BYLVAY Hard capsule Ref.[27935] Active ingredients: Odevixibat
Source: European Medicines Agency (EU) Revision Year: 2025 Publisher: Ipsen Pharma, 65 quai Georges Gorse, 92100 Boulogne-Billancourt, France
5.1. Pharmacodynamic properties
Pharmacotherapeutic group: Bile and liver therapy, other drugs for bile therapy
ATC code: A05AX05
Mechanism of action
Odevixibat is a reversible, potent, selective inhibitor of the ileal bile acid transporter (IBAT).
Pharmacodynamic effects
Odevixibat acts locally in the distal ileum to decrease the reuptake of bile acids and increase the clearance of bile acids through the colon, reducing the concentration of bile acids in the serum. The extent of reduction of serum bile acids does not correlate with systemic PK.
Clinical efficacy
The efficacy of Bylvay in patients with PFIC was evaluated in two phase 3 trials. Trial 1 was a 24-week, randomised, double-blind, placebo-controlled trial conducted in 62 patients with a confirmed diagnosis of PFIC Type 1 or Type 2. Patients were randomised 1:1:1 to placebo, or 40 or 120 mcg/kg/day odevixibat and stratified by PFIC Type (1 or 2) and age (6 months to 5 years, 6 to 12 years, and 13 to ≤18 years). Patients with pathologic variations of the ABCB11 gene that predict complete absence of the BSEP protein and those with ALT >10 × ULN or bilirubin >10 × ULN were excluded. 13% of the patients had prior biliary diversion surgery. Patients completing Trial 1 were eligible to enrol in Trial 2, a 72-week open-label extension trial. The primary endpoint in Trial 1 was the proportion of patients with at least a 70% reduction in fasting serum bile acid levels or who achieved a level ≤70 µmol/L at week 24.
The proportion of positive pruritus assessments at the patient level over the 24-week treatment period based on an observer-reported outcome (ObsRO) instrument was a secondary endpoint. A positive pruritus assessment was a score of ≤1 or at least 1-point improvement from baseline. Pruritus assessments were conducted in the morning and evening using a 5-point scale (0-4). Additional secondary endpoints included changes from baseline to end of treatment in growth, sleep parameters (per ObsRO) and ALT.
Median (range) age of patients in Trial 1 was 3.2 (0.5 to 15.9) years; 50% were male and 84% were white. 27% of patients had PFIC Type 1 and 73% had PFIC Type 2. At baseline, 81% of patients were treated with UDCA, 66% with rifampicin, and 89% with UDCA and/or rifampicin. Baseline hepatic impairment per Child-Pugh classification was mild in 66% and moderate in 34% of patients. Baseline mean (SD) eGFR was 164 (30.6) mL/min/1.73 m². Baseline mean (SD) ALT, AST and bilirubin levels were 99 (116.8) U/L, 101 (69.8) U/L, and 3.2 (3.57) mg/dL, respectively. Baseline mean (SD) pruritus score (range: 0-4) and serum bile acids levels were similar in odevixibat-treated patients (2.9 [0.089] and 252.1 [103.0] µmol/L, respectively) and placebo-treated patients (3.0 [0.143] and 247.5 [101.1] µmol/L, respectively).
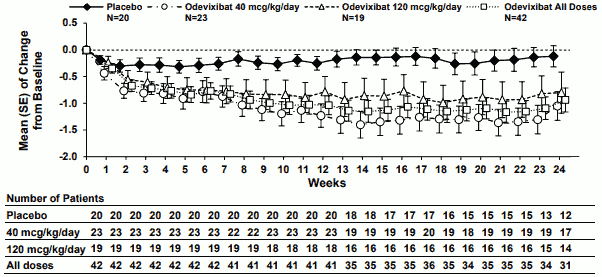
Table 4 presents the results of the comparison of the key efficacy results in Trial 1 between odevixibat and placebo. These data are displayed graphically over the 24-week treatment period in Figure 1 (serum bile acids) and Figure 2 (scratching scores).
