ENSACOVE Capsule Ref.[115492] Active ingredients: Ensartinib
Source: FDA, National Drug Code (US) Revision Year: 2024
12.1. Mechanism of Action
Ensartinib is a kinase inhibitor of anaplastic lymphoma kinase (ALK) and inhibits other kinases including MET and ROS1. In vitro, ensartinib inhibited phosphorylation of ALK and its downstream signaling proteins AKT, ERK, and S6, thereby blocking ALK-mediated signaling pathways and inhibiting proliferation in cell lines harboring ALK fusions and mutations. In vivo, ensartinib showed anti-tumor activity in a mouse xenograft model of human NSCLC harboring an ALK fusion.
12.2. Pharmacodynamics
Exposure-response relationship
Ensartinib exposure-response relationships and the time course of the pharmacodynamic response have not been fully characterized.
Cardiac Electrophysiology
At the approved recommended dosage, a mean increase in the QTc interval >20 ms was not observed.
12.3. Pharmacokinetics
Ensartinib mean (coefficient of variation [CV%]) maximum concentration (Cmax) is 292 ng/mL (60%), and the area under the concentration-time curve (AUC0–24h) is 4,920 ng·h/ml (62%) at the approved recommended dosage. Ensartinib steady state is reached within 15 days with a mean accumulation ratio of 2.7.
Absorption
Ensartinib median (minimum, maximum) time to reach Cmax (Tmax) at steady state is 3 hours (2, 8 hours).
Effect of Food
No clinically significant differences in ensartinib pharmacokinetics were observed following administration of ENSACOVE with a high-fat meal (total 800-1000 calories, >50% fat) compared to fasted conditions.
Distribution
Ensartinib mean (CV%) apparent volume of distribution is 1,720 L (42%). Ensartinib is 91.6% bound to human plasma protein.
Elimination
Ensartinib mean (standard deviation [SD]) steady-state half-life (t1/2) is 30 (20) hours.
Metabolism
Ensartinib is predominantly metabolized by CYP3A.
Excretion
Following a single oral 200 mg dose of radiolabeled ensartinib, 91% of the radioactivity was recovered in feces (38% as unchanged) and 10% in urine (4.4% as unchanged).
Specific Populations
No clinically significant differences in the pharmacokinetics of ensartinib were observed based on age (20 to 86 years), sex, race (Asian vs White), body weight (38 to 148 kg), mild to moderate renal impairment (eGFR 30 to 89 mL/min) and mild hepatic impairment (total bilirubin ≤ upper limit of normal (ULN) and AST > ULN or total bilirubin 1 to 1.5 x ULN and any AST).
The effect of severe renal impairment (eGFR 15 to 29 mL/min), end-stage renal disease (eGFR <15 mL/min) with or without hemodialysis, and moderate (total bilirubin >1.5 to ≤3 ULN and any AST) or severe (total bilirubin >3 times ULN and any AST) hepatic impairment on ensartinib pharmacokinetics is unknown.
Drug Interaction Studies
In Vitro Studies
Cytochrome P450 (CYP) Enzymes: Ensartinib does not inhibit CYP1A2, CYP2B6, CYP2C8, CYP2C9, CYP2C19, CYP2D6 and does not induce CYP1A2, CYP2B6, or CYP3A.
Transporter Systems: Ensartinib is a P-gp substrate but is not a substrate of BCRP, OATP1B1, OATP1B3, OAT1, OAT3, OCT1 or OCT2.
Ensartinib does not inhibit BCRP, P-gp, OATP1B1, OATP1B3, OAT1, OAT3, OCT1, OCT2 or OCT3.
13.1. Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenicity studies have not been conducted with ensartinib.
Ensartinib was not mutagenic in a bacterial reverse mutation (Ames) assay and was not clastogenic in an in vitro human lymphocyte chromosome aberration assay or an in vivo rat bone marrow micronucleus assay.
Dedicated fertility studies were not conducted with ensartinib. No adverse effects on male or female reproductive organs were observed in up to 3-month repeat-dose toxicology studies conducted in rats and dogs.
14. Clinical Studies
14.1 TKI-naive ALK-Positive Locally Advanced or Metastatic NSCLC (eXALT3 Study)
The efficacy of ENSACOVE was evaluated in the eXALT3 study (NCT02767804), an open-label, randomized, active-controlled, multicenter study in adult patients with locally advanced (stage IIIB following prior chemotherapy or chemoradiation or not amenable to curative intent therapy) or metastatic ALK-positive NSCLC. Patients were required to have ALK-positive NSCLC and an ECOG performance status of 0, 1, or 2. Patients could have received one prior regimen of chemotherapy but could not have previously received an ALK-targeted therapy.
