EPIDIOLEX Oral solution Ref.[10063] Active ingredients: Cannabidiol
Source: FDA, National Drug Code (US) Revision Year: 2023
12.1. Mechanism of Action
The precise mechanisms by which EPIDIOLEX exerts its anticonvulsant effect in humans are unknown. Cannabidiol does not appear to exert its anticonvulsant effects through interaction with cannabinoid receptors.
12.2. Pharmacodynamics
There are no relevant data on the pharmacodynamic effects of cannabidiol.
12.3. Pharmacokinetics
Cannabidiol demonstrated an increase in exposure that was less than dose-proportional over the range of 5 to 25 mg/kg/day in patients.
Absorption
Cannabidiol has a time to maximum plasma concentration (Tmax) of 2.5 to 5 hours at steady state (Css).
Effect of Food
Coadministration of EPIDIOLEX (750 or 1500 mg) with a high-fat/high-calorie meal increased Cmax by 5‑fold, AUC by 4‑fold, and reduced the total variability, compared with the fasted state in healthy volunteers [see Dosage and Administration (2.4)]. Coadministration of EPIDIOLEX with a low-fat/low-calorie meal increased Cmax and AUC by 4-fold and 3-fold, respectively. Furthermore, coadministration of EPIDIOLEX with bovine milk increased exposure by approximately 3-fold for Cmax and 2.5‑fold for AUC. Coadministration of EPIDIOLEX with alcohol also caused increased exposure to cannabidiol, with 93% increased Cmaxand 63% greater AUC.
Distribution
The apparent volume of distribution in healthy volunteers was 20963 L to 42849 L. Protein binding of the cannabidiol and its metabolites was >94% in vitro.
Elimination
The half-life of cannabidiol in plasma was 56 to 61 hours after twice-daily dosing for 7 days in healthy volunteers. The plasma clearance of cannabidiol following a single EPIDIOLEX 1500 mg dose (approximately equal to the 20 mg/kg/day dosage) is 1111 L/h.
Metabolism
Cannabidiol is metabolized in the liver and the gut (primarily in the liver) by CYP2C19 and CYP3A4 enzymes, and UGT1A7, UGT1A9, and UGT2B7 isoforms.
After repeat dosing, the active metabolite of cannabidiol, 7-OH-CBD, has a 38% lower AUC than the parent drug. The 7-OH-CBD metabolite is converted to 7‑COOH-CBD, which has an approximately 40‑fold higher AUC than the parent drug. Based on preclinical models of seizure, the 7-OH-CBD metabolite is active; however, the 7‑COOH-CBD metabolite is not active.
Excretion
EPIDIOLEX is excreted in feces, with minor renal clearance.
Specific Populations
Patients with Hepatic Impairment
No effects on the exposures of cannabidiol or metabolite exposures were observed following administration of a single dose of EPIDIOLEX 200 mg in patients with mild (Child-Pugh A) hepatic impairment. Patients with moderate (Child-Pugh B) or severe (Child-Pugh C) hepatic impairment had an approximately 2.5 to 5.2-fold higher AUC, compared with healthy volunteers with normal hepatic function [see Dosage and Administration (2.6), Warnings and Precautions (5.1), Use in Specific Populations (8.6)].
Drug Interaction Studies
In Vitro Assessment of Drug Interactions
Drug Metabolizing Enzymes [see Drug Interactions (7.1, 7.2)]:
Cannabidiol is a substrate for CYP3A4 and CYP2C19. Cannabidiol has the potential to inhibit CYP1A2, CYP2B6, CYP2C8, CYP2C9, and CYP2C19 at clinically relevant concentrations.
Cannabidiol may induce or inhibit CYP2B6 at clinically relevant concentrations.
Cannabidiol inhibits uridine 5'-diphospho-glucuronosyltransferase (UGT) enzymes UGT1A9 and UGT2B7, but does not inhibit the UGT1A1, UGT1A3, UGT1A4, UGT1A6, or UGT2B17 isoforms.
