DIOVAN Tablet Ref.[10570] Active ingredients: Valsartan
Source: FDA, National Drug Code (US) Revision Year: 2020
12.1. Mechanism of Action
Angiotensin II is formed from angiotensin I in a reaction catalyzed by angiotensin-converting enzyme (ACE, kininase II). Angiotensin II is the principal pressor agent of the renin-angiotensin system, with effects that include vasoconstriction, stimulation of synthesis and release of aldosterone, cardiac stimulation, and renal reabsorption of sodium. Diovan (valsartan) blocks the vasoconstrictor and aldosterone-secreting effects of angiotensin II by selectively blocking the binding of angiotensin II to the AT1 receptor in many tissues, such as vascular smooth muscle and the adrenal gland. Its action is therefore independent of the pathways for angiotensin II synthesis.
There is also an AT2 receptor found in many tissues, but AT2 is not known to be associated with cardiovascular homeostasis. Valsartan has much greater affinity (about 20,000-fold) for the AT1 receptor than for the AT2 receptor. The increased plasma levels of angiotensin II following AT1 receptor blockade with valsartan may stimulate the unblocked AT2 receptor. The primary metabolite of valsartan is essentially inactive with an affinity for the AT1 receptor about one-200th that of valsartan itself.
Blockade of the renin-angiotensin system with ACE inhibitors, which inhibit the biosynthesis of angiotensin II from angiotensin I, is widely used in the treatment of hypertension. ACE inhibitors also inhibit the degradation of bradykinin, a reaction also catalyzed by ACE. Because valsartan does not inhibit ACE (kininase II), it does not affect the response to bradykinin. Whether this difference has clinical relevance is not yet known. Valsartan does not bind to or block other hormone receptors or ion channels known to be important in cardiovascular regulation.
Blockade of the angiotensin II receptor inhibits the negative regulatory feedback of angiotensin II on renin secretion, but the resulting increased plasma renin activity and angiotensin II circulating levels do not overcome the effect of valsartan on blood pressure.
12.2. Pharmacodynamics
Valsartan inhibits the pressor effect of angiotensin II infusions. An oral dose of 80 mg inhibits the pressor effect by about 80% at peak with approximately 30% inhibition persisting for 24 hours. No information on the effect of larger doses is available.
Removal of the negative feedback of angiotensin II causes a 2- to 3-fold rise in plasma renin and consequent rise in angiotensin II plasma concentration in hypertensive patients. Minimal decreases in plasma aldosterone were observed after administration of valsartan; very little effect on serum potassium was observed.
In multiple-dose studies in hypertensive patients with stable renal insufficiency and patients with renovascular hypertension, valsartan had no clinically significant effects on glomerular filtration rate, filtration fraction, creatinine clearance, or renal plasma flow.
In multiple-dose studies in hypertensive patients, valsartan had no notable effects on total cholesterol, fasting triglycerides, fasting serum glucose, or uric acid.
12.3. Pharmacokinetics
Absorption
In healthy volunteers, valsartan peak plasma concentration is reached 2 to 4 hours after dosing. Valsartan shows bi-exponential decay kinetics following intravenous administration, with an average elimination half-life of about 6 hours. Absolute bioavailability for Diovan is about 25% (range 10% to 35%). The bioavailability of the suspension [see Dosage and Administration (2.2)] is 1.6 times as great as with the tablet. AUC and Cmax values of valsartan increase approximately linearly with increasing dose over the clinical dosing range (80-320 mg). Valsartan does not accumulate appreciably in plasma following repeated administration of 200 mg once daily.
In heart failure patients, the average time to peak plasma concentration and elimination half-life of valsartan are similar to those observed in healthy volunteers. The average accumulation factor is about 1.7 in heart failure patients following repeated administration of 160 mg twice daily. AUC and Cmax values of valsartan increase linearly and are almost proportional with increasing dose from 40 to 160 mg twice a day.
Effect of Food
With the tablet, food decreases the exposure (as measured by AUC) to valsartan by about 40% and peak plasma concentration (Cmax) by about 50%. Diovan can be administered with or without food.
Distribution
The steady state volume of distribution of valsartan after intravenous administration is small (17 L), indicating that valsartan does not distribute into tissues extensively. Valsartan is highly bound to serum proteins (95%), mainly serum albumin.
