ERIVEDGE Hard capsule Ref.[9090] Active ingredients: Vismodegib
Source: European Medicines Agency (EU) Revision Year: 2025 Publisher: Roche Registration GmbH, Emil-Barell-Strasse 1, 79639, Grenzach-Wyhlen, Germany
Pharmacodynamic properties
Pharmacotherapeutic group: Antineoplastic agents, other antineoplastic agents
ATC code: L01XJ01
Mechanism of action
Vismodegib is an orally available small-molecule inhibitor of the Hedgehog pathway. Hedgehog pathway signalling through the Smoothened transmembrane protein (SMO) leads to the activation and nuclear localisation of Glioma-Associated Oncogene (GLI) transcription factors and induction of Hedgehog target genes. Many of these genes are involved in proliferation, survival, and differentiation. Vismodegib binds to and inhibits the SMO protein thereby blocking Hedgehog signal transduction.
Clinical efficacy and safety
The pivotal trial, ERIVANCE BCC (SHH4476g), was an international, single-arm, multi-centre, 2-cohort study. Metastatic BCC was defined as BCC that had spread beyond the skin to other parts of the body, including the lymph nodes, lung, bones and/or internal organs. LaBCC patients had cutaneous lesions that were inappropriate for surgery (inoperable, multiply recurrent where curative resection deemed to be unlikely or for whom surgery would result in substantial deformity or morbidity) and for which radiotherapy was unsuccessful or contraindicated or inappropriate. Prior to study enrolment, diagnosis of BCC was confirmed by histology. Patients with Gorlin syndrome who had at least one aBCC lesion and met inclusion criteria were eligible to participate in the study. Patients were treated with oral daily dosing of Erivedge at 150 mg.
The median age of the efficacy evaluable population was 62 years (46% were at least 65 years old), 61% male and 100% White. For the mBCC cohort, 97% of patients had prior therapy including surgery (97%), radiotherapy (58%), and systemic therapies (30%). For the laBCC cohort (n=63), 94% of patients had prior therapies including surgery (89%), radiotherapy (27%), and systemic/topical therapies (11%). The median duration of treatment was 12.9 months (range 0.7 to 47.8 months).
The primary endpoint was objective response rate (ORR) as assessed by an independent review facility (IRF) as summarised in Table 2. Objective response was defined as a complete or partial response determined on two consecutive assessments separated by at least 4 weeks. In the mBCC cohort, tumour response was assessed according to the Response Evaluation Criteria in Solid Tumours (RECIST) version 1.0. In the laBCC cohort, tumour response was assessed based on visual assessment of external tumour and ulceration, tumour imaging (where appropriate), and tumour biopsy. A patient was considered a responder in the laBCC cohort if at least one of the following criteria was met and the patient did not experience progression: (1) ≥30% reduction in lesion size [sum of the longest diameter (SLD)], from baseline in target lesions by radiography; (2) ≥30% reduction in SLD from baseline in externally visible dimension of target lesions; (3) Complete resolution of ulceration in all target lesions. Key data are summarised in Table 2:
Table 2. SHH4476g Erivedge Efficacy Results (IRF 21 months and Investigator assessed 39 months follow-up after last patient enrolled): efficacy-evaluable patients*,†:
| IRF-Assessed | Investigator-Assessed | |||
|---|---|---|---|---|
| mBCC (n=33) | laBCC** (n=63) | mBCC (n=33) | laBCC** (n=63) | |
| Responders | 11 (33.3%) | 30 (47.6%) | 16 (48.5%) | 38 (60.3%) |
| 95% CI for overall response | (19.2%, 51.8%) | (35.5%, 60.6%) | (30.8%, 66.2%) | (47.2%, 71.7%) |
| Complete Response | 0 | 14 (22.2%) | 0 | 20 (31.7%) |
| Partial Response | 11 (33.3%) | 16 (25.4%) | 16 (48.5%) | 18 (28.6%) |
| Stable disease | 20 | 22 | 14 | 15 |
| Progressive disease‡ | 1 | 8 | 2 | 6 |
| Median Duration of Response (months) | 7.6 | 9.5 | 14.8 | 26.2 |
| (95% CI) | (5.5, 9.4) | (7.4, 21.4) | (5.6, 17.0) | (9.0, 37.6) |
| Median Progression Free survival (months) | 9.5 | 9.5 | 9.3 | 12.9 |
| (95% CI) | (7.4,11.1) | (7.4, 14.8) | (7.4, 16.6) | (10.2, 28.0) |
| Median OS, (months) | 33.4 | NE | ||
| (95% CI) | (18.1, NE) | (NE, NE) | ||
| 1-year survival rate | 78.7% | 93.2% | ||
| (95% CI) | (64.7, 92.7) | (86.8, 99.6) | ||
NE = not estimable
* Efficacy-evaluable patient population is defined as all enrolled patients who received any amount of Erivedge and for whom the independent pathologist's interpretation of archival tissue or baseline biopsy was consistent with BCC.