Transporters:
Cannabidiol and the cannabidiol metabolite, 7-OH-CBD, are not anticipated to interact with BCRP, BSEP, MDR1/P-gp, OAT1, OAT3, OCT1, OCT2, MATE1, MATE2-K, OATP1B1, or OATP1B3. The cannabidiol metabolite, 7-COOH-CBD, is not a substrate of BCRP, OATP1B1, OATP1B3, or OCT1. However, 7-COOH-CBD is a substrate for P-gp. 7-COOH-CBD is an inhibitor of transport mediated via BCRP and BSEP at clinically relevant concentrations.
In Vivo Assessment of Drug Interactions
Drug Interaction Studies with AEDs:
Clobazam and Valproate:
The interaction potential with other AEDs (clobazam and valproate) was evaluated in dedicated clinical studies following coadministration of EPIDIOLEX (750 mg twice daily in healthy volunteers and 20 mg/kg/day in patients).
Coadministration with clobazam in healthy volunteers increased the cannabidiol active metabolite 7-OH-CBD mean Cmax by 73% and AUC by 47%; and increased the clobazam active metabolite, N-desmethylclobazam, Cmax and AUC by approximately 3-fold, with no effect on clobazam levels [see Drug Interactions (7.2)].
When EPIDIOLEX was coadministered with valproate in a healthy-volunteer trial, there was no effect on the systemic exposure to valproate. In a separate study in epilepsy patients investigating the effect of EPIDIOLEX on valproate exposure, there were decreases in both the plasma Cmax and AUC of valproate, which were not clinically relevant (approximately 17% and 21%, respectively), and a decrease in exposure of the putative hepatotoxic metabolite of valproate, 2-propyl-4-pentenoic acid (approximately 28% and 33%, respectively).
In the healthy-volunteer trial, coadministration with valproate resulted in no clinically relevant changes in exposure to cannabidiol or its major metabolites (cannabidiol Cmax decreased by 26%; 6-OH-CBD AUC increased by 27%; 7-OH-CBD AUC increased by 22%; 7-COOH-CBD Cmax and AUC increased by 25% and 32%, respectively).
Effect of EPIDIOLEX on Midazolam:
Coadministration of EPIDIOLEX with midazolam (a sensitive CYP3A4 substrate) did not result in changes in plasma concentrations of midazolam compared to midazolam administered alone.
Effect of EPIDIOLEX on Stiripentol:
When EPIDIOLEX was coadministered with stiripentol in a healthy volunteer trial, Cmax and AUC of stiripentol increased 28% and 55%, respectively. In patients with epilepsy, Cmax and AUC of stiripentol increased 17% and 30%, respectively [see Drug Interactions (7.2)].
Effect of EPIDIOLEX on Caffeine:
In vivo data from steady-state dosing with cannabidiol (750 mg twice daily) when coadministered with a single dose of caffeine (200 mg), a sensitive CYP1A2 substrate, showed increased caffeine exposure by 15% for Cmax and 95% for AUC compared to when caffeine was administered alone [see Drug Interactions (7.2)].
Effect of CYP3A4 and CYP2C19 Inducers and Inhibitors Coadministered with EPIDIOLEX on Exposure to Cannabidiol:
Coadministration of EPIDIOLEX with potent inhibitors of CYP3A4 and CYP2C19 had the following effects on exposure to cannabidiol and its metabolites. The potent CYP3A4 inhibitor, itraconazole, increased exposure by <10% for cannabidiol and <20% for 7-OH-CBD and 7-COOH-CBD for both AUC and Cmax. Although the effects of the potent CYP2C19 inhibitor fluconazole were slightly more marked, they are still considered not to be clinically meaningful (cannabidiol increased by 22% and 24% for AUC and Cmax, respectively; 7-OH-CBD decreased by 28% and 41% for AUC and Cmax; 7-COOH-CBD decreased by 33% and 48% for AUC and Cmax).