Metabolism
The primary metabolite, accounting for about 9% of dose, is valeryl 4-hydroxy valsartan. In vitro metabolism studies involving recombinant CYP 450 enzymes indicated that the CYP 2C9 isoenzyme is responsible for the formation of valeryl-4-hydroxy valsartan. Valsartan does not inhibit CYP 450 isozymes at clinically relevant concentrations. CYP 450 mediated drug interaction between valsartan and coadministered drugs are unlikely because of the low extent of metabolism.
Excretion
Valsartan, when administered as an oral solution, is primarily recovered in feces (about 83% of dose) and urine (about 13% of dose). The recovery is mainly as unchanged drug, with only about 20% of dose recovered as metabolites.
Following intravenous administration, plasma clearance of valsartan is about 2 L/h and its renal clearance is 0.62 L/h (about 30% of total clearance).
The apparent clearance of valsartan following oral administration is approximately 4.5 L/h in heart failure patients. Age does not affect the apparent clearance in heart failure patients.
Specific Populations
Geriatric: Exposure (measured by AUC) to valsartan is higher by 70% and the half-life is longer by 35% in the elderly than in the young [see Use in Specific Populations (8.5)].
Pediatric: In a study of pediatric hypertensive patients (n=26, 1 to 16 years of age) given single doses of a suspension of Diovan (mean: 0.9 to 2 mg/kg), the clearance (L/h/kg) of valsartan for children was similar to that of adults receiving the same formulation.
Gender: Pharmacokinetics of valsartan does not differ significantly between males and females.
Renal Insufficiency: There is no apparent correlation between renal function (measured by creatinine clearance) and exposure (measured by AUC) to valsartan in patients with different degrees of renal impairment (down to creatinine clearance of 10 mL/min). Valsartan is not removed from the plasma by hemodialysis [see Use in Specific Populations (8.6)].
Hepatic Insufficiency: On average, patients with mild-to-moderate chronic liver disease have twice the exposure (measured by AUC values) to valsartan of healthy volunteers (matched by age, sex, and weight) [see Use in Specific Populations (8.7)].
Drug Interaction Studies
No clinically significant pharmacokinetic interactions were observed when Diovan (valsartan) was coadministered with amlodipine, atenolol, cimetidine, digoxin, furosemide, glyburide, hydrochlorothiazide, or indomethacin. The valsartan-atenolol combination was more antihypertensive than either component, but it did not lower the heart rate more than atenolol alone.
Coadministration of valsartan and warfarin did not change the pharmacokinetics of valsartan or the time-course of the anticoagulant properties of warfarin.
Transporters: The results from an in vitro study with human liver tissue indicate that valsartan is a substrate of the hepatic uptake transporter OATP1B1 and the hepatic efflux transporter MRP2. Coadministration of inhibitors of the uptake transporter (rifampin, cyclosporine) or efflux transporter (ritonavir) may increase the systemic exposure to valsartan.
13.1. Carcinogenesis, Mutagenesis, Impairment of Fertility
There was no evidence of carcinogenicity when valsartan was administered in the diet to mice and rats for up to 2 years at doses up to 160 and 200 mg/kg/day, respectively. These doses in mice and rats are about 2.6 and 6 times, respectively, the MRHD on a mg/m2 basis (Calculations assume an oral dose of 320 mg/day and a 60-kg patient).
Mutagenicity assays did not reveal any valsartan-related effects at either the gene or chromosome level. These assays included bacterial mutagenicity tests with Salmonella (Ames) and E coli; a gene mutation test with Chinese hamster V79 cells; a cytogenetic test with Chinese hamster ovary cells; and a rat micronucleus test.
Valsartan had no adverse effects on the reproductive performance of male or female rats at oral doses up to 200 mg/kg/day. This dose is 6 times the MRHD on a mg/m2 basis (Calculations assume an oral dose of 320 mg/day and a 60-kg patient).
13.2. Animal Toxicology and/or Pharmacology
Daily oral dosing of neonatal/juvenile rats with valsartan at doses as low as 1 mg/kg/day (about 10% of the maximum recommended pediatric dose on a mg/m2 basis) from postnatal day 7 to postnatal day 70 produced persistent, irreversible kidney damage. These kidney effects in neonatal rats represent expected exaggerated pharmacological effects that are observed if rats are treated during the first 13 days of life.
