DIASTAT Gel Ref.[10827] Active ingredients: Diazepam
Source: FDA, National Drug Code (US) Revision Year: 2021
2. Clinical Pharmacology
Mechanism of Action
Although the precise mechanism by which diazepam exerts its antiseizure effects is unknown, animal and in vitro studies suggest that diazepam acts to suppress seizures through an interaction with γ-aminobutyric acid (GABA) receptors of the A-type (GABAA). GABA, the major inhibitory neurotransmitter in the central nervous system (CNS), acts at this receptor to open the membrane channel allowing chloride ions to flow into neurons. Entry of chloride ions causes an inhibitory potential that reduces the ability of neurons to depolarize to the threshold potential necessary to produce action potentials. Excessive depolarization of neurons is implicated in the generation and spread of seizures. It is believed that diazepam enhances the actions of GABA by causing GABA to bind more tightly to the GABAA receptor.
Pharmacokinetics
Pharmacokinetic information of diazepam following rectal administration was obtained from studies conducted in healthy adult subjects. No pharmacokinetic studies were conducted in pediatric patients. Therefore, information from the literature is used to define pharmacokinetic labeling in the pediatric population.
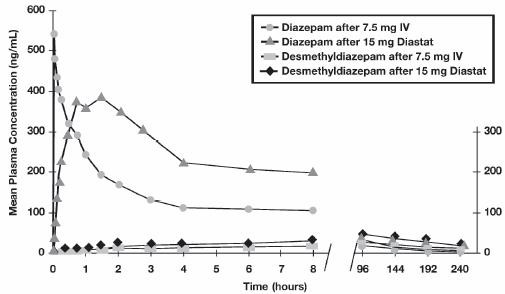
Diazepam rectal gel is well absorbed following rectal administration, reaching peak plasma concentrations in 1.5 hours. The absolute bioavailability of diazepam rectal gel relative to Valium injectable is 90%. The volume of distribution of diazepam rectal gel is calculated to be approximately 1 L/kg. The mean elimination half-life of diazepam and desmethyldiazepam following administration of a 15 mg dose of diazepam rectal gel was found to be about 46 hours (CV=43%) and 71 hours (CV=37%), respectively.
Both diazepam and its major active metabolite desmethyldiazepam bind extensively to plasma proteins (95-98%).
Metabolism and Elimination
It has been reported in the literature that diazepam is extensively metabolized to one major active metabolite (desmethyldiazepam) and two minor active metabolites, 3-hydroxydiazepam (temazepam) and 3-hydroxy-N-diazepam (oxazepam) in plasma. At therapeutic doses, desmethyldiazepam is found in plasma at concentrations equivalent to those of diazepam while oxazepam and temazepam are not usually detectable. The metabolism of diazepam is primarily hepatic and involves demethylation (involving primarily CYP2C19 and CYP3A4) and 3-hydroxylation (involving primarily CYP3A4), followed by glucuronidation. The marked inter-individual variability in the clearance of diazepam reported in the literature is probably attributable to variability of CYP2C19 (which is known to exhibit genetic polymorphism; about 3-5% of Caucasians have little or no activity and are "poor metabolizers") and CYP3A4. No inhibition was demonstrated in the presence of inhibitors selective for CYP2A6, CYP2C9, CYP2D6, CYP2E1, or CYP1A2, indicating that these enzymes are not significantly involved in metabolism of diazepam.
Special Populations
Hepatic Impairment
No pharmacokinetic studies were conducted with diazepam rectal gel in hepatically impaired subjects. Literature review indicates that following administration of 0.1 to 0.15 mg/kg of diazepam intravenously, the half-life of diazepam was prolonged by two to five-fold in subjects with alcoholic cirrhosis (n=24) compared to age-matched control subjects (n=37) with a corresponding decrease in clearance by half: however, the exact degree of hepatic impairment in these subjects was not characterized in this literature (see PRECAUTIONS).
Renal Impairment
The pharmacokinetics of diazepam have not been studied in renally impaired subjects (see PRECAUTIONS).
Pediatrics
No pharmacokinetic studies were conducted with diazepam rectal gel in the pediatric population. However, literature review indicates that following IV administration (0.33 mg/kg), diazepam has a longer half-life in neonates (birth up to one month; approximately 50-95 hours) and infants (one month up to two years; about 40-50 hours), whereas it has a shorter half-life in children (two to 12 years; approximately 15-21 hours) and adolescents (12 to 16 years; about 18-20 hours) (see PRECAUTIONS).
Elderly
A study of single dose IV administration of diazepam (0.1 mg/kg) indicates that the elimination half-life of diazepam increases linearly with age, ranging from about 15 hours at 18 years (healthy young adults) to about 100 hours at 95 years (healthy elderly) with a corresponding decrease in clearance of free diazepam (see PRECAUTIONS and DOSAGE AND ADMINISTRATION).
Effect of Gender, Race, and Cigarette Smoking
No targeted pharmacokinetic studies have been conducted to evaluate the effect of gender, race, and cigarette smoking on the pharmacokinetics of diazepam. However, covariate analysis of a population of treated patients following administration of diazepam rectal gel, indicated that neither gender nor cigarette smoking had any effect on the pharmacokinetics of diazepam.