Coadministration with the potent CYP3A4 and CYP2C19 inducing agent rifampin caused a decrease in cannabidiol exposure of 32% and 34% for AUC and Cmax [see Drug Interactions (7.1)]. There were moderate changes in exposure to the active metabolite (7-OH-CBD decreased by 63% and 67% for AUC and Cmax, 7‑COOH‑CBD decreased by 48% for AUC, whereas there was no change in Cmax).
Effect of EPIDIOLEX on Everolimus:
Coadministration of EPIDIOLEX (12.5 mg/kg twice daily) with the P-gp and CYP3A4 substrate everolimus (5 mg) in healthy volunteers led to an approximately 2.5-fold increase in everolimus mean Cmax and AUC [see Drug Interactions (7.2)].
13.1. Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
In a carcinogenicity study in mice, oral administration of cannabidiol (0 [water], 0 [vehicle], 30, 100, or 300 mg/kg/day) for 2 years resulted in an increased incidence of hepatocellular adenomas in male mice at the highest dose tested. At the mid dose (100 mg/kg/day), plasma exposures (AUC) were approximately 5 and 3 times that at the recommended human doses (RHDs) of 20 and 25 mg/kg/day, respectively.
The carcinogenic potential of cannabidiol has not been assessed in rats.
Mutagenesis
Cannabidiol was negative for genotoxicity in in vitro (Ames) and in vivo (rat Comet and bone marrow micronucleus) assays.
Impairment of Fertility
Oral administration of cannabidiol (0, 75, 150, or 250 mg/kg/day) to male and female rats, prior to and throughout mating and continuing in females during early gestation, produced no adverse effects on fertility. The highest dose tested was associated with plasma exposures (AUC) approximately 60 and 34 times that in humans at the RHDs of 20 and 25 mg/kg/day, respectively.
14. Clinical Studies
14.1 Lennox-Gastaut Syndrome
The effectiveness of EPIDIOLEX for the treatment of seizures associated with LGS was established in two randomized, double-blind, placebo-controlled trials in patients aged 2 to 55 years (Study 1, NCT02224690; and Study 2, NCT02224560).
Study 1 (N=171) compared a dose of EPIDIOLEX 20 mg/kg/day with placebo. Study 2 (N=225) compared a 10 mg/kg/day dose and a 20 mg/kg/day dose of EPIDIOLEX with placebo. In both studies, patients had a diagnosis of LGS and were inadequately controlled on at least one AED, with or without vagal nerve stimulation and/or ketogenic diet. Both trials had a 4-week baseline period, during which patients were required to have a minimum of 8 drop seizures (≥2 drop seizures per week). The baseline period was followed by a 2-week titration period and a 12-week maintenance period.
In Study 1, 94% of patients were taking at least 2 concomitant AEDs. The most frequently used concomitant AEDs (greater than 25%) in Study 1 were clobazam (49%), valproate (40%), lamotrigine (37%), levetiracetam (34%), and rufinamide (27%). In Study 2, 94% of patients were taking at least 2 concomitant AEDs. The most frequently used concomitant AEDs (greater than 25%) in Study 2, were clobazam (49%), valproate (38%), levetiracetam (31%), lamotrigine (30%), and rufinamide (29%).
The primary efficacy measure in both studies was the percent change from baseline in the frequency (per 28 days) of drop seizures (atonic, tonic, or tonic-clonic seizures) over the 14-week treatment period. Key secondary endpoints in both studies included analyses of change in total seizure frequency and changes from baseline in the Subject/Caregiver Global Impression of Change (S/CGIC) score at the last visit. For the S/CGIC, the following question was rated on a 7-point scale: "Since [you/your child] started treatment, please assess the status of [your/your child's] overall condition (comparing [your/their] condition now to [your/their] condition before treatment) using the scale below. "The 7-point scale was as follows: "Very Much Improved" (1); "Much Improved" (2); "Slightly Improved" (3); "No Change" (4); "Slightly Worse" (5); "Much Worse" (6); "Very Much Worse" (7).
