DAWNZERA Solution for injection Ref.[116065] Active ingredients: Donidalorsen
Source: FDA, National Drug Code (US) Revision Year: 2025
12.1. Mechanism of Action
Donidalorsen is an ASO‑GalNAc conjugate that causes ribonuclease H1 (RNase H1)‑mediated degradation of PKK mRNA through binding to PKK mRNA, which results in reduced production of PKK protein. PKK is a pro‑enzyme for plasma kallikrein, which results in the release of bradykinin, a potent vasodilator causing swelling and pain in HAE. In patients with HAE, C1‑inhibitor (C1‑INH) deficiency or dysfunction leads to excessive plasma kallikrein activity, bradykinin generation, and angioedema attacks. Donidalorsen lowers PKK concentration, preventing excessive bradykinin production in patients with HAE.
12.2. Pharmacodynamics
In OASIS-HAE in adult and pediatric patients (≥12 years) with HAE‑1 or HAE‑2 [see Clinical Studies (14)], a decrease in plasma PKK concentrations was observed at the first assessment (Week 4) following treatment with DAWNZERA 80 mg. The mean percentage reduction from baseline at Week 4 across both treatment groups was 48%. The mean percentage change from baseline to Week 24 in trough plasma PKK concentrations indicated reductions of 73% and 47% following treatment with DAWNZERA 80 mg every 4 weeks and every 8 weeks, respectively, compared with a slight increase (2%) observed in the placebo group.
Cardiac Electrophysiology
At the maximum recommended dose of DAWNZERA 80 mg every 4 weeks, clinically significant QTc interval prolongation was not observed.
12.3. Pharmacokinetics
The pharmacokinetic properties of DAWNZERA were evaluated following subcutaneous administration of multiple doses every 4 weeks in healthy subjects and every 4 weeks or every 8 weeks in patients with HAE. The pharmacokinetics of DAWNZERA were similar between healthy subjects and patients with HAE.
Donidalorsen exposure (area under the plasma concentration‑time curve [AUC]) at steady state following subcutaneous administration in healthy subjects increased in a greater than dose‑proportional manner over the dose range of 0.25 times the maximum recommended dosage to 80 mg every 4 weeks.
Geometric Mean (Coefficient of Variation [CV%]) of steady‑state maximum plasma concentration (Cmax,ss), trough plasma concentration (Ctrough,ss), and area under the plasma concentration‑time curve over the dosing interval (AUCτ,ss) are presented in Table 2. No accumulation of donidalorsen Cmax and AUC was observed in plasma after repeated dosing every 4 weeks. However, a 2-fold increase of plasma donidalorsen Ctrough was observed following repeated dosing every 4 weeks.
Table 2. Summary of Geometric Mean (CV%) Steady-State Donidalorsen Pharmacokinetic Parameters Following Dosage of DAWNZERA 80 mg Every 4 Weeks or 80 mg Every 8 Weeks in Patients with HAE:
| Pharmacokinetic Parameters (Geometric Mean) | DAWNZERA | |
| 80 mg q4wks | 80 mg q8wks | |
| Cmax,ss(ng/mL) | 417 (81%) | 416 (78%) |
| Ctrough,ss(ng/mL) | 0.755 (63%) | 0.255 (73%) |
| AUCτ,ss(ng·h/mL) | 5240 (52%) | 5210 (52%) |
AUCτ,ss = area under the plasma concentration time curve over each dosing interval at steady state; Cmax,ss = maximum plasma concentration at steady state; Ctrough,ss = trough plasma concentration at steady state; q4wks = every 4 weeks; q8wks = every 8 weeks.
Absorption
Following subcutaneous administration, donidalorsen is absorbed with the median (range) time to maximum plasma concentration of approximately 2 (0.25, 8) hours post dose.
Distribution
Donidalorsen is expected to distribute primarily to the liver and kidney cortex after subcutaneous dosing. The apparent volume of distribution for the central (Vc/F) and peripheral (Vp/F) compartment were 69.8 L and 1840 L, respectively. Donidalorsen is highly bound to human plasma proteins (>98% bound) in vitro.
Elimination
The terminal plasma elimination half-life of donidalorsen in a typical patient with HAE is approximately 1 month. The half-life of the initial rapid clearance phase, reflecting tissue distribution, was approximately 5 hours.
Metabolism
The oligonucleotide moiety of donidalorsen is expected to be metabolized by endo‑ and exonucleases to short oligonucleotide fragments of varying sizes within the liver. Based on in vitro studies, donidalorsen is not a substrate of cytochrome P450 (CYP) enzymes.