14. Clinical Studies
14.1 Hypertension
Adult Hypertension
The antihypertensive effects of Diovan (valsartan) were demonstrated principally in 7 placebo-controlled, 4- to 12-week trials (1 in patients over 65 years) of dosages from 10 to 320 mg/day in patients with baseline diastolic blood pressures of 95-115 mmHg. The studies allowed comparison of once-daily and twice-daily regimens of 160 mg/day; comparison of peak and trough effects; comparison (in pooled data) of response by gender, age, and race; and evaluation of incremental effects of hydrochlorothiazide.
Administration of valsartan to patients with essential hypertension results in a significant reduction of sitting, supine, and standing systolic and diastolic blood pressure, usually with little or no orthostatic change.
In most patients, after administration of a single oral dose, onset of antihypertensive activity occurs at approximately 2 hours, and maximum reduction of blood pressure is achieved within 6 hours. The antihypertensive effect persists for 24 hours after dosing, but there is a decrease from peak effect at lower doses (40 mg) presumably reflecting loss of inhibition of angiotensin II. At higher doses, however (160 mg), there is little difference in peak and trough effect. During repeated dosing, the reduction in blood pressure with any dose is substantially present within 2 weeks, and maximal reduction is generally attained after 4 weeks. In long-term follow-up studies (without placebo control), the effect of valsartan appeared to be maintained for up to 2 years. The antihypertensive effect is independent of age, gender or race. The latter finding regarding race is based on pooled data and should be viewed with caution, because antihypertensive drugs that affect the renin-angiotensin system (that is, ACE inhibitors and angiotensin-II blockers) have generally been found to be less effective in low-renin hypertensives (frequently blacks) than in high-renin hypertensives (frequently whites). In pooled, randomized, controlled trials of Diovan that included a total of 140 blacks and 830 whites, valsartan and an ACE-inhibitor control were generally at least as effective in blacks as whites. The explanation for this difference from previous findings is unclear.
Abrupt withdrawal of valsartan has not been associated with a rapid increase in blood pressure.
The blood pressure-lowering effect of valsartan and thiazide-type diuretics are approximately additive.
The 7 studies of valsartan monotherapy included over 2,000 patients randomized to various doses of valsartan and about 800 patients randomized to placebo. Doses below 80 mg were not consistently distinguished from those of placebo at trough, but doses of 80, 160 and 320 mg produced dose-related decreases in systolic and diastolic blood pressure, with the difference from placebo of approximately 6-9/3-5 mmHg at 80 to 160 mg and 9/6 mmHg at 320 mg. In a controlled trial the addition of HCTZ to valsartan 80 mg resulted in additional lowering of systolic and diastolic blood pressure by approximately 6/3 and 12/5 mmHg for 12.5 and 25 mg of HCTZ, respectively, compared to valsartan 80 mg alone.
Patients with an inadequate response to 80 mg once daily were titrated to either 160 mg once daily or 80 mg twice daily, which resulted in a similar response in both groups.
In controlled trials, the antihypertensive effect of once-daily valsartan 80 mg was similar to that of once-daily enalapril 20 mg or once-daily lisinopril 10 mg.
There are no trials of Diovan demonstrating reductions in cardiovascular risk in patients with hypertension, but at least one pharmacologically similar drug has demonstrated such benefits.
There was essentially no change in heart rate in valsartan-treated patients in controlled trials.
Pediatric Hypertension
The antihypertensive effects of Diovan were evaluated in two randomized, double-blind clinical studies.
In a clinical study involving 261 hypertensive pediatric patients 6 to 16 years of age, patients who weighed <35 kg received 10, 40 or 80 mg of valsartan daily (low, medium and high doses), and patients who weighed ≥35 kg received 20, 80, and 160 mg of valsartan daily (low, medium and high doses). Renal and urinary disorders, and essential hypertension with or without obesity were the most common underlying causes of hypertension in children enrolled in this study. At the end of 2 weeks, valsartan reduced both systolic and diastolic blood pressure in a dose-dependent manner. Overall, the three dose levels of valsartan (low, medium and high) significantly reduced systolic blood pressure by -8, -10, -12 mm Hg from the baseline, respectively. Patients were re-randomized to either continue receiving the same dose of valsartan or were switched to placebo. In patients who continued to receive the medium and high doses of valsartan, systolic blood pressure at trough was -4 and -7 mm Hg lower than patients who received the placebo treatment. In patients receiving the low dose of valsartan, systolic blood pressure at trough was similar to that of patients who received the placebo treatment. Overall, the dose-dependent antihypertensive effect of valsartan was consistent across all the demographic subgroups.