In Studies 1 and 2, the median percent change from baseline (reduction) in the frequency of drop seizures was significantly greater for both dosage groups of EPIDIOLEX than for placebo (Table 5). A reduction in drop seizures was observed within 4 weeks of initiating treatment with EPIDIOLEX, and the effect remained generally consistent over the 14-week treatment period.
Table 5. Change in Drop Seizure Frequency in Lennox-Gastaut Syndrome during the Treatment Period (Studies 1 and 2):
| Drop Seizure Frequency (per 28 Days) | Placebo | EPIDIOLEX 10 mg/kg/day | EPIDIOLEX 20 mg/kg/day |
|---|---|---|---|
| Study 1 | N=85 | - | N=86 |
| Baseline Period Median Seizure Frequency | 75 | - | 71 |
| Median Percentage Change from Baseline During Treatment | -22 | - | -44 |
| p-value compared to placeboa | 0.01 | ||
| Study 2 | N=76 | N=73 | N=76 |
| Baseline Period Median Seizure Frequency | 80 | 87 | 86 |
| Median Percentage Change from Baseline During Treatment | -17 | -37 | -42 |
| p-value compared to placeboa | <0.01 | <0.01 |
a Obtained from a Wilcoxon rank-sum test.
Figure 1 displays the percentage of patients by category of reduction from baseline in drop seizure frequency per 28 days during the treatment period in Study 1.
Figure 1. Proportion of Patients by Category of Seizure Respons e for EPIDIOLEX and Placebo in Patients with Lennox–Gastaut Syndrome (Study 1):
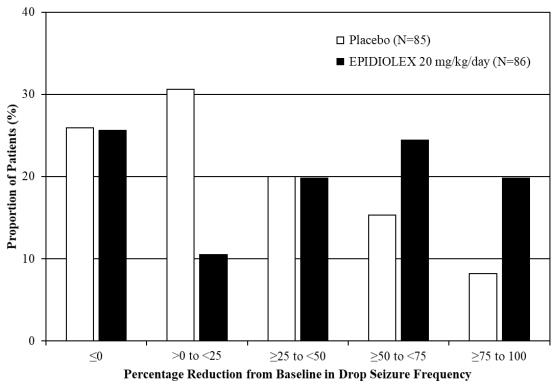
Figure 2 displays the percentage of patients by category of reduction from baseline in drop seizure frequency (per 28 days) during the treatment period in Study 2.
Figure 2. Proportion of Patients by Category of Seizure Respons e for EPIDIOLEX and Placebo in Patients with Lennox-Gastaut Syndrome (Study 2):
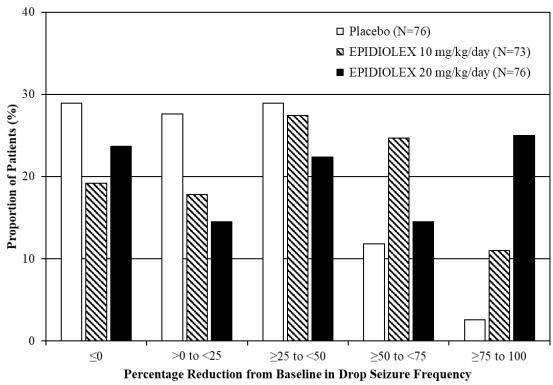
In Study 1, 3 of 85 (4%) patients in the EPIDIOLEX 20 mg/kg/day group reported no drop seizures during the maintenance period, compared to 0 patients in the placebo group. In Study 2, 3 of 73 (4%) patients in the EPIDIOLEX 10 mg/kg/day group, 5 of 76 (7%) patients in the EPIDIOLEX 20 mg/kg/day group, and 1 of 76 (1%) patients in the placebo group reported no drop seizures during the maintenance period.
In LGS patients, EPIDIOLEX was associated with significant reductions in total seizure frequency (drop and non-drop seizures) versus placebo. During the treatment period in Study 1, the median percent reduction in total seizure frequency (per 28 days) was 41% in patients taking EPIDIOLEX 20 mg/kg/day compared to 14% in patients taking placebo (p<0.01). In Study 2, the median percent reduction in total seizure frequency (per 28 days) was 36% in the 10 mg/kg/day group, 38% in the 20 mg/kg/day group, and 18% in the placebo group (p<0.01 for both groups).
