COMETRIQ Hard capsule Ref.[116727] Active ingredients: Cabozantinib
Source: European Medicines Agency (EU) Revision Year: 2026 Publisher: Ipsen Pharma, 70 rue Balard, 75015 Paris, France
5.1. Pharmacodynamic properties
Pharmacotherapeutic group: antineoplastic agent, protein kinase inhibitor
ATC code: L01EX07
Mechanism of action
Cabozantinib is a small molecule that inhibits multiple receptor tyrosine kinases (RTKs) implicated in tumour growth and angiogenesis, pathologic bone remodelling, and metastatic progression of cancer. Cabozantinib was evaluated for its inhibitory activity against a variety of kinases and was identified as an inhibitor of MET (hepatocyte growth factor receptor protein) and VEGF (vascular endothelial growth factor) receptors. In addition, cabozantinib inhibits other tyrosine kinases including RET, the GAS6 receptor (AXL), the stem cell factor receptor (KIT), and Fms-like tyrosine kinase-3 (FLT3).
Pharmacodynamic effects
Cabozantinib exhibited dose-related tumour growth inhibition, tumour regression, and/or inhibited metastasis in a broad range of preclinical tumour models.
Efficacy with cabozantinib was observed in medullary thyroid cancer patients with wild-type or mutant RET.
Clinical data in medullary thyroid cancer
A multi-center, randomised double-blind study comparing cabozantinib (N=219) with placebo (N=111) was conducted in patients with unresectable locally advanced or metastatic MTC and documented radiographic disease progression within 14 months prior to study entry. The primary objective was to compare progression-free survival (PFS) in patients receiving cabozantinib versus patients receiving placebo. The secondary objectives were to compare overall response rate (ORR) and overall survival (OS). Centralized, independent, blinded review of the imaging data was used in the assessment of PFS and ORR. Patients were treated until disease progression or unacceptable toxicity.
The result of the PFS analysis, based on the central review RECIST assessment, demonstrated a statistically significant difference in the duration of PFS with cabozantinib versus placebo: the median duration was 11.2 months for subjects in the cabozantinib arm versus 4.0 months for subjects in the placebo arm (stratified Hazard Ratio [HR] = 0.28; 95% CI: 0.19, 0.40; p<0.0001; Figure 1). The PFS results were consistent across all baseline and demographic subgroups evaluated, including prior therapy with tyrosine kinase inhibitors (which may have consisted of agents targeting pathways associated with anti-angiogenesis), RET mutational status (including subjects documented not to have RET mutations), prior anticancer or radiotherapy status, or the existence of bone metastases.
The ORR was 27.9% and 0% for subjects in the cabozantinib arm and placebo arm, respectively (p<0.0001; Table 2). The median duration of objective responses was 14.6 months (95% CI: 11.1, 17.5) for subjects in the cabozantinib arm.
Figure 1. Kaplan Meier curve of progression free survival:
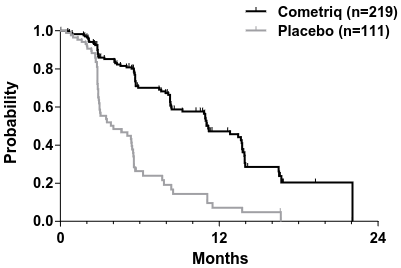
| Number of subjects at risk | ||||||||
| Month | 0 | 3 | 6 | 9 | 12 | 15 | 18 | 21 |
| Cometriq | 219 | 121 | 78 | 55 | 31 | 12 | 2 | 1 |
| Placebo | 111 | 35 | 11 | 6 | 3 | 2 | 0 | 0 |
The final analysis of OS was conducted after 218 events (deaths) occurred and shows a trend for an increase in median survival of 5.5 months in the cabozantinib arm: median (months) 26.6 cabozantinib vs. 21.1 placebo (HR = 0.85 [95% CI: 0.64, 1.12], p = 0.2409).