In a clinical study involving 90 hypertensive pediatric patients 1 to 5 years of age with a similar study design, there was some evidence of effectiveness, but safety findings for which a relationship to treatment could not be excluded mitigate against recommending use in this age group [see Adverse Reactions (6.1)].
14.2 Heart Failure
The Valsartan Heart Failure Trial (Val-HeFT) was a multinational, double-blind study in which 5,010 patients with NYHA class II (62%) to IV (2%) heart failure and LVEF < 40%, on baseline therapy chosen by their physicians, were randomized to placebo or valsartan (titrated from 40 mg twice daily to the highest tolerated dose or 160 mg twice daily) and followed for a mean of about 2 years. Although Val-HeFT's primary goal was to examine the effect of valsartan when added to an ACE inhibitor, about 7% were not receiving an ACE inhibitor. Other background therapy included diuretics (86%), digoxin (67%), and beta-blockers (36%). The population studied was 80% male, 46% 65 years or older and 89% Caucasian. At the end of the trial, patients in the valsartan group had a blood pressure that was 4 mmHg systolic and 2 mmHg diastolic lower than the placebo group. There were two primary end points, both assessed as time to first event: all-cause mortality and heart failure morbidity, the latter defined as all-cause mortality, sudden death with resuscitation, hospitalization for heart failure, and the need for intravenous inotropic or vasodilatory drugs for at least 4 hours. These results are summarized in the following table.
| Placebo | Valsartan | Hazard Ratio | Nominal | |
|---|---|---|---|---|
| (N=2,499) | (N=2,511) | (95% CI*) | p-value | |
| All-cause mortality | 484 | 495 | 1.02 | 0.8 |
| (19.4%) | (19.7%) | (0.90-1.15) | ||
| HF morbidity | 801 | 723 | 0.87 | 0.009 |
| (32.1%) | (28.8%) | (0.79-0.97) |
* CI = Confidence Interval
Although the overall morbidity result favored valsartan, this result was largely driven by the 7% of patients not receiving an ACE inhibitor, as shown in the following table.
| Without ACE Inhibitor | With ACE Inhibitor | |||
|---|---|---|---|---|
| Placebo | Valsartan | Placebo | Valsartan | |
| (N=181) | (N=185) | (N=2,318) | (N=2,326) | |
| Events (%) | 77 (42.5%) | 46 (24.9%) | 724 (31.2%) | 677 (29.1%) |
| Hazard ratio (95% CI) | 0.51 (0.35, 0.73) | 0.92 (0.82, 1.02) | ||
| p-value | 0.0002 | 0.0965 | ||
The modest favorable trend in the group receiving an ACE inhibitor was largely driven by the patients receiving less than the recommended dose of ACE inhibitor. Thus, there is little evidence of further clinical benefit when valsartan is added to an adequate dose of ACE inhibitor.
Secondary end points in the subgroup not receiving ACE inhibitors were as follows.
| Placebo | Valsartan | Hazard Ratio | |
|---|---|---|---|
| (N=181) | (N=185) | (95% CI) | |
| Components of HF morbidity | |||
| All-cause mortality | 49 (27.1%) | 32 (17.3%) | 0.59 (0.37, 0.91) |
| Sudden death with resuscitation | 2 (1.1%) | 1 (0.5%) | 0.47 (0.04, 5.20) |
| CHF therapy | 1 (0.6%) | 0 (0.0%) | – |
| CHF hospitalization | 48 (26.5%) | 24 (13.0%) | 0.43 (0.27, 0.71) |
| Cardiovascular mortality | 40 (22.1%) | 29 (15.7%) | 0.65 (0.40, 1.05) |
| Non-fatal morbidity | 49 (27.1%) | 24 (13.0%) | 0.42 (0.26, 0.69) |
In patients not receiving an ACE inhibitor, valsartan-treated patients had an increase in ejection fraction and reduction in left ventricular internal diastolic diameter (LVIDD).