The linker that covalently connects the ASO to the GalNAc residues is cleaved via hydrolysis and undergoes dephosphorylation and subsequent oxidative metabolism to form inactive metabolites, which are minimally released in circulation. The most abundant linker-related metabolite (M8) is a substrate of CYP3A4.
Excretion
The mean fraction of unchanged ASO eliminated in urine was less than 1% of the administered dose in healthy subjects within 24 hours post-dose. The renal route of elimination is minor for linker-related metabolites.
Specific Populations
No clinically meaningful differences in the pharmacokinetics or pharmacodynamics of donidalorsen were observed based on age (12 to 68 years), body weight (37 to 152 kg), sex, race (68% White, 24% Black, and 4% Asian), ethnicity, disease status (healthy subjects or subjects with HAE), mild renal impairment (eGFR ≥60 to <90 mL/min/1.73 m²), or mild hepatic impairment (defined using NCI-ODWG Criteria: total bilirubin ≤1 × ULN and AST >1 × ULN, or total bilirubin >1 to 1.5 × ULN and any AST).
Donidalorsen has not been studied in patients with moderate or severe renal impairment, end‑stage renal disease, or moderate or severe hepatic impairment.
Drug Interaction Studies
No clinical drug‑drug interaction studies have been performed with donidalorsen. In vitro studies show that donidalorsen is not a substrate or inhibitor of transporters, does not interact with highly plasma protein bound drugs, and is not an inhibitor/inducer of CYP enzymes. In vitro studies show that linker-related metabolite M8 is not an inhibitor or inducer of CYP enzymes. M8 is a substrate of transporters bile salt export pump (BSEP) and organic anion transporting polypeptide 1B3 (OATP1B3), and is an inhibitor of multidrug and toxin extrusion protein 1 (MATE1) transporter.
13.1. Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
In a 6-month carcinogenicity study in transgenic (Tg.rasH2) mice, subcutaneous administration of donidalorsen, up to the highest dose tested (20 mg/kg in males and 60 mg/kg in females) or a mouse-specific surrogate (10 mg/kg) once every 2 weeks did not result in an increase in malignant tumors.
Mutagenesis
Donidalorsen was negative for genotoxicity in the in vitro bacterial reverse mutation test and chromosomal aberration assay in Chinese hamster lung cells and in vivo mouse bone marrow micronucleus assay.
Fertility
Fertility and reproductive performance were unaffected by subcutaneous administration of donidalorsen (up to 10 mg/kg/week [2.5-times the MRHD on a BSA basis]) or a mouse‑specific surrogate (4 mg/kg/week) to male and female mice weekly, prior to and during mating, and continuing every other day in females throughout the periods of implantation and organogenesis.
14. Clinical Studies
The efficacy of DAWNZERA for prophylaxis to prevent attacks of hereditary angioedema (HAE) in adult and pediatric patients 12 years of age and older was evaluated in a 24‑week multicenter, randomized, double‑blind, placebo‑controlled trial (OASIS-HAE [ NCT05139810]).
The trial (OASIS-HAE) included 90 adult and pediatric patients 12 years of age and older with Type I and Type II HAE, who had at least 2 investigator‑confirmed attacks during the 8‑week run‑in period. Patients were randomized to receive DAWNZERA 80 mg once every 4 weeks (n=45), DAWNZERA 80 mg once every 8 weeks (n=23), or matching placebo (n=22). Patients were required to discontinue other prophylactic HAE medications, except androgens and tranexamic acid, prior to entering the trial; all patients were allowed to use rescue medications for treatment of breakthrough HAE attacks.
The demographics and baseline characteristics of OASIS-HAE trial are provided in Table 3.
Table 3. Demographics and Baseline Characteristics of Patients in the OASIS-HAE Trial:
| OASIS-HAE (N=90) | |
| Female, n (%) | 48 (53) |
| Race, n (%) | |
| Asian | 1 (1) |
| Black or African American | 2 (2) |
| White | 82 (91) |
| American Indian or Alaskan Native Asian | 3 (3) |
| Multiple | 1(1) |
| Other | 1(1) |
| Hispanic or Latino, n (%) | 6 (7) |
| Mean age, years (SD) | 37 (14) |
| ≤17 years, n (%) | 7 (8) |
| >17 years, n (%) | 83 (92) |
| C1-INH HAE Type 1, n (%) | 84 (93) |
| Prior HAE prophylaxis*, n (%) | 16 (18) |
| Baseline HAE attack rate**, n (%) | |
| ≤2 attacks/4 weeks | 28 (31) |
| 2 to 5 attacks/4 weeks | 48 (53) |
| ≥5 attacks/4 weeks | 14 (16) |
* Within 5 half-lives of screening (up to 10 weeks).
