DECAPEPTYL SR Powder for suspension for injection Ref.[8222] Active ingredients: Triptorelin
Source: Medicines & Healthcare Products Regulatory Agency (GB) Revision Year: 2017 Publisher: Ipsen Limited, 190 Bath Road, Slough, Berkshire, SL1 3XE, United Kingdom
Pharmacodynamic properties
Pharmacotherapeutic group: Gonadotropin-Releasing Hormone analogue
L02AE04: Antineoplastic and immunomodulator
Triptorelin is a decapeptide analogue of GnRH which initially stimulates release of pituitary gonadotropins.
Patients with prostate cancer
This results in an increase in peripheral circulating levels of testosterone and dihydrotestosterone. Continued administration (over 7 days) however, leads to suppression of gonadotropins and a consequent fall in plasma testosterone. In patients with prostate cancer, plasma testosterone levels fall to castrate levels after 2-3 weeks of treatment, frequently resulting in an improvement of function and objective symptoms.
The efficacy and safety of triptorelin has been determined in clinical studies involving 645 patients with locally advanced or metastatic prostate cancer.
Of these, three long term controlled studies compared the efficacy and safety of triptorelin to bilateral orchidectomy as an initial therapy in patients with locally advanced or metastatic prostate cancer (stage C or D). In one of these three long term studies, 7 patients in the triptorelin group and 7 patients in the orchidectomy group had also undergone prostatectomy. Triptorelin induced biochemical castration at least as rapidly as surgical pulpectomy and was as effective as surgical castration in the long term palliative treatment of locally advanced or metastatic prostate cancer. Both the triptorelin and orchidectomy groups showed improvements in dysuria and pain, and reduction in volume of prostate. Analysis after six and eight years in two of the studies showed that there was no significant difference in the median survival rates in the triptorelin group versus the orchidectomy group.
A study assessing the pharmacodynamic equivalence between triptorelin 3-month and 28-day prolonged release formulations in patients with locally advanced or metastatic prostate cancer, found that equivalent testosterone suppression was achieved, whether 3 doses of Decapeptyl SR 3 mg (n=68) or a single dose of Decapeptyl SR 11.25 mg (n=63) was given. The percentage of patients who achieved a testosterone castrate level ≤ 0.5 ng/mL at D84 was similar in the two treatment groups (98% and 96% in the 3-month and 28-day formulation groups, respectively). The time to achieve chemical castration was not significantly different between the two groups.
In a phase III randomized clinical trial including 970 patients with locally advanced prostate cancer (mainly T2c-T4 with some T1c to T2b patients with pathological regional nodal disease) of whom 483 were assigned to short-term androgen suppression (6 months) in combination with radiation therapy and 487 to long-term therapy (3 years), a non-inferiority analysis compared the short-term to long-term concomitant and adjuvant hormonal treatment with triptorelin (62.2%) or goserelin (30.1%). The 5-year overall mortality was 19.0% and 15.2%, in the short-term and long-term groups, respectively. The observed Hazard Ratio of 1.42 with an upper one-sided 95.71% CI of 1.79 or two-sided 95.71% CI of 1.09; 1.85 (p = 0.65 for non inferiority), demonstrate that the combination of radiotherapy plus 6 months of androgen deprivation therapy provides inferior survival as compared with radiotherapy plus 3 years of androgen deprivation therapy. Overall survival at 5 years of long-term treatment and short-term treatment shows 84.8% survival and 81.0%, respectively.
Overall quality of life using QLQ-C30 did not differ significantly between the two groups (P= 0.37).
Neoadjuvant triptorelin prior to radiotherapy has been shown to significantly reduce prostate volume.
The use of a GnRH agonist may be considered after radical prostatectomy in selected patients considered at high risk of disease progression. There are no disease-free survival data or survival data with triptorelin in this setting.
Patients with endometriosis and uterine fibroids
Continued administration of Decapeptyl SR 3 mg induces suppression of oestrogen secretion and thus enables resting of ectopic endometrial tissue. In pre-operative therapy for uterine fibroids there appears to be a beneficial effect on the blood loss at surgery. Studies have demonstrated a consistent and marked reduction in uterine and/or fibroid volume becoming maximal in a three to six month treatment period. Clinical studies have shown that 90-100% of patients with fibroids become amenorrhoeic within two months of treatment and triptorelin provides relief from the symptoms of abdominal pain, dysmenorrhoea and menorrhagia associated with uterine fibroids.
Breast cancer
Clinical studies performed in premenopausal women with endocrine responsive early stage breast cancer have been conducted with triptorelin in order to suppress oestradiol ovarian secretion, the main source of oestrogens. Based on studies performed in healthy women and women with endometriosis, the effect of triptorelin is achieved 3-4 weeks after administration.
Two phase 3 studies (SOFT and TEXT) have explored the 5-year benefit of ovarian function suppression (OFS) in combination with tamoxifen (T) or an aromatase inhibitor (exemestane-E) in premenopausal women with endocrine responsive early stage breast cancer.
