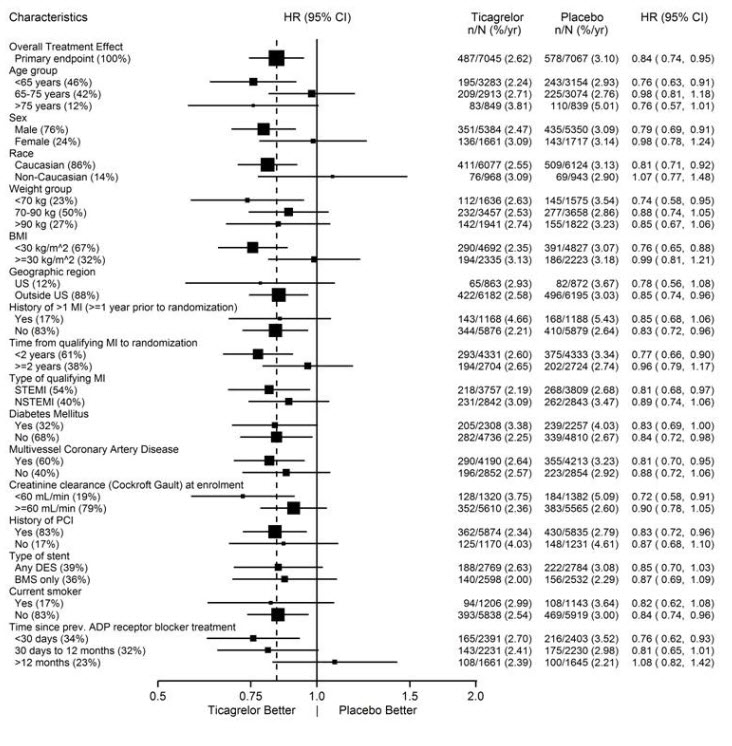
Note: The figure above presents effects in various subgroups all of which are baseline characteristics and most of which were pre-specified. The 95% confidence limits that are shown do not take into account how many comparisons were made, nor do they reflect the effect of a particular factor after adjustment for all other factors. Apparent homogeneity or heterogeneity among groups should not be over-interpreted.
14.2 Coronary Artery Disease but No Prior Stroke or Myocardial Infarction
THEMIS
The THEMIS study (NCT01991795) was a double-blind, parallel group, study in which 19,220 patients with CAD and Type 2 Diabetes Mellitus (T2DM) but no history of MI or stroke were randomized to twice daily BRILINTA or placebo, on a background of 75-150 mg of aspirin. The primary endpoint was the composite of first occurrence of CV death, MI, and stroke. CV death, MI, ischemic stroke, and all-cause death were assessed as secondary endpoints.
Patients were eligible to participate if they were ≥50 years old with CAD, defined as a history of PCI or CABG, or angiographic evidence of ≥50% lumen stenosis of at least 1 coronary artery and T2DM treated for at least 6 months with glucose-lowering medication. Patients with previous intracerebral hemorrhage, gastrointestinal bleeding within the past 6 months, known bleeding diathesis, and coagulation disorder were excluded. Patients taking anticoagulants or ADP receptor antagonists were excluded from participating, and patients who developed an indication for those medications during the trial were discontinued from study drug.
Patients were treated for a median of 33 months and up to 58 months.
Patients were predominantly male (69%) with a mean age of 66 years. At baseline, 80% had a history of coronary artery revascularization; 58% had undergone PCI, 29% had undergone a CABG and 7% had undergone both. The proportion of patients studied in the US was 12%. Patients in THEMIS had established CAD and other risk factors that put them at higher cardiovascular risk.
BRILINTA was superior to placebo in reducing the incidence of CV death, MI, or stroke. The effect on the composite endpoint was driven by the individual components MI and stroke; see Table 9.
Table 9. Primary composite endpoint, primary endpoint components, and secondary endpoints (THEMIS):
| BRILINTA N=9619 | Placebo N=9601 | HR (95% CI) | p-value | |
|---|---|---|---|---|
| Events / 1000 patient years | Events / 1000 patient years | |||
| Time to first CV death, MI, or stroke* | 24 | 27 | 0.90 (0.81, 0.99) | 0.04 |
| CV death† | 12 | 11 | 1.02 (0.88, 1.18) | |
| Myocardial infarction† | 9 | 11 | 0.84 (0.71, 0.98) | |
| Stroke† | 6 | 7 | 0.82 (0.67, 0.99) | |
| Secondary endpoints | ||||
| CV death | 12 | 11 | 1.02 (0.88, 1.18) | |
| Myocardial infarction | 9 | 11 | 0.84 (0.71, 0.98) | |
| Ischemic stroke | 5 | 6 | 0.80 (0.64, 0.99) | |
| All-cause death | 18 | 19 | 0.98 (0.87, 1.10) | |
CI = Confidence interval; CV = Cardiovascular; HR = Hazard ratio; MI = Myocardial infarction.
