Source: FDA, National Drug Code (US) Revision Year: 2021
Effient is contraindicated in patients with active pathological bleeding such as peptic ulcer or intracranial hemorrhage [see Warnings and Precautions (5.1) and Adverse Reactions (6.1)].
Effient is contraindicated in patients with a history of prior transient ischemic attack (TIA) or stroke. In TRITON-TIMI 38 (TRial to Assess Improvement in Therapeutic Outcomes by Optimizing Platelet InhibitioN with Prasugrel), patients with a history of TIA or ischemic stroke (>3 months prior to enrollment) had a higher rate of stroke on Effient (6.5%; of which 4.2% were thrombotic stroke and 2.3% were intracranial hemorrhage [ICH]) than on clopidogrel (1.2%; all thrombotic). In patients without such a history, the incidence of stroke was 0.9% (0.2% ICH) and 1.0% (0.3% ICH) with Effient and clopidogrel, respectively. Patients with a history of ischemic stroke within 3 months of screening and patients with a history of hemorrhagic stroke at any time were excluded from TRITON-TIMI 38. Patients who experience a stroke or TIA while on Effient generally should have therapy discontinued [see Adverse Reactions (6.1) and Clinical Studies (14)].
Effient is contraindicated in patients with hypersensitivity (e.g., anaphylaxis) to prasugrel or any component of the product [see Adverse Reactions (6.2)].
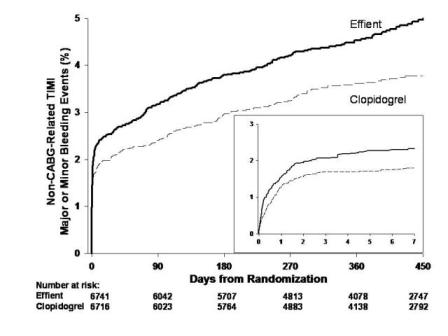
Thienopyridines, including Effient, increase the risk of bleeding. With the dosing regimens used in TRITON-TIMI 38, TIMI (Thrombolysis in Myocardial Infarction) Major (clinically overt bleeding associated with a fall in hemoglobin ≥5 g/dL, or intracranial hemorrhage) and TIMI Minor (overt bleeding associated with a fall in hemoglobin of ≥3 g/dL but <5 g/dL) bleeding events were more common on Effient than on clopidogrel [see Adverse Reactions (6.1)]. The bleeding risk is highest initially, as shown in Figure 1 (events through 450 days; inset shows events through 7 days).
Figure 1. Non-CABG-Related TIMI Major or Minor Bleeding Events:
Suspect bleeding in any patient who is hypotensive and has recently undergone coronary angiography, PCI, CABG, or other surgical procedures even if the patient does not have overt signs of bleeding.
Do not use Effient in patients with active bleeding, prior TIA or stroke [see Contraindications (4.1, 4.2)].
Other risk factors for bleeding are:
Thienopyridines inhibit platelet aggregation for the lifetime of the platelet (7-10 days), so withholding a dose will not be useful in managing a bleeding event or the risk of bleeding associated with an invasive procedure. Because the half-life of prasugrel’s active metabolite is short relative to the lifetime of the platelet, it may be possible to restore hemostasis by administering exogenous platelets; however, platelet transfusions within 6 hours of the loading dose or 4 hours of the maintenance dose may be less effective.
The risk of bleeding is increased in patients receiving Effient who undergo CABG. If possible, Effient should be discontinued at least 7 days prior to CABG.
Of the 437 patients who underwent CABG during TRITON-TIMI 38, the rates of CABG-related TIMI Major or Minor bleeding were 14.1% in the Effient group and 4.5% in the clopidogrel group [see Adverse Reactions (6.1)]. The higher risk for bleeding events in patients treated with Effient persisted up to 7 days from the most recent dose of study drug. For patients receiving a thienopyridine within 3 days prior to CABG, the frequencies of TIMI Major or Minor bleeding were 26.7% (12 of 45 patients) in the Effient group, compared with 5.0% (3 of 60 patients) in the clopidogrel group. For patients who received their last dose of thienopyridine within 4 to 7 days prior to CABG, the frequencies decreased to 11.3% (9 of 80 patients) in the prasugrel group and 3.4% (3 of 89 patients) in the clopidogrel group.
Do not start Effient in patients likely to undergo urgent CABG. CABG-related bleeding may be treated with transfusion of blood products, including packed red blood cells and platelets; however, platelet transfusions within 6 hours of the loading dose or 4 hours of the maintenance dose may be less effective.