Triptorelin was the main treatment used to achieve OFS (91.0% of randomised subjects in the SOFT study, and 100% in the TEXT study). The remaining 9% of women in the SOFT study had bilateral oophorectomy or bilateral ovarian irradiation.
SOFT study results
The SOFT study was designed to answer the question of the added value of OFS to tamoxifen as adjuvant treatment of premenopausal women with endocrine responsive early stage breast cancer.
A total of 3047 women were analysed (1015 women in the T+OFS, 1018 women in the T alone and 1014 women in the E+OFS arm).
At a median follow-up of 67 months (5.6 years), treatment with T+OFS non-significantly reduced the hazard of a Disease Free Survival (DFS) event versus T alone (HR=0.83; 95% CI, 0.66 to 1.04; p=0.10). The estimated 5-year DFS was 86.6% (95% CI, 84.2% to 88.7%) among women assigned to T+OFS compared with 84.7% (95% CI, 82.2% to 86.9%) for women assigned to T alone.
However, after adjustment for prespecified covariates in the multivariate Cox model, women assigned treatment with T+OFS had a significantly reduced hazard of a DFS event compared with women assigned T alone, with a reduction of 22% (HR=0.78; 95% CI, 0.62 to 0.98; p=0.03).
Women assigned treatment with T+OFS had a non-significantly reduced hazard of a breast cancer event compared with women assigned T alone (HR=0.81; 95% CI, 0.63 to 1.03; p=0.09). The estimated 5-year Breast Cancer Free Interval (BCFI) was 88.4% (95% CI, 86.1% to 90.3%) for women assigned treatment with T+OFS compared with 86.4% (95% CI, 84.0% to 88.5%) for women assigned T alone.
However, after adjusting for pre-specified covariates in the multivariable Cox model, women assigned T+OFS had a significantly reduced hazard of a BCFI event compared with women assigned T with a reduction of 25% (HR=0.75; 95% CI, 0.59 to 0.96; p=0.02).
The absolute benefit is higher in women who received adjuvant chemotherapy. The DFS rate at 5 years for women who received adjuvant chemotherapy was 80.7% in the T + OFS arm and 77.1% in the T arm only (HR=0.82; 95% CI, 0.64 to 1.07) with an absolute benefit of 3.6% for T+OFS.
In particular, the benefit of adding OFS was apparent for 5-year DFS in a post-hoc analysis for the subgroup of women less than 40 years old (HR=0.74; 95% CI, 0.53, 1.03) with an absolute benefit of 4.4% for T+OFS compared to T alone.
In the SOFT study, subjects assigned E+OFS had a statistically significantly reduced hazard of a DFS event, as compared with subjects assigned T alone (HR=0.68, 95% CI, 0.53 to 0.86). The estimated 5-year DFS rate was 89.0% (95% CI, 86.8% to 90.9%) among subjects assigned to E+OFS as compared with 84.7% (95% CI, 82.2% to 86.9%) among subjects assigned T alone.
Subjects assigned E+OFS had a statistically significantly reduced hazard of a breast cancer event as compared with subjects assigned T alone (HR=0.64; 95% CI, 0.49 to 0.83). The estimated 5-year BCFI was 90.9% (95% CI, 88.9% to 92.6%) among subjects assigned E+OFS compared with 86.4% (95% CI, 84.0% to 88.5%) among subjects assigned T alone.
Subjects assigned E+OFS had a statistically significantly reduced hazard of a distant recurrence as compared with subjects assigned T alone (HR=0.71; 95% CI, 0.52 to 0.96). The estimated 5-year Distant Recurrence Free Interval (DRFI) was 93.0% (95% CI, 91.2% to 94.5%) among subjects assigned E+OFS compared with 90.7% (95% CI, 88.6% to 92.4%).
The absolute benefit is higher in women who received adjuvant chemotherapy. The DFS rate at 5 years for women who received adjuvant chemotherapy was 83.8% in the E + OFS arm and 77.1% in the T arm only (HR=0.70, 95%CI, 0.53 to 0.92) with an absolute benefit of 6.7% for E+OFS.
Kaplan-Meier Estimates of DFS in women who received prior chemotherapy
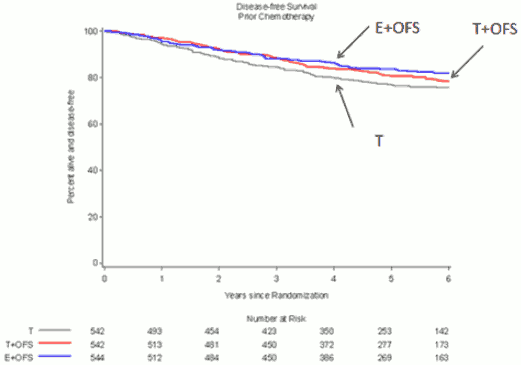
In the 3 arms SOFT study, women who received chemotherapy had a higher proportion of high risk clinical criteria of recurrence: 49.3% below age < 40, 56.9% with lymph nodes positive, 47.0% with breast tumour size > 2 cm and 33.7% with tumour grade 3.