Table 4. Comparison of key efficacy results for odevixibat vs. placebo over the 24-week treatment period in patients with PFIC in trial 1:
| Efficacy endpoint | Placebo (N=20) | Odevixibat | ||
|---|---|---|---|---|
| 40 mcg/kg/day (N=23) | 120 mcg/kg/day (N=19) | Total (N=42) | ||
| Proportion of patients with reduction in serum bile acids at end of treatment | ||||
| n (%) (95% CI) | 0 (0.00, 16.84) | 10 (43.5) (23.19, 65.51) | 4 (21.1) (6.05, 45.57) | 14 (33.3) (19.57, 49.55) |
| Difference in proportion vs. placebo (95% CI) | 0.44 (0.22, 0.66) | 0.21 (0.02, 0.46) | 0.33 (0.09, 0.50) | |
| One-sided p-valuea | 0.0015 | 0.0174 | 0.0015 | |
| Proportion of positive pruritus assessments over the treatment period | ||||
| Proportion | 28.74 | 58.31 | 47.69 | 53.51 |
| Difference in proportion (SE) vs. placebo (95% CI)b | 28.23 (9.18) (9.83, 46.64) | 21.71 (9.89) (1.87, 41.54) | 24.97 (8.24) (8.45, 41.49) | |
a Based on Cochran Mantel Haenszel test stratified by PFIC Type. P-values for the dose groups are adjusted for multiplicity.
b Based on least squares means from an analysis of covariance model with daytime and night-time baseline pruritus scores as covariates and treatment group and stratification factors (PFIC Type and age category) as fixed effects.
Figure 1. Mean (±SE) change from baseline in serum bile acid concentration (µmol/L) over time:
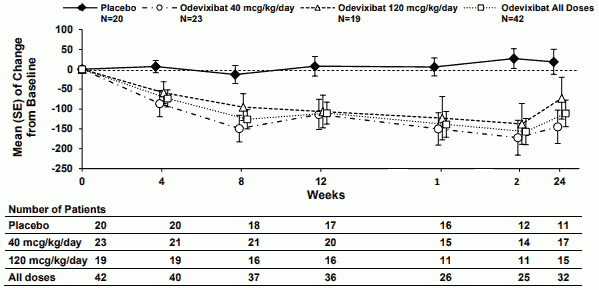
Figure 2. Mean (±SE) change from baseline in pruritus (scratching) severity score over time:
In line with the results for reduction of pruritus (scratching), odevixibat reduced the percentage of days the patient required soothing, and patients less often required help falling asleep and had fewer days needing to sleep with a caregiver. Treatment with odevixibat also led to improvements from baseline in liver function test results (Table 5). The effect of odevixibat on growth parameters over 24 weeks is also presented.
Table 5. Comparison of efficacy results for growth and hepatic biochemical parameters for odevixibat vs. placebo over the 24-week treatment period in patients with PFIC in trial 1:
| Efficacy endpoint | Placebo (N=20) | Odevixibat | ||
|---|---|---|---|---|
| 40 mcg/kg/day (N=23) | 120 mcg/kg/day (N=19) | Total (N=42) | ||
| Alanine aminotransferase (U/L) (mean [SE]) | ||||
| Baseline | 76.9 (12.57) | 127.7 (34.57) | 89.1 (19.95) | 110.2 (20.96) |
| Change to Week 24 | 3.7 (4.95) | -27.9 (17.97) | -25.3 (22.47) | -26.7 (13.98) |
| Mean difference vs. placebo (95% CI)a | -14.8 (16.63) (-48.3, 18.7) | -14.9 (17.25) (-49.6, 19.9) | -14.8 (15.05) (-45.1, 15.4) | |
| Aspartate aminotransferase (U/L) (mean [SE]) | ||||
| Baseline | 90.2 (11.59) | 114.2 (17.24) | 96.0 (16.13) | 106.0 (11.87) |
| Change to Week 24 | 4.7 (5.84) | -36.7 (12.21) | -27.0 (19.42) | -32.1 (11.02) |
| Total bilirubin (µmol/L) (mean [SE]) | ||||
| Baseline | 53.3 (12.97) | 52.2 (10.13) | 57.0 (18.05) | 54.4 (9.75) |
| Change to Week 24 | -9.6 (15.16) | -23.7 (9.23) | -19.3 (13.62) | -21.7 (7.92) |
| Height z-scores (mean [SE]) | ||||
| Baseline | -2.26 (0.34) | -1.45 (0.27) | -2.09 (0.37) | -1.74 (0.23) |
| Change to Week 24 | -0.16 (0.10) | 0.05 (0.11) | 0.00 (0.16) | 0.03 (0.09) |
| Mean difference vs. placebo (95% CI)a | 0.32 (0.16) (0.00, 0.65) | 0.15 (0.17) (-0.18, 0.48) | 0.24 (0.14) (-0.05, 0.53) | |
| Weight z-scores (mean [SE]) | ||||
| Baseline | -1.52 (0.32) | -0.74 (0.27) | -1.19 (0.35) | -0.94 (0.21) |
| Change to Week 24 | 0.10 (0.10) | 0.29 (0.11) | 0.15 (0.12) | 0.22 (0.08) |
| Mean difference vs. placebo (95% CI)a | 0.28 (0.14) (-0.01, 0.57) | 0.08 (0.15) (-0.22, 0.37) | 0.18 (0.13) (-0.08, 0.44) | |
a Based on least squares means from a mixed model for repeated measures (MMRM) with baseline value as a covariate, and treatment group, visit, treatment-by-visit interaction, treatment-by-baseline interaction and stratification factors (PFIC type and age category) as fixed effects.