Discontinue thienopyridines, including Effient, for active bleeding, elective surgery, stroke, or TIA. The optimal duration of thienopyridine therapy is unknown. In patients who are managed with PCI and stent placement, premature discontinuation of any antiplatelet medication, including thienopyridines, conveys an increased risk of stent thrombosis, myocardial infarction, and death. Patients who require premature discontinuation of a thienopyridine will be at increased risk for cardiac events. Lapses in therapy should be avoided, and if thienopyridines must be temporarily discontinued because of an adverse event(s), they should be restarted as soon as possible [see Contraindications (4.1, 4.2) and Warnings and Precautions (5.1)].
Thrombotic thrombocytopenic purpura (TTP) has been reported with the use of Effient. TTP can occur after a brief exposure (<2 weeks). TTP is a serious condition that can be fatal and requires urgent treatment, including plasmapheresis (plasma exchange). TTP is characterized by thrombocytopenia, microangiopathic hemolytic anemia (schistocytes [fragment red blood cells] seen on peripheral smear), neurological findings, renal dysfunction, and fever [see Adverse Reactions (6.2)].
Hypersensitivity including angioedema has been reported in patients receiving Effient, including patients with a history of hypersensitivity reaction to other thienopyridines [see Contraindications (4.3) and Adverse Reactions (6.2)].
The following serious adverse reactions are also discussed elsewhere in the labeling:
Safety in patients with ACS undergoing PCI was evaluated in a clopidogrel-controlled study, TRITON-TIMI 38, in which 6741 patients were treated with Effient (60-mg loading dose and 10-mg once daily) for a median of 14.5 months (5802 patients were treated for over 6 months; 4136 patients were treated for more than 1 year). The population treated with Effient was 27 to 96 years of age, 25% female, and 92% Caucasian. All patients in the TRITON-TIMI 38 study were to receive aspirin. The dose of clopidogrel in this study was a 300-mg loading dose and 75-mg once daily.
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared with the rates observed in other clinical trials of another drug and may not reflect the rates observed in practice.
The rate of study drug discontinuation because of adverse reactions was 7.2% for Effient and 6.3% for clopidogrel. Bleeding was the most common adverse reaction leading to study drug discontinuation for both drugs (2.5% for Effient and 1.4% for clopidogrel).
In TRITON-TIMI 38, overall rates of TIMI Major or Minor bleeding adverse reactions unrelated to coronary artery bypass graft surgery (CABG) were significantly higher on Effient than on clopidogrel, as shown in Table 1.
Table 1. Non-CABG-Related Bleeding a (TRITON-TIMI 38):
| Effient (%) (N=6741) | Clopidogrel (%) (N=6716) | |
|---|---|---|
| TIMI Major or Minor bleeding | 4.5 | 3.4 |
| TIMI Major bleedingb | 2.2 | 1.7 |
| Life-threatening | 1.3 | 0.8 |
| Fatal | 0.3 | 0.1 |
| Symptomatic intracranial hemorrhage (ICH) | 0.3 | 0.3 |
| Requiring inotropes | 0.3 | 0.1 |
| Requiring surgical intervention | 0.3 | 0.3 |
| Requiring transfusion (≥4 units) | 0.7 | 0.5 |
| TIMI Minor bleedingb | 2.4 | 1.9 |
a Patients may be counted in more than one row.
b See 5.1 for definition.
Figure 1 demonstrates non-CABG related TIMI Major or Minor bleeding. The bleeding rate is highest initially, as shown in Figure 1 (inset: Days 0 to 7) [see Warnings and Precautions (5.1)].
In TRITON-TIMI 38, non-CABG-related TIMI Major or Minor bleeding rates in patients with the risk factors of age ≥75 years and weight <60 kg are shown in Table 2.
Table 2. Bleeding Rates for Non-CABG-Related Bleeding by Weight and Age (TRITON-TIMI 38):
| Major/Minor | Fatal | |||
|---|---|---|---|---|
| Effienta (%) | Clopidogrelb (%) | Effienta (%) | Clopidogrelb (%) | |
| Weight <60 kg (N=308 Effient, N=356 clopidogrel) | 10.1 | 6.5 | 0.0 | 0.3 |
| Weight ≥60 kg (N=6373 Effient, N=6299 clopidogrel) | 4.2 | 3.3 | 0.3 | 0.1 |
| Age <75 years (N=5850 Effient, N=5822 clopidogrel) | 3.8 | 2.9 | 0.2 | 0.1 |
| Age ≥75 years (N=891 Effient, N=894 clopidogrel) | 9.0 | 6.9 | 1.0 | 0.1 |
a 10-mg Effient maintenance dose
b 75-mg clopidogrel maintenance dose
In TRITON-TIMI 38, 437 patients who received a thienopyridine underwent CABG during the course of the study. The rate of CABG-related TIMI Major or Minor bleeding was 14.1% for the Effient group and 4.5% in the clopidogrel group (see Table 3). The higher risk for bleeding adverse reactions in patients treated with Effient persisted up to 7 days from the most recent dose of study drug.
