CAMZYOS Hard capsule Ref.[51067] Active ingredients: Mavacamten
Source: European Medicines Agency (EU) Revision Year: 2023 Publisher: Bristol-Myers Squibb Pharma EEIG, Plaza 254, Blanchardstown Corporate Park 2, Dublin 15, D15 T867, Ireland
4.1. Therapeutic indications
CAMZYOS is indicated for the treatment of symptomatic (New York Heart Association, NYHA, class II-III) obstructive hypertrophic cardiomyopathy (oHCM) in adult patients (see section 5.1).
4.2. Posology and method of administration
Treatment should be initiated under the supervision of a physician experienced in the management of patients with cardiomyopathy.
Before treatment initiation, patients' left ventricular ejection fraction (LVEF) should be assessed by echocardiography (see section 4.4). If LVEF is <55%, treatment should not be initiated.
Before initiation of treatment, women of childbearing potential must have a negative pregnancy test (see section 4.4 and 4.6).
Patients should be genotyped for Cytochrome P450 (CYP) 2C19 (CYP2C19) in order to determine appropriate mavacamten dose. Patients with CYP2C19 poor metabolizer phenotype may have increased mavacamten exposures (up to 3 times) that can lead to increased risk of systolic dysfunction compared to normal metabolizers (see section 4.4 and 5.2). If treatment initiation occurs prior to determination of CYP2C19 phenotype, patients should follow dosing instructions for poor metabolisers (see figure 1 and table 1) until CYP2C19 phenotype is determined.
Posology
The dose range is 2.5 mg to 15 mg (either 2.5 mg, 5 mg, 10 mg or 15 mg). The bioequivalence between strengths has not been confirmed in a bioequivalence study in humans; therefore, the use of multiple capsules to achieve a prescribed dose is prohibited and one capsule of the appropriate dose strength should be used.
CYP2C19 poor metaboliser phenotype
The recommended starting dose is 2.5 mg orally once daily. The maximum dose is 5 mg once daily. The patient should be assessed for early clinical response by left ventricular outflow tract (LVOT) gradient with Valsalva manoeuvre 4 and 8 weeks after treatment initiation (see figure 1).
CYP2C19 intermediate, normal, rapid and ultra-rapid metaboliser phenotype
The recommended starting dose is 5 mg orally once daily. The maximum dose is 15 mg once daily. The patient should be assessed for early clinical response by LVOT gradient with Valsalva manoeuvre 4 and 8 weeks after treatment initiation (see figure 2). Once an individualised maintenance dose is achieved, patients should be assessed every 12 weeks (see figure 3). If at any visit the patient's LVEF is <50%, the treatment should be interrupted for 4 weeks and until LVEF returns to ≥50% (see figure 4).
In patients experiencing an intercurrent illness such as serious infection or arrhythmia (including atrial fibrillation or other uncontrolled tachyarrhythmia) which may impair systolic function, LVEF assessment is recommended, and dose increases are not recommended until intercurrent illness is resolved (see section 4.4).
Consideration should be given to discontinue treatment in patients who have shown no response (e.g., no improvement in symptoms, quality of life, exercise capacity, LVOT gradient) after 4-6 months on the maximum tolerated dose.
Figure 1. Treatment initiation in CYP2C19 poor metaboliser phenotype:
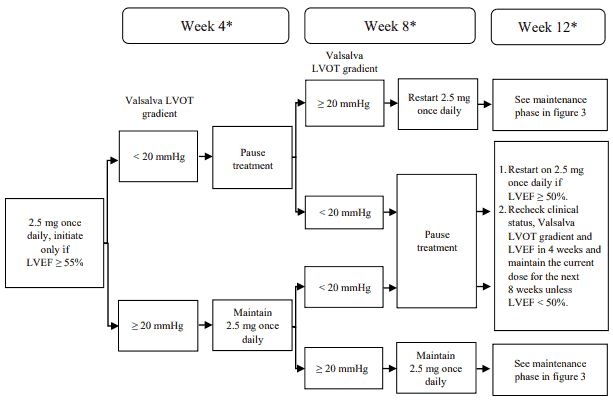
* Interrupt treatment if LVEF is <50% at any clinical visit; restart treatment after 4 weeks if
LVEF ≥50% (see figure 4).