* Primary endpoint
† The event rate for the components CV death, MI and stroke are calculated from the actual number of first events for each component.
The Kaplan-Meier curve (Figure 15) shows time to first occurrence of the primary composite endpoint of CV death, MI, or stroke.
Figure 15. Time to First Occurrence of CV death, MI or Stroke (THEMIS):
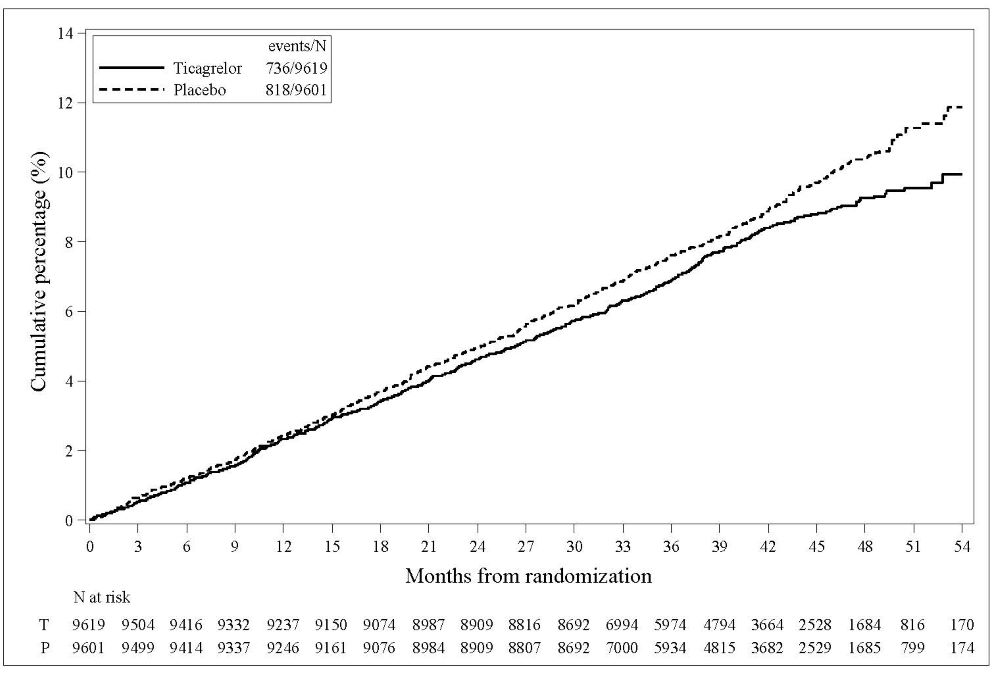
T = Ticagrelor; P = Placebo; N = Number of patients.
The treatment effect of BRILINTA appeared similar across patient subgroups, see Figure 16.