Table 3. CABG-Related Bleeding a (TRITON-TIMI 38):
| Effient (%) (N=213) | Clopidogrel (%) (N=224) | |
|---|---|---|
| TIMI Major or Minor bleeding | 14.1 | 4.5 |
| TIMI Major bleeding | 11.3 | 3.6 |
| Fatal | 0.9 | 0 |
| Reoperation | 3.8 | 0.5 |
| Transfusion of ≥5 units | 6.6 | 2.2 |
| Intracranial hemorrhage | 0 | 0 |
| TIMI Minor bleeding | 2.8 | 0.9 |
a Patients may be counted in more than one row.
Hemorrhagic events reported as adverse reactions in TRITON-TIMI 38 were, for Effient and clopidogrel, respectively: epistaxis (6.2%, 3.3%), gastrointestinal hemorrhage (1.5%, 1.0%), hemoptysis (0.6%, 0.5%), subcutaneous hematoma (0.5%, 0.2%), post-procedural hemorrhage (0.5%, 0.2%), retroperitoneal hemorrhage (0.3%, 0.2%), pericardial effusion/hemorrhage/tamponade (0.3%, 0.2%), and retinal hemorrhage (0.0%, 0.1%).
During TRITON-TIMI 38, newly-diagnosed malignancies were reported in 1.6% and 1.2% of patients treated with prasugrel and clopidogrel, respectively. The sites contributing to the differences were primarily colon and lung. In another Phase 3 clinical study of ACS patients not undergoing PCI, in which data for malignancies were prospectively collected, newly-diagnosed malignancies were reported in 1.8% and 1.7% of patients treated with prasugrel and clopidogrel, respectively. The site of malignancies was balanced between treatment groups except for colorectal malignancies. The rates of colorectal malignancies were 0.3% prasugrel, 0.1% clopidogrel and most were detected during investigation of GI bleed or anemia. It is unclear if these observations are causally-related, are the result of increased detection because of bleeding, or are random occurrences.
In TRITON-TIMI 38, common and other important non-hemorrhagic adverse events were, for Effient and clopidogrel, respectively: severe thrombocytopenia (0.06%, 0.04%), anemia (2.2%, 2.0%), abnormal hepatic function (0.22%, 0.27%), allergic reactions (0.36%, 0.36%), and angioedema (0.06%, 0.04%). Table 4 summarizes the adverse events reported by at least 2.5% of patients.
Table 4. Non-Hemorrhagic Treatment Emergent Adverse Events Reported by at Least 2.5% of Patients in Either Group:
| Effient (%) (N=6741) | Clopidogrel (%) (N=6716) | |
|---|---|---|
| Hypertension | 7.5 | 7.1 |
| Hypercholesterolemia/Hyperlipidemia | 7.0 | 7.4 |
| Headache | 5.5 | 5.3 |
| Back pain | 5.0 | 4.5 |
| Dyspnea | 4.9 | 4.5 |
| Nausea | 4.6 | 4.3 |
| Dizziness | 4.1 | 4.6 |
| Cough | 3.9 | 4.1 |
| Hypotension | 3.9 | 3.8 |
| Fatigue | 3.7 | 4.8 |
| Non-cardiac chest pain | 3.1 | 3.5 |
| Atrial fibrillation | 2.9 | 3.1 |
| Bradycardia | 2.9 | 2.4 |
| Leukopenia (<4 × 109 WBC/L) | 2.8 | 3.5 |
| Rash | 2.8 | 2.4 |
| Pyrexia | 2.7 | 2.2 |
| Peripheral edema | 2.7 | 3.0 |
| Pain in extremity | 2.6 | 2.6 |
| Diarrhea | 2.3 | 2.6 |
The following adverse reactions have been identified during post-approval use of Effient. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Blood and lymphatic system disorders: Thrombocytopenia, Thrombotic thrombocytopenic purpura (TTP) [see Warnings and Precautions (5.4) and Patient Counseling Information (17)]
Immune system disorders: Hypersensitivity reactions including anaphylaxis [see Contraindications (4.3)]
Coadministration of Effient and warfarin increases the risk of bleeding [see Warnings and Precautions (5.1) and Clinical Pharmacology (12.3)].
Coadministration of Effient and NSAIDs (used chronically) may increase the risk of bleeding [see Warnings and Precautions (5.1)].
As with other oral P2Y12 inhibitors, co-administration of opioid agonists delay and reduce the absorption of prasugrel’s active metabolite presumably because of slowed gastric emptying [see Clinical Pharmacology (12.3)]. Consider the use of a parenteral anti-platelet agent in acute coronary syndrome patients requiring co-administration of morphine or other opioid agonists.