LVEF = left ventricular ejection fraction; LVOT = left ventricular outflow tract
Figure 2. Treatment initiation in CYP2C19 intermediate, normal, rapid and ultra-rapid metaboliser phenotype:
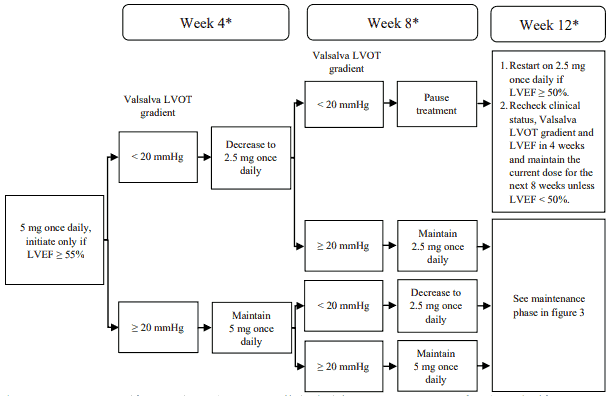
* Interrupt treatment if LVEF is <50% at any clinical visit; restart treatment after 4 weeks if
LVEF ≥50% (see figure 4).
LVEF = left ventricular ejection fraction; LVOT = left ventricular outflow tract
Figure 3. Maintenance phase:
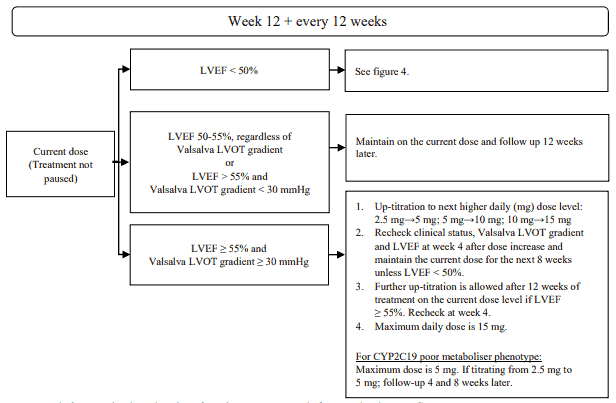
LVEF = left ventricular ejection fraction; LVOT = left ventricular outflow tract
Figure 4. Treatment interruption at any clinic visit if LVEF <50%:
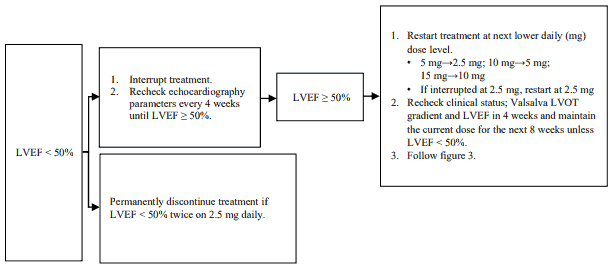
LVEF = left ventricular ejection fraction; LVOT = left ventricular outflow tract
Dose modification with concomitant medicinal products
For concomitant treatment with inhibitors and inducers of CYP2C19 or CYP3A4, follow the steps shown in table 1 (see also section 4.5).