Trial 2 is an interim cut of data from an ongoing 72-week open-label extension trial in PFIC patients treated with Bylvay 120 mcg/kg/day. The 79 patients (PFIC1 [22%], PFIC2 [51%], PFIC3 [5%] or PFIC6 [1%]) treated with 120 mcg/kg/day for up to 48 weeks experienced a durable effect on serum bile acids reduction, improvement in pruritus score, ALT, AST and total bilirubin. Across the 79 patients, 45 had assessments on or after 48 weeks of treatment with odevixibat, including 13, 30, 1 and 1 patients with PFIC1, PFIC2, PFIC3, and PFIC6, respectively; 9, 21, 4, and 0 patients, respectively, had not reached 48 weeks of treatment and were ongoing at the data cut-off. Overall, 7 patients with PFIC2 had discontinued prior to 48 weeks of treatment with odevixibat. Improvements in z-scores for height and weight indicate an enhanced growth velocity and the potential for catch-up growth in actively growing children.
Paediatric population
The European Medicines Agency has deferred the obligation to submit the results of studies with Bylvay in paediatric population less than 6 months; see section 4.2 for information on paediatric use.
Exceptional circumstances
This medicinal product has been authorised under 'Exceptional Circumstances'. This means that due to the rarity of the disease it has not been possible to obtain complete information on this medicinal product. The European Medicines Agency will review any new information which may become available every year and this SmPC will be updated as necessary.
5.2. Pharmacokinetic properties
Absorption
Odevixibat is minimally absorbed following oral administration; absolute bioavailability data in humans are not available, and estimated relative bioavailability is <1%. Peak odevixibat plasma concentration (Cmax) is reached within 1 to 5 hours. Simulated Cmax values in a paediatric PFIC patient population for the 40 and 120 mcg/kg/day doses are 0.211 ng/mL and 0.623 ng/mL, respectively, and AUC values were 2.26 ng × h/mL and 5.99 ng × h/mL, respectively. There is minimal accumulation of odevixibat following once-daily dosing.
Effect of food
Systemic exposure of odevixibat does not predict efficacy. Therefore, no dose adjustment for food effects is considered necessary. Concomitant administration of a high-fat meal (800-1000 calories with approximately 50% of total caloric content of the meal from fat) resulted in decreases of approximately 72% and 62% in Cmax and AUC0-24, respectively, compared to administration under fasted conditions. When odevixibat was sprinkled on apple sauce, decreases of approximately 39% and 36% in Cmax and AUC0-24, respectively, were observed compared to administration under fasted conditions. Taking into account the lack of PK/PD relationship and need for sprinkling the odevixibat capsule contents on food for younger children, odevixibat can be administered with food.
Distribution
Odevixibat is more than 99% bound to human plasma proteins. The mean body weight adjusted apparent volumes of distribution (V/F) in paediatric patients for the 40 and 120 mcg/kg/day dose regimens are 40.3 and 43.7 L/kg, respectively.
Biotransformation
Odevixibat is minimally metabolised in humans.