** Period from screening to first dose.
The primary endpoint for OASIS-HAE was the HAE attack rate (number of investigator-confirmed HAE attacks per 4 weeks) from Week 0 to Week 24. As shown in Table 4, DAWNZERA 80 mg administered subcutaneously every 4 or 8 weeks demonstrated statistically significant reductions in the HAE attack rate compared to placebo.
Table 4. HAE Attack Rate (Attacks/4 Weeks) at Week 24 in OASIS-HAE:
| DAWNZERA 80 mg q4wks (N=45) | DAWNZERA 80 mg q8wks (N=23) | Placebo (N=22) | |
| HAE Attack Rate per 4 Weeks from Week 0 to Week 24* | |||
| LS mean (95% CI) attack rate | 0.44 (0.27, 0.73) | 1.02 (0.65, 1.59) | 2.26 (1.66, 3.09) |
| % Reduction (95% CI) relative to placebo† | -81 (-89, -65) | -55 (-74, -22) | -- |
| Wald chi-square p-value | <0.001 | 0.004 | -- |
CI = confidence interval; HAE = hereditary angioedema; LS = least square; N = number of patients in the specific treatment group; q4wks = every 4 weeks; q8wks = every 8 weeks.
* Primary efficacy endpoint = comparison of the time-normalized number of investigator-confirmed HAE attacks per 4 weeks from Week 0 to Week 24 between the DAWNZERA 80 mg q4wks group and the placebo group.
† Calculated as the ratio of the model-based treatment period HAE attack rates (donidalorsen/placebo) minus 1 multiplied by 100.
The mean decreases from baseline in the HAE attack rate observed throughout the treatment period in the DAWNZERA treatment groups are shown in Figure 1.
Figure 1. Mean (± SEM) Investigator‑confirmed HAE Attack Rate (Attacks/4 Weeks) in OASIS-HAE:
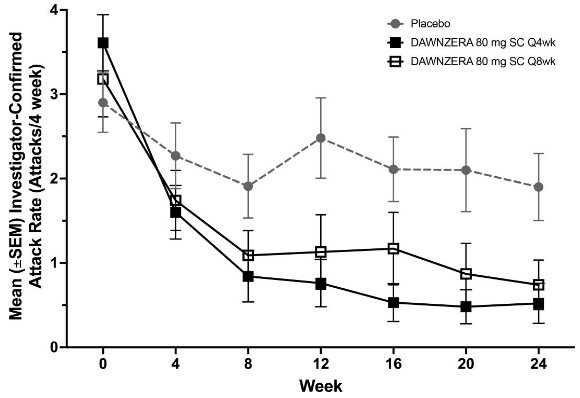
HAE = hereditary angioedema; q4wks = every 4 weeks; q8wks = every 8 weeks; SC = subcutaneous; SEM = standard error of the mean.
Pre-defined secondary endpoints were assessed from Week 4 to Week 24. The moderate or severe HAE attack rate was 0.12 for the DAWNZERA 80 mg every 4 weeks group, 0.68 for the DAWNZERA 80 mg every 8 weeks group, and 1.15 for the placebo group, representing a reduction of 89% (95% CI: 66, 97) and 41% (95% CI: -26, 72) in moderate or severe HAE attack rate relative to placebo, respectively. The HAE attacks requiring acute therapy was 0.15 for the DAWNZERA 80 mg every 4 weeks group, 0.59 for the DAWNZERA 80 mg every 8 weeks group, and 1.80 for the placebo group, representing a reduction of 92% (95% CI: 77, 97) and 67% (95% CI: 29, 85) in HAE attacks requiring acute therapy relative to placebo, respectively.
The proportion of patients who were attack-free from Week 4 to Week 24 were 53% in the DAWNZERA 80 mg every 4 weeks group, 35% in the DAWNZERA 80 mg every 8 weeks group, and 9% in the placebo group, representing an odds ratio of being attack-free of 11.79 (95% CI: 2.34, 59.36) and 3.23 (95% CI: 0.46, 22.85), respectively.
The proportion of patients with a ≥50%, ≥70%, and ≥90% reduction from baseline to Week 4 through Week 24 was 93%, 82%, and 62% in the DAWNZERA 80 mg every 4 weeks group, 83%, 65%, and 48% in the DAWNZERA 80 mg every 8 weeks group, and 27%, 18%, and 9% in the placebo group, respectively.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.