A greater improvement on the Subject/Caregiver Global Impression of Change (S/CGIC) was reported in patients treated with EPIDIOLEX compared with placebo in Studies 1 and 2. In Study 1, the mean S/CGIC score at last visit was 3.0 in the 20 mg/kg/day EPIDIOLEX group (corresponding to "slightly improved") compared with 3.7 (most closely associated with "no change") in the placebo group (p<0.01). In Study 2, the mean S/CGIC score at last visit was 3.0 and 3.2 in the 10 mg/kg/day and 20 mg/kg/day EPIDIOLEX groups, respectively ("slightly improved"), compared with 3.6 ("no change") in the placebo group (p<0.01 and p=0.04, respectively).
14.2 Dravet Syndrome
The effectiveness of EPIDIOLEX for the treatment of seizures associated with DS was demonstrated in a single randomized, double-blind, placebo-controlled trial in 120 patients aged 2 to 18 years (Study 3, NCT02091375). Study 3 compared a dose of EPIDIOLEX 20 mg/kg/day with placebo. Patients had a diagnosis of treatment-resistant DS and were inadequately controlled with at least 1 concomitant AED, with or without vagal nerve stimulation or ketogenic diet. During the 4-week baseline period, patients were required to have at least 4 convulsive seizures while on stable AED therapy. The baseline period was followed by a 2-week titration period and a 12-week maintenance period. The primary efficacy measure was the percent change from baseline in the frequency (per 28 days) of convulsive seizures (all countable atonic, tonic, clonic, and tonic-clonic seizures) over the 14-week treatment period.
In Study 3, 93% of patients were taking at least 2 concomitant AEDs during the trial. The most commonly used concomitant AEDs (greater than 25%) in Study 3 were clobazam (65%), valproate (57%), stiripentol (43%), levetiracetam (28%), and topiramate (26%).
The median percent change from baseline (reduction) in the frequency of convulsive seizures was significantly greater for EPIDIOLEX 20 mg/kg/day than for placebo (Table 6). A reduction in convulsive seizures was observed within 4 weeks of initiating treatment with EPIDIOLEX and the effect remained generally consistent over the 14-week treatment period.
Table 6. Change in Convulsive Seizure Frequency in Dravet Syndrome during the Treatment Period (Study 3):
| Total Convulsive Seizures (per 28 Days) | Placebo | EPIDIOLEX 20 mg/kg/day |
|---|---|---|
| Study 3 | N=59 | N=61 |
| Baseline Period Median Seizure Frequency | 15 | 12 |
| Median Percentage Change from Baseline During Treatment | -13 | -39 |
| p-value compared to placeboa | 0.01 |
a Obtained from Wilcoxon rank-sum test.
Figure 3 displays the percentage of patients by category of reduction from baseline in convulsive seizure frequency (per 28 days) during the treatment period in Study 3.
Figure 3. Proportion of Patients by Category of Seizure Respons e for EPIDIOLEX and Placebo in Patients with Dravet Syndrome (Study 3):
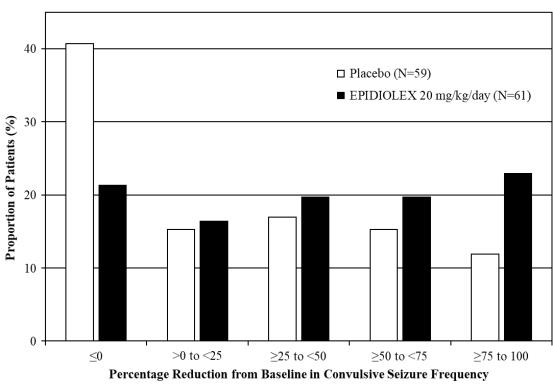
In Study 3, 4 of 60 (7%) patients treated with EPIDIOLEX 20 mg/kg/day reported no convulsive seizures during the maintenance period, compared to 0 patients in the placebo group.