Figure 2. Kaplan-Meier curve of overall survival:
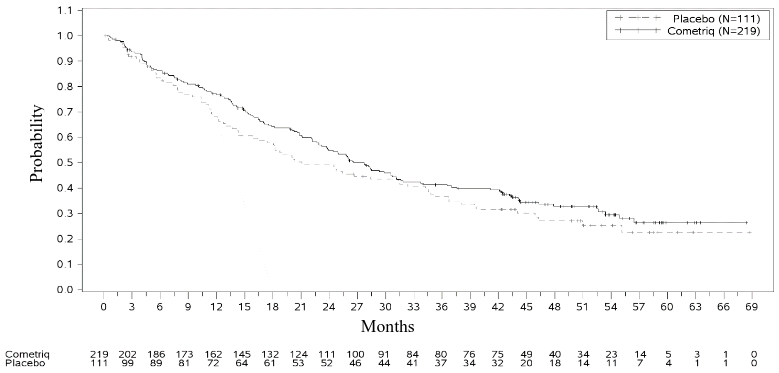
Table 2. Summary of key efficacy findings:
| Cabozantinib | Placebo | |
| Median progression-free survival | 11.2 months | 4.0 months |
| HR: 0.28 (0.19, 0.40) p<0.0001 | ||
| Median overall survival | 26.6 months | 21.1 months |
| HR: 0.85 (0.64, 1.12) p=0.2409 | ||
| Overall response ratea (95% CI) | 27.9% (21.9%, 34.5%) | 0% |
| p<0.0001 | ||
| Duration of response; median (95% CI) | 14.6 months (11.1, 17.5) | N/A |
| Disease control rateb (95% CI) | 55.3% (48.3%, 62.2%) | 13.5% (7.6%, 21.6%) |
| Calcitonin responsea | 47% (49/104)c | 3% (1/40)c |
| CEA responsea | 33% (47/143)c | 2% (1/55)c |
a Response = CR + PR
b Disease control rate = SD + ORR
c Includes patients who were evaluable for response
RET mutation status
Of the 215 subjects with sufficient data to determine mutational status, 78.6% (n=169) were classified as RET mutation positive (126 of which were positive for the M918T mutation), and 21.4% (n=46) were classified as RET mutation negative. For an additional 115 subjects the RET mutational status could not be determined or was unclear. All three subgroups showed increased PFS in the cabozantinib arm compared to the placebo arm (HRs of 0.23, 0.53, and 0.30 for RET mutation positive, negative, and unknown subgroups, respectively). The objective response rates measured in these subgroups were generally consistent with the PFS results, with the RET mutation positive, negative, and unknown subgroups showing tumour response rates of 32%, 22%, and 25%, respectively.
Further genetic analysis showed that a small proportion of patients harboured somatic tumour mutations in HRAS, KRAS, or NRAS. These patients (n=16) showed significant prolongation of PFS (HR of 0.15) and an objective response rate of 31%. RET mutation negative patients with no evidence of RAS mutation (n=33) showed a decreased PFS benefit on cabozantinib (HR of 0.87) and a lower response rate of 18% compared to other mutational subgroups.
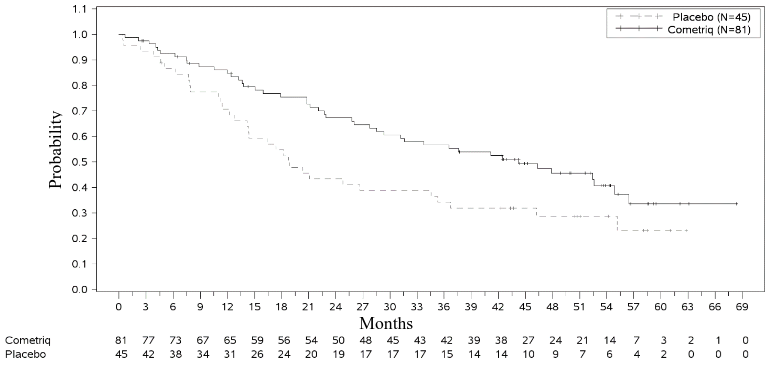
A significant improvement in OS was observed in the subgroup of RET M918T mutation positive patients (n=81/219 cabozantinib arm): 44.3 months in the cabozantinib arm vs. 18.9 months in the placebo arm (HR=0.60, p=0.0255). There was no improvement in OS for the RET M918T negative and unknown subgroups.
Figure 3. Kaplan-Meier analysis of OS among subjects with a RET M918T mutation:
Paediatric population
The European Medicines Agency has deferred the obligation to submit the results of studies with cabozantinib in one or more subsets of the paediatric population in the treatment of malignant solid tumours (see section 4.2 for information on paediatric use).
5.2. Pharmacokinetic properties
Absorption
Following oral administration of cabozantinib, peak cabozantinib plasma concentrations are reached at 2 to 5 hours post-dose. Plasma-concentration time profiles show a second absorption peak approximately 24 hours after administration, which suggests that cabozantinib may undergo enterohepatic recirculation.
Repeat daily dosing of cabozantinib at 140 mg for 19 days resulted in an approximately a 4- to 5-fold mean cabozantinib accumulation (based on AUC) compared to a single dose administration; steady state is achieved by approximately Day 15.
A high-fat meal moderately increased Cmax and AUC values (41% and 57%, respectively) relative to fasted conditions in healthy volunteers administered a single 140 mg oral cabozantinib dose. There is no information on the precise food-effect when taken 1 hour after administration of cabozantinib.
Bioequivalence could not be demonstrated between the cabozantinib capsule and tablet formulations following a single 140 mg dose in healthy subjects. A 19% increase in the Cmax of the tablet formulation (CABOMETYX) compared to the capsule formulation (COMETRIQ) was observed. AUC were similar between cabozantinib tablet (CABOMETYX) and capsule (COMETRIQ) formulations (<10% difference).
Distribution
Cabozantinib is highly protein bound in vitro in human plasma (≥99.7%). Based on the population-pharmacokinetic (PK) model, the volume of distribution (V/F) is approximately 349 L (SE: ± 2.73%). Protein binding was not altered in subjects with mild or moderately impaired renal or hepatic function.