Clinical Studies
The effectiveness of diazepam rectal gel has been established in two adequate and well controlled clinical studies in children and adults exhibiting the seizure pattern described below under INDICATIONS AND USAGE.
A randomized, double-blind study compared sequential doses of diazepam rectal gel and placebo in 91 patients (47 children, 44 adults) exhibiting the appropriate seizure profile. The first dose was given at the onset of an identified episode. Children were dosed again four hours after the first dose and were observed for a total of 12 hours. Adults were dosed at four and 12 hours after the first dose and were observed for a total of 24 hours. Primary outcomes for this study were seizure frequency during the period of observation and a global assessment that took into account the severity and nature of the seizures as well as their frequency.
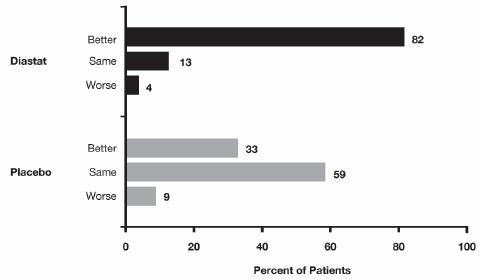
The median seizure frequency for the diazepam rectal gel treated group was zero seizures per hour, compared to a median seizure frequency of 0.3 seizures per hour for the placebo group, a difference that was statistically significant (p <0.0001). All three categories of the global assessment (seizure frequency, seizure severity, and "overall") were also found to be statistically significant in favor of diazepam rectal gel (p < 0.0001). The following histogram displays the results for the "overall" category of the global assessment.
Patients treated with diazepam rectal gel experienced prolonged time-to-next-seizure compared to placebo (p = 0.0002) as shown in the following graph.
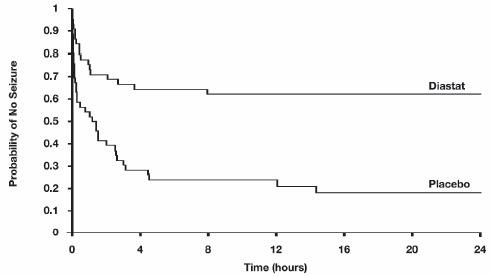
In addition, 62% of patients treated with diazepam rectal gel were seizure-free during the observation period compared to 20% of placebo patients.
Analysis of response by gender and age revealed no substantial differences between treatment in either of these subgroups. Analysis of response by race was considered unreliable, due to the small percentage of non-Caucasians.
A second double-blind study compared single doses of diazepam rectal gel and placebo in 114 patients (53 children, 61 adults). The dose was given at the onset of the identified episode and patients were observed for a total of 12 hours. The primary outcome in this study was seizure frequency. The median seizure frequency for the diazepam rectal gel-treated group was zero seizures per 12 hours, compared to a median seizure frequency of 2.0 seizures per 12 hours for the placebo group, a difference that was statistically significant (p <0.03). Patients treated with diazepam rectal gel experienced prolonged time-to-next-seizure compared to placebo (p = 0.0072) as shown in the following graph.
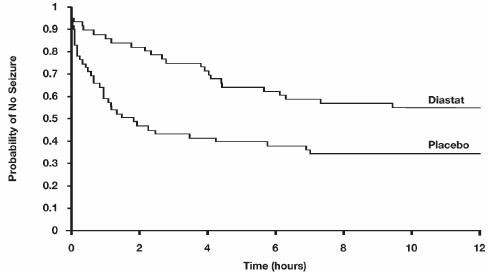
In addition, 55% of patients treated with diazepam rectal gel were seizure-free during the observation period compared to 34% of patients receiving placebo. Overall, caregivers judged diazepam rectal gel to be more effective than placebo (p = 0.018), based on a 10 centimeter visual analog scale. In addition, investigators also evaluated the effectiveness of diazepam rectal gel and judged diazepam rectal gel to be more effective than placebo (p <0.001).
An analysis of response by gender revealed a statistically significant difference between treatments in females but not in males in this study, and the difference between the 2 genders in response to the treatments reached borderline statistical significance. Analysis of response by race was considered unreliable, due to the small percentage of non-Caucasians.
6.6. Carcinogenesis, Mutagenesis, Impairment of Fertility
The carcinogenic potential of rectal diazepam has not been evaluated. In studies in which mice and rats were administered diazepam in the diet at a dose of 75 mg/kg/day (approximately six and 12 times, respectively, the maximum recommended human dose [MRHD=1 mg/kg/day] on a mg/m2 basis) for 80 and 104 weeks, respectively, an increased incidence of liver tumors was observed in males of both species.
The data currently available are inadequate to determine the mutagenic potential of diazepam.
Reproduction studies in rats showed decreases in the number of pregnancies and in the number of surviving offspring following administration of an oral dose of 100 mg/kg/day (approximately 16 times the MRHD on a mg/m2 basis) prior to and during mating and throughout gestation and lactation. No adverse effects on fertility or offspring viability were noted at a dose of 80 mg/kg/day (approximately 13 times the MRHD on a mg/m2 basis).
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.