Figure 16. Subgroup analyses of ticagrelor (THEMIS):
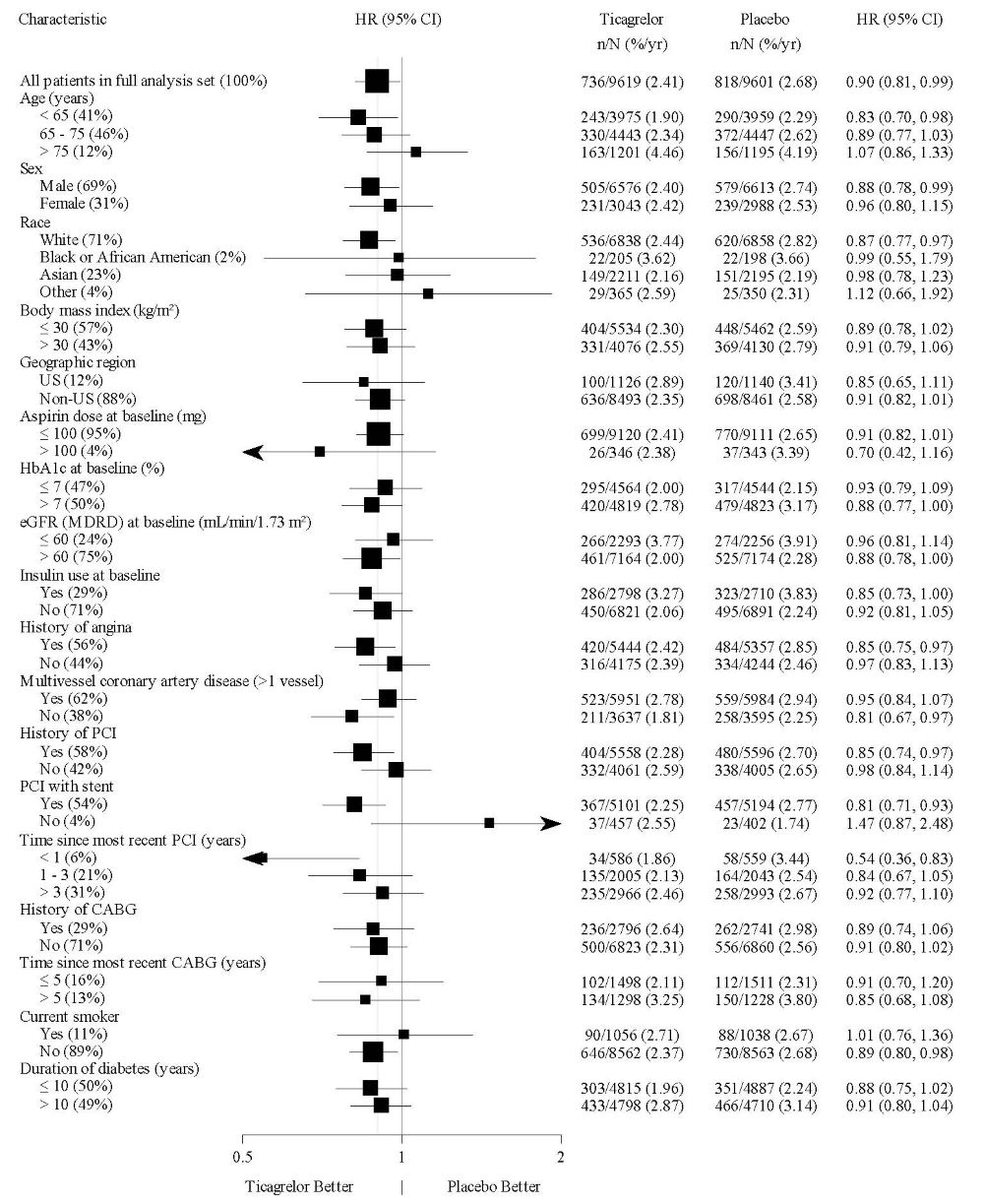
Note: The figure above presents effects in various subgroups all of which are baseline characteristics. The 95% confidence limits that are shown do not take into account how many comparisons were made, nor do they reflect the effect of a particular factor after adjustment for all other factors. Apparent homogeneity or heterogeneity among groups should not be over-interpreted.
14.3 Acute Ischemic Stroke or Transient Ischemic Attack (TIA)
THALES
The THALES study (NCT03354429) was a 11016-patient, randomized, double-blind, parallel-group study of BRILINTA 90 mg twice daily versus placebo in patients with acute ischemic stroke or transient ischemic attack (TIA). The primary endpoint was the first occurrence of the composite of stroke and death up to 30 days. Ischemic stroke was assessed as one of the secondary endpoints.
Patients were eligible to participate if they were ≥40 years old, with non-cardioembolic acute ischemic stroke (NIHSS score ≤5) or high-risk TIA (defined as ABCD2 score ≥6 or ipsilateral atherosclerotic stenosis ≥50% in the internal carotid or an intracranial artery). Patients who received thrombolysis or thrombectomy within 24 hours prior to randomization were not eligible.
Patients were randomized within 24 hours of onset of an acute ischemic stroke or TIA to receive 30 days of either BRILINTA (90 mg twice daily, with an initial loading dose of 180 mg) or placebo, on a background of aspirin initially 300-325 mg then 75-100 mg daily. The median treatment duration was 31 days.