Effects were generally consistent across subgroups defined by age and gender for the population of patients not receiving an ACE inhibitor. The number of black patients was small and does not permit a meaningful assessment in this subset of patients.
14.3 Post-Myocardial Infarction
The VALsartan In Acute myocardial iNfarcTion trial (VALIANT) was a randomized, controlled, multinational, double-blind study in 14,703 patients with acute myocardial infarction and either heart failure (signs, symptoms or radiological evidence) or left ventricular systolic dysfunction (ejection fraction ≤40% by radionuclide ventriculography or ≤35% by echocardiography or ventricular contrast angiography). Patients were randomized within 12 hours to 10 days after the onset of myocardial infarction symptoms to one of three treatment groups: valsartan (titrated from 20 or 40 mg twice daily to the highest tolerated dose up to a maximum of 160 mg twice daily), the ACE inhibitor, captopril (titrated from 6.25 mg three times daily to the highest tolerated dose up to a maximum of 50 mg three times daily), or the combination of valsartan plus captopril. In the combination group, the dose of valsartan was titrated from 20 mg twice daily to the highest tolerated dose up to a maximum of 80 mg twice daily; the dose of captopril was the same as for monotherapy. The population studied was 69% male, 94% Caucasian, and 53% were 65 years of age or older. Baseline therapy included aspirin (91%), beta-blockers (70%), ACE inhibitors (40%), thrombolytics (35%) and statins (34%). The mean treatment duration was 2 years. The mean daily dose of Diovan in the monotherapy group was 217 mg.
The primary endpoint was time to all-cause mortality. Secondary endpoints included (1) time to cardiovascular (CV) mortality, and (2) time to the first event of cardiovascular mortality, reinfarction, or hospitalization for heart failure. The results are summarized in the following table.
| Valsartan vs. Captopril (N=4,909) (N=4,909) | Valsartan + Captopril vs. Captopril (N=4,885) (N=4,909) | |||||
|---|---|---|---|---|---|---|
| No. of Deaths Valsartan/Captopril | Hazard Ratio CI | p-value | No. of Deaths Comb/Captopril | Hazard Ratio CI | p-value | |
| All-cause mortality | 979 (19.9%) /958 (19.5%) | 1.001 (0.902, 1.111) | 0.98 | 941 (19.3%) /958 (19.5%) | 0.984 (0.886, 1.093) | 0.73 |
| CV mortality | 827 (16.8%) /830 (16.9%) | 0.976 (0.875, 1.090) | ||||
| CV mortality, hospitalization for HF, and recurrent non-fatal MI | 1,529 (31.1%) /1,567 (31.9%) | 0.955 (0.881, 1.035) | ||||
There was no difference in overall mortality among the three treatment groups. There was thus no evidence that combining the ACE inhibitor captopril and the angiotensin II blocker valsartan was of value.
The data were assessed to see whether the effectiveness of valsartan could be demonstrated by showing in a non-inferiority analysis that it preserved a fraction of the effect of captopril, a drug with a demonstrated survival effect in this setting. A conservative estimate of the effect of captopril (based on a pooled analysis of 3 post-infarction studies of captopril and 2 other ACE inhibitors) was a 14% to 16% reduction in mortality compared to placebo. Valsartan would be considered effective if it preserved a meaningful fraction of that effect and unequivocally preserved some of that effect. As shown in the table, the upper bound of the CI for the hazard ratio (valsartan/captopril) for overall or CV mortality is 1.09 to 1.11, a difference of about 9% to 11%, thus making it unlikely that valsartan has less than about half of the estimated effect of captopril and clearly demonstrating an effect of valsartan. The other secondary endpoints were consistent with this conclusion.
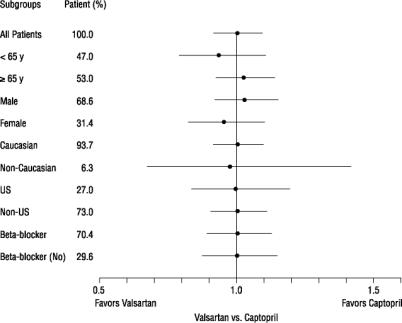
There were no clear differences in all-cause mortality based on age, gender, race, or baseline therapies, as shown in the figure above.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.