Table 1. Dose modification of mavacamten with concomitant medicinal products:
| Concomitant medicinal product | CYP2C19 poor metaboliser phenotype* | CYP2C19 intermediate, normal, rapid and ultra-rapid phenotype |
|---|---|---|
| Inhibitors | ||
| Combined use of a strong CYP2C19 inhibitor and a strong CYP3A4 inhibitor | Contra-indicated (see section 4.3). | Contra-indicated (see section 4.3). |
| Strong CYP2C19 inhibitor | No dose adjustment (see section 4.5). If CYP2C19 phenotype has not yet been determined: No adjustment of the starting dose of 2.5 mg is needed. The dose should be reduced from 5 mg to 2.5 mg or pause treatment if on 2.5 mg (see section 4.5). | Initiate mavacamten at a dose of 2.5 mg. The dose should be reduced from 15 mg to 5 mg and from 10 mg and 5 mg to 2.5 mg or pause treatment if on 2.5 mg (see section 4.5). |
| Strong CYP3A4 inhibitor | Contra-indicated (see section 4.3). | No dose adjustment (see section 4.5). |
| Moderate CYP2C19 inhibitor | No dose adjustment. If CYP2C19 phenotype has not yet been determined: No adjustment of the starting dose of 2.5 mg is needed. The dose should be reduced from 5 mg to 2.5 mg or pause treatment if on 2.5 mg (see section 4.5). | No adjustment of the starting dose of 5 mg is needed. The dose should be reduced by one dose level or pause treatment if on 2.5 mg (see section 4.5). |
| Moderate or weak CYP3A4 inhibitor | No adjustment of the starting dose of 2.5 mg is needed. If patients are receiving a 5 mg dose of mavacamten, their dose should be reduced to 2.5 mg (see section 4.5). | No dose adjustment (see section 4.5). |
| Inducers | ||
| Discontinuing or decreasing the dose of strong CYP2C19 inducer and strong CYP3A4 inducer | The dose should be reduced from 5 mg to 2.5 mg or pause treatment if on 2.5 mg (see section 4.5). | The dose should be reduced by one dose level when on doses 5 mg or higher when discontinuing or decreasing the dose of strong inducers while on mavacamten (see section 4.5). No dose adjustment when on 2.5 mg. |
| Discontinuing or decreasing the dose of moderate or weak CYP3A4 inducer | Decrease mavacamten dose to 2.5 mg or pause treatment if on 2.5 mg (see section 4.5). | No dose adjustment (see section 4.5). |
* includes patients for whom the CYP2C19 phenotype has not yet been determined.
Missed or delayed doses
If a dose is missed, it should be taken as soon as possible, and the next scheduled dose should be taken at the usual time the following day. Two doses should not be taken on the same day.
Special populations
Elderly
No dose adjustment to the standard dose and titration scheme is required for patients aged 65 years and older (see section 5.2).
Renal impairment
No dose adjustment to the standard dose and titration scheme is required for patients with mild (estimated glomerular filtration rate [eGFR] 60-89 mL/min/1.73m²) to moderate (eGFR 30-59 mL/min/1.73m²) renal impairment. No dose recommendation can be made for patients with severe (eGFR <30 mL/min/1.73m²) renal impairment because mavacamten has not been studied in patients with severe renal impairment (see section 5.2).
Hepatic impairment
The mavacamten starting dose should be 2.5 mg in all patients with mild (Child-Pugh class A) and moderate (Child-Pugh class B) hepatic impairment since mavacamten exposure is likely to be increased (see section 5.2). No dose recommendation can be made for patients with severe hepatic impairment (Child-Pugh class C) because mavacamten has not been studied in patients with severe hepatic impairment (see section 4.4 and 5.2).
Paediatric population
The safety and efficacy of mavacamten in children and adolescents below 18 years have not been established. No data are available. Mavacamten should not be used in children less than 12 years because of potential safety concerns.
Method of administration
For oral use.
Treatment should be taken once daily with or without meals at about the same time each day. Use a single capsule for a prescribed dose. The capsule should be swallowed whole with water.
4.9. Overdose
Human experience of overdose with mavacamten is limited. Mavacamten has been given as a single dose of up to 144 mg in patients with HCM. There was one serious adverse reaction of vasovagal reaction, hypotension, and asystole lasting 38 seconds reported at that dose. In healthy subjects, doses of up to 25 mg have been administered for up to 25 days. A reduction of LVEF by 20% or greater was experienced in 3 out of 8 participants treated at the 25 mg dose level. Systolic dysfunction is the most likely result of overdose of mavacamten. If warranted, treatment of overdose with mavacamten consists of discontinuation of mavacamten treatment as well as medically supportive measures to maintain hemodynamic status (e.g. initiation of inotropic support with adrenergic agents), including close monitoring of vital signs and LVEF and management of the clinical status of the patient. Early administration of activated charcoal may be considered in case of mavacamten overdose to reduce absorption. This recommendation is based on standard treatment of medicinal product overdose, as the use of activated charcoal to reduce absorption of mavacamten has not been specifically studied.
6.3. Shelf life
3 years.
6.4. Special precautions for storage
This medicinal product does not require any special storage conditions.
6.5. Nature and contents of container
Polyvinylchloride (PVC) / Polychlorotrifluoroethylene (PCTFE) / Aluminium foil blister containing 14 hard capsules.
Pack size of 14 or 28 hard capsules.
Not all pack sizes may be marketed.
6.6. Special precautions for disposal and other handling
Any unused medicinal product or waste material should be disposed of in accordance with local requirements.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.