BRILINTA was superior to placebo in reducing the rate of the primary endpoint (composite of stroke and death), corresponding to a relative risk reduction (RRR) of 17% and an absolute risk reduction (ARR) of 1.1% (Table 10). The effect was driven primarily by a significant reduction in the stroke component of the primary endpoint (19% RRR, 1.1% ARR).
Table 10. Incidences of the primary composite endpoint, primary composite endpoint components, and secondary endpoint (THALES):
| BRILINTA N=5523 | Placebo N=5493 | HR (95% CI) | p-value | |||
|---|---|---|---|---|---|---|
| n (patients with event) | KM% | n (patients with event) | KM% | |||
| Time to first Stroke or Death | 303 | 5.4% | 362 | 6.5% | 0.83 (0.71, 0.96) | 0.015 |
| Time to first Stroke* | 284 | 5.1% | 347 | 6.3% | 0.81 (0.69, 0.95) | |
| Time to Death* | 36 | 0.6% | 27 | 0.5% | 1.33 (0.81, 2.19) | |
| Secondary Endpoint | ||||||
| Time to first Ischemic Stroke | 276 | 5.0% | 345 | 6.2% | 0.79 (0.68, 0.93) | 0.004 |
CI = Confidence interval; HR = Hazard ratio; KM = Kaplan-Meier percentage calculated at 30 days; N = Number of patients
*
The Kaplan-Meier curve (Figure 17) shows the time to first occurrence of the primary composite endpoint of stroke and death.
Figure 17. Time to First Occurrence of Stroke or Death (THALES):
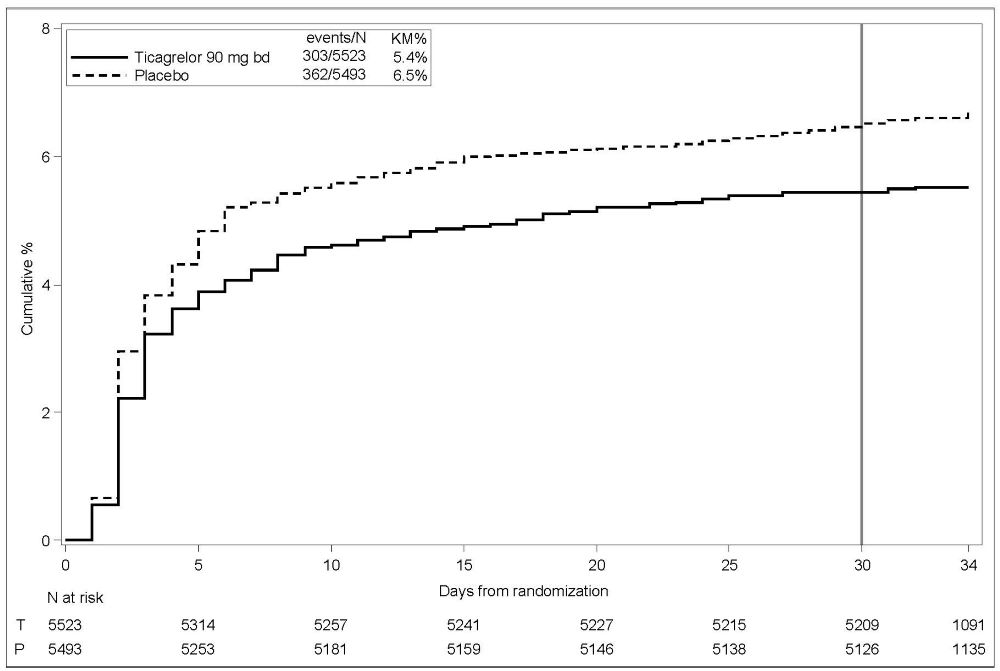
KM%: Kaplan-Meier percentage evaluated at Day 30; T=Ticagrelor; P=placebo; N=Number of patients
BRILINTA's treatment effect on stroke and on death accrued over the first 10 days and was sustained at 30 days. Although not studied, this suggests that shorter treatment could result in similar benefit and reduced bleeding risk.
The treatment effect of BRILINTA was generally consistent across pre-defined subgroups (Figure 18).