14.3 Tuberous Sclerosis Complex
The effectiveness of EPIDIOLEX for the treatment of seizures associated with TSC was demonstrated in a randomized, double-blind, placebo-controlled trial in 224 patients aged 1 to 65 years (Study 4; NCT02544763).
Study 4 (N=224) compared doses of EPIDIOLEX 25 mg/kg/day and 50 mg/kg/day (2 times the recommended maintenance dosage) with placebo. Patients had a diagnosis of TSC and seizures inadequately controlled with at least one concomitant AED, with or without vagal nerve stimulation or ketogenic diet. During the 4-week baseline period, patients had at least 8 seizures, with at least 1 seizure occurring in at least 3 of the 4 weeks (focal motor seizures without impairment of consciousness or awareness; focal seizures with impairment of consciousness or awareness; focal seizures evolving to bilateral generalized convulsive seizures and generalized seizures [tonic–clonic, tonic, clonic or atonic seizures]). The baseline period was followed by a 4-week titration period and a 12‑week maintenance period.
In Study 4, all patients but 1 (in EPIDIOLEX 25 mg/kg/day group) were taking 1-5 concomitant AEDs during the trial. The most commonly used concomitant AEDs (greater than 25%) were valproate (45%), vigabatrin (33%), levetiracetam (29%), and clobazam (27%). The baseline median TSC-associated seizure frequency was 57 per 28 days for the combined groups. The primary efficacy measure was the change in seizure frequency of TSC-associated seizures over the 16-week treatment period compared with baseline.
In Study 4, the percentage change from baseline (reduction) in the frequency of TSC-associated seizures was significantly greater for patients treated with EPIDIOLEX than for placebo (Table 7). A reduction in TSC-associated seizures was observed within 4 weeks of initiating treatment with EPIDIOLEX and the effect remained generally consistent over the 12-week maintenance period.
Table 7. Change in TSC-Associated Seizure Frequency during the Treatment Period (Study 4):
| Total TSC-Associated Seizures (per 28 Days) | Placebo | EPIDIOLEX 25 mg/kg/day |
|---|---|---|
| Study 4 | N=76 | N=75 |
| Baseline Period Median Seizure Frequency | 54 | 56 |
| Median Percentage Change from Baseline During Treatment | -20 | -43 |
| p-value compared to placeboa | <0.01 | |
| Percentage Change from Baseline During Treatment in Estimated Mean Seizure Frequencyb | -24 | -48 |
| p-value compared to placebob | <0.01 |
a Obtained from a Wilcoxon rank-sum test.
b Obtained from log-transformed ANCOVA.
Figure 4 displays the percentage of patients by category of reduction from baseline in TSC-associated seizure frequency (per 28 days) during the treatment period in Study 4.
Figure 4. Proportion of Patients by Category of Seizure Response for EPIDIOLEX and Placebo in Patients with Tuberous Sclerosis Complex (Study 4):
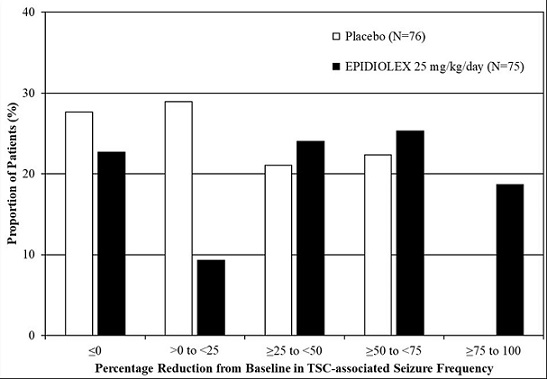
In Study 4, 4 of 75 (5%) patients treated with EPIDIOLEX 25 mg/kg/day reported no TSC-associated seizures during the maintenance period, compared to 0 patients in the placebo group.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.