Biotransformation
Cabozantinib was metabolized in vivo. Four metabolites were present in plasma at exposures (AUC) greater than 10% of parent: XL184-N-oxide, XL184 amide cleavage product, XL184 monohydroxy sulfate, and 6-desmethyl amide cleavage product sulfate. Two non-conjugated metabolites (XL184-N-oxide and XL184 amide cleavage product), which possess <1% of the on-target kinase inhibition potency of parent cabozantinib, each represent <10% of total drug-related plasma exposure.
Cabozantinib is a substrate for CYP3A4 metabolism in vitro, as a neutralizing antibody to CYP3A4 inhibited formation of metabolite XL184 N-oxide by >80% in a NADPH-catalyzed human liver microsomal (HLM) incubation; in contrast, neutralizing antibodies to CYP1A2, CYP2A6, CYP2B6, CYP2C8, CYP2C19, CYP2D6 and CYP2E1 had no effect on cabozantinib metabolite formation. A neutralizing antibody to CYP2C9 showed a minimal effect on cabozantinib metabolite formation (ie, a <20% reduction).
Elimination
The plasma terminal half-life of cabozantinib in single dose studies in healthy volunteers is approximately 120 hours. Mean clearance (CL/F) at steady-state in cancer patients was estimated to be 4.4 L/hr in a population PK analysis. Within a 48-day collection period after a single dose of 14C-cabozantinib in healthy volunteers, approximately 81% of the total administered radioactivity was recovered with 54% in faeces and 27% in urine.
Pharmacokinetics in special patient populations
Renal impairment
Results from a study in patients with renal impairment indicate that the ratios of geometric LS mean for plasma cabozantinib, Cmax and AUC0-inf were 19% and 30% higher, for subjects with mild renal impairment (90% CI for Cmax 91.60% to 155.51%; AUC0-inf 98.79% to 171.26%) and 2% and 6-7% higher (90% CI for Cmax 78.64% to 133.52%; AUC0-inf 79.61% to 140.11%), for subjects with moderate renal impairment, compared to subjects with normal renal function. Patients with severe renal impairment have not been studied.
Hepatic impairment
Results from a study in patients with hepatic impairment indicate that exposure (AUC0-inf) increased by 81% and 63% in subjects with mild and moderate hepatic impairment, respectively (90% CI for AUC0-inf: 121.44% to 270.34% for mild and 107.37% to 246.67% for moderate). Patients with severe hepatic impairment have not been studied.
Race
No data are available to determine a difference in PK based on race.
5.3. Preclinical safety data
Adverse reactions not observed in clinical studies, but seen in animals at exposure levels similar to clinical exposure levels and with possible relevance to clinical use were as follows: in rat and dog repeat-dose toxicity studies up to 6 months duration, target organs for toxicity were GI tract, bone marrow, lymphoid tissues, kidney, adrenal and reproductive tract tissues. The no observed adverse effect level (NOAEL) for these findings were below human clinical exposure levels at intended therapeutic dose.
Cabozantinib has shown no mutagenic or clastogenic potential in a standard battery of genotoxicity assays. The carcinogenic potential of cabozantinib has been evaluated in two species: rasH2 transgenic mice and Sprague-Dawley rats. In the 2-year rat carcinogenicity study, cabozantinib-related neoplastic findings consisted of an increased incidence of benign pheochromocytoma, alone or in combination with malignant pheochromocytoma/complex malignant pheochromocytoma of the adrenal medulla in both sexes at exposures well below the intended exposure in humans. The clinical relevance of the observed neoplastic lesions in rats is uncertain, but likely to be low. Cabozantinib was not carcinogenic in the rasH2 mouse model at a slightly higher exposure than the intended human therapeutic exposure.
Fertility studies in rats have shown reduced male and female fertility. Further, hypospermatogenesis was observe in male dogs at exposure levels below human clinical exposure levels at intended therapeutic dose.
Embryo-foetal development studies were performed in rats and rabbits. In rats, cabozantinib caused postimplantation loss, foetal oedema, cleft palate/lip, dermal aplasia and kinked or rudimentary tail. In rabbits, cabozantinib produced foetal soft tissue changes (reduced spleen size, small or missing intermediate lung lobe) and increased foetal incidence of total malformations. NOAEL for embryo-foetal toxicity and teratogenic findings were below human clinical exposure levels at intended therapeutic dose.
Juvenile rats (comparable to a >2 year old pediatric population) administered cabozantinib showed increased WBC parameters, decreased haematopoiesis, pubescent/immature female reproductive system (without delayed vaginal opening), tooth abnormalities, reduced bone mineral content and density, liver pigmentation and bile duct hyperplasia. Findings in uterus/ovaries and decreased haematopoiesis appeared to be transient, while effects on bone parameters and liver pigmentation were sustained. Evaluations in juvenile rats (comparable to a <2 year old pediatric population) have not been performed.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.