Figure 18. Subgroup analyses of ticagrelor 90 mg (THALES):
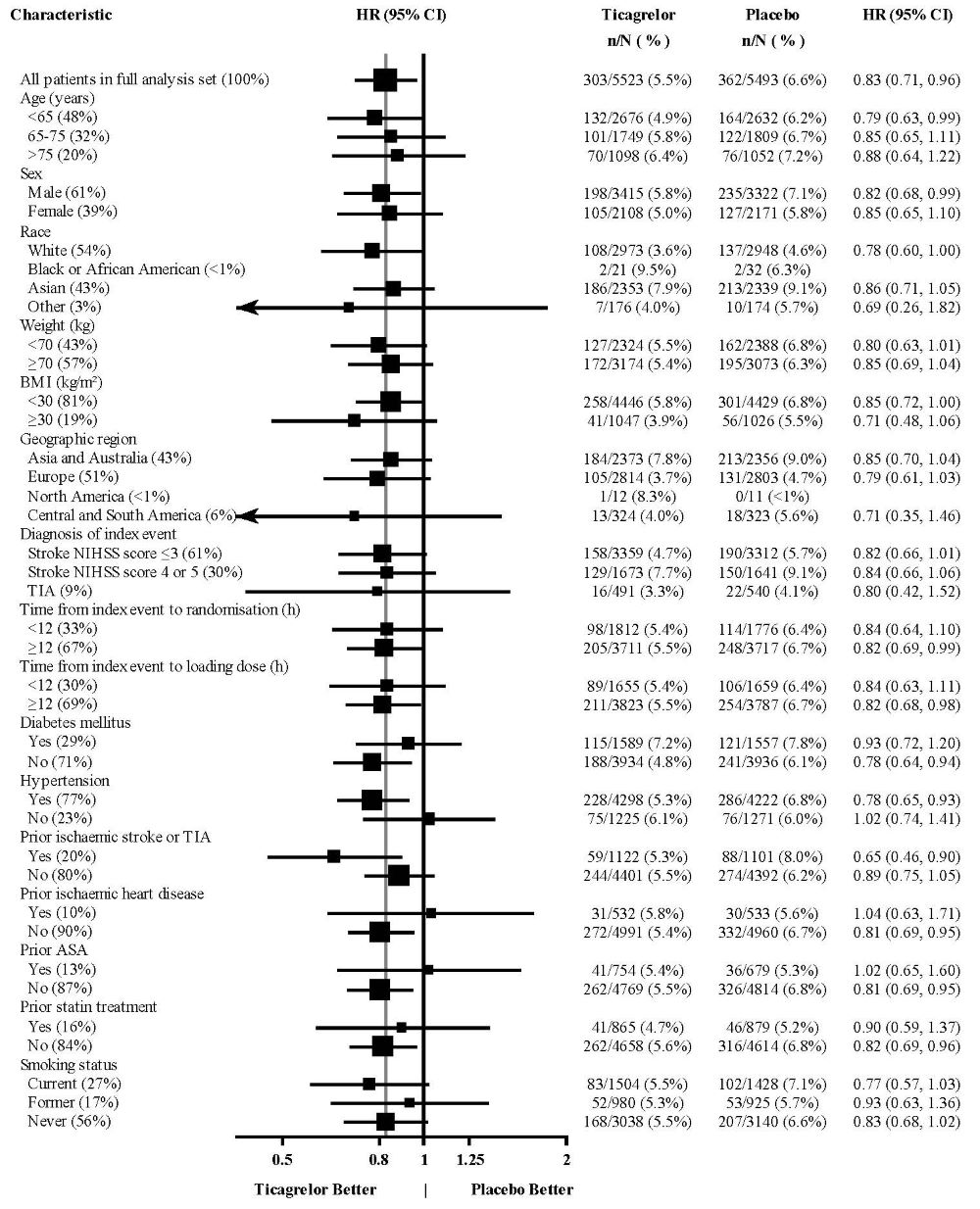
Note: The figure above presents effects in various subgroups all of which are baseline characteristics and were pre-specified. The 95% confidence limits that are shown do not take into account how many comparisons were made, nor do they reflect the effect of a particular factor after adjustment for all other factors. Apparent homogeneity or heterogeneity among groups should not be over-interpreted.
At Day 30, there was an absolute reduction of 1.2% (95% CI: -2.1%, -0.3%) in the incidence of non-hemorrhagic stroke and death (excluding fatal bleed) favoring ticagrelor (294 events: 5.3%) over placebo (359 events: 6.5%) in the intention-to-treat population. In the same population, there was an absolute increase of 0.4% (95% CI: 0.2%, 0.6%) in the incidence of GUSTO severe bleeding unfavorable to ticagrelor arm (28 events: 0.5%) compared to the placebo arm (7 events: 0.1%).
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.