Effient can be administered with drugs that are inducers or inhibitors of cytochrome P450 enzymes [see Clinical Pharmacology (12.3)].
Effient can be administered with aspirin (75-mg to 325-mg per day), heparin, GPIIb/IIIa inhibitors, statins, digoxin, and drugs that elevate gastric pH, including proton pump inhibitors and H2 blockers [see Clinical Pharmacology (12.3)].
There are no data with Effient use in pregnant women to inform a drug-associated risk. No structural malformations were observed in animal reproductive and developmental toxicology studies when rats and rabbits were administered prasugrel during organogenesis at doses of up to 30 times the recommended therapeutic exposures in humans [see Data]. Due to the mechanism of action of Effient, and the associated identified risk of bleeding, consider the benefits and risks of Effient and possible risks to the fetus when prescribing Effient to a pregnant woman [see Boxed Warning, and Warnings and Precautions (5.1, 5.3)].
The background risk of major birth defects and miscarriage for the indicated population is unknown. The background risk in the U.S. general population of major birth defects is 2-4% and of miscarriage is 15-20% of clinically recognized pregnancies.
In embryo fetal developmental toxicology studies, pregnant rats and rabbits received prasugrel at maternally toxic oral doses equivalent to more than 40 times the human exposure. A slight decrease in fetal body weight was observed; but, there were no structural malformations in either species. In prenatal and postnatal rat studies, maternal treatment with prasugrel had no effect on the behavioral or reproductive development of the offspring at doses greater than 150 times the human exposure.
There is no information regarding the presence of prasugrel in human milk, the effects on the breastfed infant, or the effects on milk production. Metabolites of prasugrel were found in rat milk [see Data]. The developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for Effient and any potential adverse effects on the breastfed child from Effient or from the underlying maternal condition.
Following a 5-mg/kg oral dose of [14C]-prasugrel to lactating rats, metabolites of prasugrel were detected in the maternal milk and blood.
Safety and effectiveness in pediatric patients have not been established.
In a randomized, placebo-controlled trial, the primary objective of reducing the rate of vaso-occlusive crisis (painful crisis or acute chest syndrome) in pediatric patients, aged 2 to less than 18 years, with sickle cell anemia was not met.
In TRITON-TIMI 38, 38.5% of patients were ≥65 years of age and 13.2% were ≥75 years of age. The risk of bleeding increased with advancing age in both treatment groups, although the relative risk of bleeding (Effient compared with clopidogrel) was similar across age groups.
Patients ≥75 years of age who received Effient 10-mg had an increased risk of fatal bleeding events (1.0%) compared to patients who received clopidogrel (0.1%). In patients ≥75 years of age, symptomatic intracranial hemorrhage occurred in 7 patients (0.8%) who received Effient and in 3 patients (0.3%) who received clopidogrel. Because of the risk of bleeding, and because effectiveness is uncertain in patients ≥75 years of age [see Clinical Studies (14)], use of Effient is generally not recommended in these patients, except in high-risk situations (diabetes and past history of myocardial infarction) where its effect appears to be greater and its use may be considered [see Warnings and Precautions (5.1), Clinical Pharmacology (12.3), and Clinical Studies (14)].
No dosage adjustment is necessary for patients with renal impairment. There is limited experience in patients with end-stage renal disease, but such patients are generally at higher risk of bleeding [see Warnings and Precautions (5.1) and Clinical Pharmacology (12.3)].
No dosage adjustment is necessary in patients with mild to moderate hepatic impairment (Child-Pugh Class A and B). The pharmacokinetics and pharmacodynamics of prasugrel in patients with severe hepatic disease have not been studied, but such patients are generally at higher risk of bleeding [see Warnings and Precautions (5.1) and Clinical Pharmacology (12.3)].
In TRITON-TIMI 38, 4.6% of patients treated with Effient had body weight <60 kg. Individuals with body weight <60 kg had an increased risk of bleeding and an increased exposure to the active metabolite of prasugrel [see Dosage and Administration (2), Warnings and Precautions (5.1), and Clinical Pharmacology (12.3)]. Consider lowering the maintenance dose to 5-mg in patients <60 kg. The effectiveness and safety of the 5-mg dose have not been prospectively studied [see Dosage and Administration (2) and Clinical Pharmacology (12.3)].
In healthy subjects, patients with stable atherosclerosis, and patients with ACS receiving prasugrel, there was no relevant effect of genetic variation in CYP2B6, CYP2C9, CYP2C19, or CYP3A5 on the pharmacokinetics of prasugrel’s active metabolite or its inhibition of platelet aggregation.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.