Patients with asymptomatic, untreated brain metastases who were not on corticosteroids and patients with asymptomatic, treated brain metastases who were on stable or decreasing dose of corticosteroids were eligible. Patients were required to have completed radiation therapy at least 2 weeks, or chemotherapy at least 4 weeks, prior to enrollment. Patients with leptomeningeal disease were ineligible.
Patients were randomized 1:1 to receive ENSACOVE 225 mg orally once daily or crizotinib 250 mg orally twice daily in 28-day cycles until disease progression or unacceptable toxicity. Randomization was stratified by prior chemotherapy (0 vs. 1), ECOG performance status (0 or 1 vs. 2), presence of central nervous system (CNS) metastases (yes or no), and geographic region (Asia vs. the rest of the world). Tumor assessments were performed every 8 weeks.
The main efficacy outcome measure was progression-free survival (PFS) as evaluated by Blinded Independent Central Review (BICR) according to RECIST version 1.1. The key secondary efficacy outcome measure was overall survival (OS); other secondary outcome measures included CNS response rate, time to CNS progression, and overall response rate (ORR).
A total of 290 patients were randomized to ENSACOVE (n=143) or crizotinib (n=147). The baseline demographic characteristics of the overall study population were median age 54 years (range: 25-90); 16% age >65 years; 51% male; 56% Asian; 41% White and 1.4% Black; 8% Hispanic or Latino; ECOG PS 0 or 1 (95%); and 62% never smokers. Patients had Stage IIIB (8%) or Stage IV NSCLC (92%); 26% had received prior chemotherapy for advanced disease and 17% had received prior radiation. Baseline CNS metastases were present in 36% of the patients.
The eXALT3 study demonstrated a statistically significant improvement in PFS for patients randomized to ENSACOVE compared to patients randomized to crizotinib. The efficacy results as assessed by BICR are summarized in Table 6 and Figure 1.
Table 6. Efficacy Results for eXALT3 Study According to BICR Assessment:
| Efficacy Parameter | ENSACOVE N=143 | Crizotinib N=147 |
|---|---|---|
| Progression-free survival | ||
| Number of events, n (%) | 59 (41%) | 80 (54%) |
| Progressive disease, n (%) | 51 (36%) | 77 (52%) |
| Death, n (%) | 8 (6%) | 3 (2%) |
| Median, months (95% Cl) | 25.8 (21.8, NE) | 12.7 (9.2, 16.6) |
| Hazard ratio (95% Cl) | 0.56 (0.40, 0.79) | |
| p-value a | 0.0007 | |
| Overall response rate | ||
| Overall response rate % (95% Cl) | 74% (66, 81) | 67% (58, 74) |
| Complete response % | 12% | 5% |
| Partial response % | 62% | 61% |
| Duration of response | ||
| Number of responders, n | 106 | 98 |
| Median, months (95% Cl) | NE (22.0, NE) | 27.3 (12.9, NE) |
CI = Confidence Interval, NE=not estimable, BICR = Blinded Independent Central Review
a p-value based on unstratified log-rank test
Figure 1. Kaplan-Meier Plot of Progression-Free Survival by IRR from Study 301 (eXALT3):
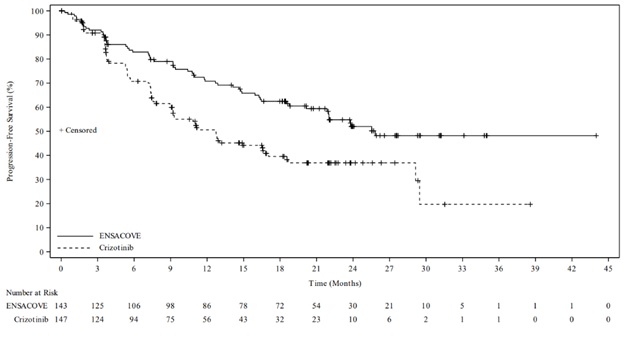
At the time of the primary PFS analysis, OS results were immature. At the time of final analysis of OS, there was no statistically significant difference (p-value = 0.4570) between ENSACOVE and crizotinib. Median OS was 63.2 months in the ENSACOVE arm and 55.7 months in the crizotinib arm, with the hazard ratio of 0.88 (95% CI: 0.63, 1.23).
The results of the pre-specified analyses of CNS response rate by BICR in patients with baseline measurable CNS disease are summarized in Table 7.
Table 7. IRR-assessed CNS Responses in Patients with Measurable CNS Disease at Baseline in Study 301 (eXALT3):
| Efficacy Parameter | ENSACOVE N=17 | Crizotinib N=24 |
|---|---|---|
| CNS overall response rate % (95% Cl) | 59% (33, 82) | 21% (7, 42) |
| Complete response % | 24% | 8% |
| Partial response % | 35% | 13% |
| Duration of Response | ||
| Number of responders, n | 10 | 5 |
| Patients with DOR ≥12 months | 30% | 40% |
BICR = Blinded Independent Central Review; CI = Confidence Interval
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.