Combined SOFT and TEXT study results
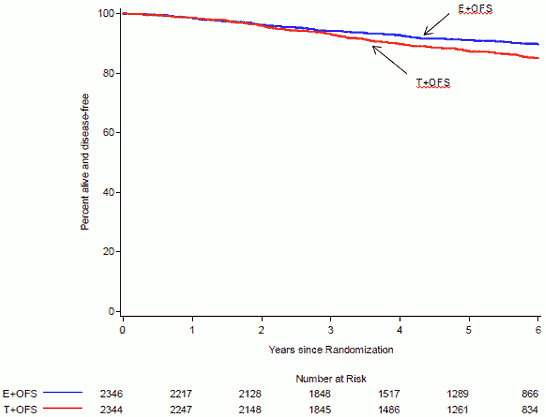
The primary objective of TEXT study was to evaluate the role of aromatase inhibitors (exemestane) in women treated with OFS compared with T+OFS including all women from SOFT and TEXT studies. A total of 4690 women were analysed: 2346 women in the E+OFS arm and 2344 women in the T+OFS arm.
At a median follow-up of 68 months (5.7 years), treatment with E+OFS statistically significantly reduced the hazard of a DFS event versus T+OFS (HR=0.72; 95% CI, 0. 60 to 0.86; p=0.0002). The estimated 5-year DFS was 91.1% (95% CI, 89.7% to 92.3%) for women assigned to E+OFS compared with 87.3% (95% CI, 85.7% to 88.7%) for women assigned T+OFS.
Kaplan-Meier Estimates of DFS OFS+E vs OFS+T
Women assigned E+OFS had a statistically significantly reduced hazard of a breast cancer event compared with women assigned T+OFS (HR=0.66; 95% CI, 0.55 to 0.80; P<0.0001). The estimated 5-year BCFI was improved at 92.8% (95% CI, 91.6% to 93.9%) for women assigned E+OFS compared with 88.8% (95% CI, 87.3% to 90.1%) for women assigned T+OFS.
Pharmacokinetic properties
SUBCUTANEOUS FORM
In healthy volunteers
Subcutaneously administered triptorelin (100 μg) is rapidly absorbed (Tmax = 0.63 ± 0.26 hr for peak plasma concentration = 1.85 ± 0.23 ng/mL). Elimination is effected with a biological half-life of 7.6 ± 1.6 hr, after a 3 to 4 hr distribution phase. Total plasma clearance is: 161 ± 28 mL/min. Distribution volume is 104.1 ± 11.7 litres.
In patients with prostate cancer
With subcutaneous administration (100 μg), triptorelin blood levels oscillate between maximum values of 1.28 ± 0.24 ng/mL (Cmax) obtained in general one hour after injection (Tmax) and minimum values of 0.28 ± 0.15 ng/mL (Cmax) obtained 24hrs after injection.
The biological half-life is on average 11.7 ± 3.4 hr but varies according to patients. Plasma clearance (118 ± 32 mL/min) reflects slower elimination in patients, whilst distribution volumes are close to those of healthy volunteers (113.4 ± 21.6 litres).
SUSTAINED RELEASE FORM
In patients with prostate cancer
Following intramuscular injection of the sustained release form, an initial phase of release of the active principle present on the surface of the microspheres is observed, followed by further fairly regular release (Cmax = 0.32 ± 0.12 ng/mL), with a mean rate of release of triptorelin of 46.6 ± 7.1 μg/day. The bioavailability of the microparticles is approximately 53% at one month.
In patients with endometriosis and uterine fibroids
After intramuscular injection of Decapeptyl SR 3 mg in women with endometriosis and uterine fibroids the maximum blood level of triptorelin is obtained between 2 to 6 hours after injection, the peak value reached is 11 ng/mL. There was no evidence of accumulation of the product following monthly injections over six months.
The minimum blood level oscillates between 0.1 and 0.2 ng/mL. The bioavailability of the sustained release product is approximately 50%.
Trough plasma concentrations are maintained between 0.1 and 0.2 ng/mL. The bioavailability of the sustained release product is approximately 50%. These data observed in endometriosis and uterine fibroma patients can be extrapolated to breast cancer patients as it is not expected that the disease has an impact on the prolonged release properties of the product.
Preclinical safety data
Preclinical findings were only those related to the expected pharmacological activity of triptorelin, namely down-regulation of the hypothalamic-pituitary-gonadal axis. These included atrophy of the testes and genital tract, with resultant suppression of spermatogenesis, together with decreased weight of the prostate gland. These findings were largely reversible within the recovery period. In a small number of rats, in a 24 months oncogenicity study, a low incidence of benign histological changes were seen in the non-glandular part of the fore stomach. Erosions, ulcers, necrosis and inflammation were seen at varying degrees of severity. The clinical relevance of these findings is unknown. The increased incidence of adenomatous tumours in the rat pituitary observed with Decapeptyl following long-term repeated dosing is thought to be a class specific action of GnRH analogues due to a hormonally-mediated mechanism and has not been found in the mouse nor has it been described in man.
Standard mutagenicity testing revealed no mutagenic activity of triptorelin.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.