Elimination
Following administration of a single oral dose of 3000 mcg of radiolabeled odevixibat in healthy adults, the average percent recovery of the administered dose was 82.9% in faeces; less than 0.002% was recovered in the urine. More than 97% of faecal radioactivity was determined to be unchanged odevixibat.
The mean body weight normalised apparent total clearances CL/F in paediatric patients for the 40 and 120 mcg/kg/day dose regimens are 26.4 and 23.0 L/kg/h, respectively, and the mean half-life is approximately 2.5 hours.
Linearity/non-linearity
The Cmax and AUC0-t increase with increasing doses in a dose-proportional manner; however due to the high interindividual variability of approximately 40%, it is not possible to estimate the dose proportionality accurately.
Pharmacokinetic/pharmacodynamic relationship(s)
Consistent with the mechanism and site of action of odevixibat in the gastrointestinal tract no relationship between systemic exposure and clinical effects is observed. Also, no dose-response relationship could be established for the investigated dose range 10-200 mcg/kg/day and the PD parameters C4 and FGF19.
Special populations
No clinically significant differences in the pharmacokinetics of odevixibat were observed based on age, sex or race.
Hepatic impairment
The majority of patients with PFIC presented with some degree of hepatic impairment because of the disease. Hepatic metabolism of odevixibat is not a major component of the elimination of odevixibat. Analysis of data from a placebo-controlled study in patients with PFIC Types 1 and 2 did not demonstrate a clinically important impact of mildly impaired hepatic function (Child Pugh A) on the pharmacokinetics of odevixibat. Although, body weight adjusted CL/F values were lower and body weight adjusted V/F values were larger in paediatric patients with PFIC with Child Pugh B compared to healthy subjects, the safety profile was comparable between the patient groups. Patients with severe hepatic impairment (Child-Pugh C) have not been studied.
Renal impairment
There are no clinical data in patients with renal impairment, but the impact of renal impairment is expected to be small due to low systemic exposure and odevixibat is not excreted in urine.
In vitro studies
In in vitro studies, odevixibat did not inhibit CYPs 1A2, 2B6, 2C8, 2C9, 2C19 or 2D6 at clinically relevant concentrations, but was shown to be an inhibitor of CYP3A4/5.
Odevixibat does not inhibit the transporters P-gp, breast cancer resistance protein (BCRP), organic anion transporter (OATP1B1, OATP1B3, OAT1, OAT3), organic cation transporter (OCT2), multidrug and toxin extrusion transporter (MATE1 or MATE2-K).
Odevixibat is not a BCRP substrate.
5.3. Preclinical safety data
Adverse reactions not observed in clinical trials, but seen in animals at exposure levels similar to clinical exposure levels and with possible relevance to clinical use were as follows:
Reproductive and developmental toxicity:
In pregnant New Zealand White rabbits, early delivery/abortion was observed in two rabbits receiving odevixibat during the period of foetal organogenesis at an exposure multiple of ≥2.3 of the anticipated clinical exposure (based on total plasma odevixibat AUC0-24). Reductions in maternal body weight and food consumption were noted in all dose groups (transient at the exposure multiple 1.1 of the anticipated dose).
Starting from the exposure multiple of 1.1 of the clinical human exposure (based on total plasma odevixibat AUC0-24), 7 foetuses (1.3% of all foetuses from odevixibat exposed does) in all dose groups were found to have cardiovascular defects (i.e. ventricular diverticulum, small ventricle and dilated aortic arch). No such malformations were observed when odevixibat was administered to pregnant rats. Because of the findings in rabbits, an effect of odevixibat on cardiovascular development cannot be excluded.
Odevixibat had no effect on the reproductive performance, fertility, embryo-foetal development, or prenatal/postnatal development studies in rats at the exposure multiple of 133 of the anticipated clinical exposure (based on total plasma odevixibat AUC0-24), including juveniles (exposure multiple of 63 of the anticipated human exposure).
There is insufficient information on the excretion of odevixibat in animal milk.
The presence of odevixibat in breast milk was not measured in animal studies. Exposure was demonstrated in the pups of lactating dams in the pre- and post-natal developmental toxicity study with rats (3.2-52.1% of the odevixibat plasma concentration of the lactating dams). It is therefore possible that odevixibat is present in breast milk.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.