† Unevaluable/missing data included 1 mBCC and 4 laBCC patients.
‡ Progression in laBCC cohort is defined as meeting any of the following criteria: (1) ≥20% increase in the sum of the longest dimensions (SLD) from nadir in target lesions (either by radiography or by externally visible dimension), (2) New ulceration of target lesions persisting without evidence of healing for at least 2 weeks, (3) New lesions by radiography or physical examination, (4) Progression of non-target lesions by RECIST.
** 54% of laBCC patients had no histopathologic evidence of BCC at 24 weeks.
As shown in the waterfall plots in figures 1 and 2, which chart maximum reduction in target lesion(s) size for each patient, the majority of patients in both cohorts experienced tumour shrinkage as assessed by the IRF.
Figure 1. SHH4476g Metastatic BCC Cohort:
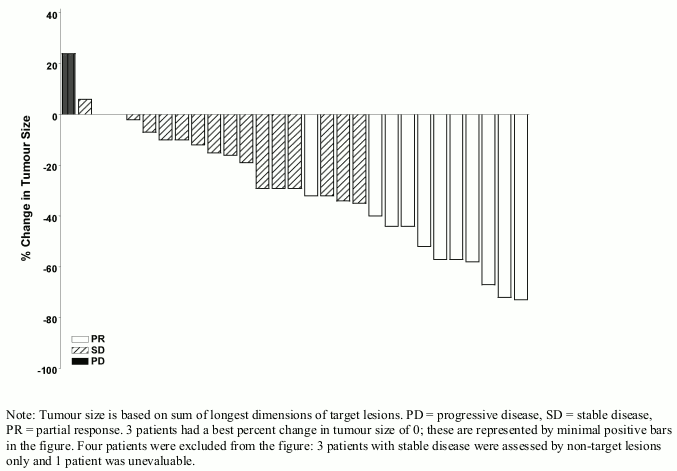
Note: Tumour size is based on sum of longest dimensions of target lesions. PD = progressive disease, SD = stable disease, PR = partial response. 3 patients had a best percent change in tumour size of 0; these are represented by minimal positive bars in the figure. Four patients were excluded from the figure: 3 patients with stable disease were assessed by non-target lesions only and 1 patient was unevaluable.
Figure 2. SHH4476g Locally Advanced BCC Cohort:
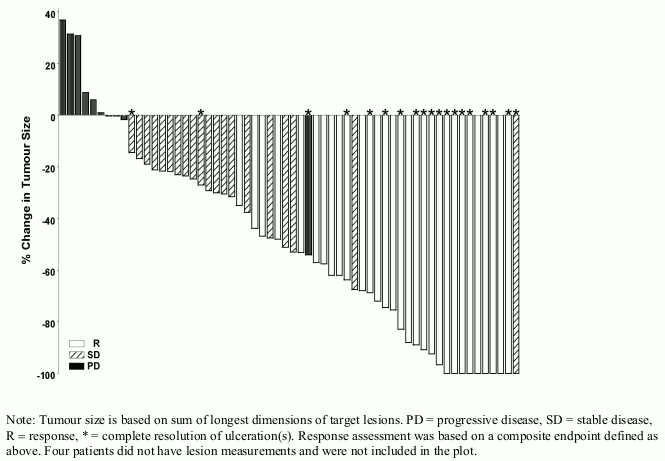
Note: Tumour size is based on sum of longest dimensions of target lesions. PD = progressive disease, SD = stable disease, R = response, * = complete resolution of ulceration(s). Response assessment was based on a composite endpoint defined as above. Four patients did not have lesion measurements and were not included in the plot.
Time to maximum tumour reduction
Among patients who achieved tumour reduction, the median time to maximum tumour reduction occurred in 5.6 and 5.5 months for laBCC and mBCC patients respectively, based on the IRF assessment. According to investigator assessment, the median time to maximum tumour reduction occurred in 6.7 and 5.5 months for laBCC and mBCC patients respectively.
Cardiac electrophysiology
In a thorough QTc study in 60 healthy subjects, there was no effect of therapeutic doses of Erivedge on the QTc interval.
Post approval study results
A post-approval, open-label, non-comparative, multicenter, phase II clinical trial (MO25616) was conducted in 1232 patients with advanced BCC, of whom 1215 patients were evaluable for efficacy and safety with laBCC (n=1119) or mBCC (n=96). LaBCC was defined as cutaneous lesions that were inappropriate for surgery (inoperable, or for whom surgery would result in substantial deformity) and for which radiotherapy was unsuccessful or contraindicated. Metastatic BCC was defined as histologically confirmed distant metastasis. Prior to study enrollment, diagnosis of BCC was confirmed by histology. Patients were treated with oral daily dosing of Erivedge at 150 mg.
The median age for all patients was 72 years. The majority of patients were male (57%); 8% had mBCC whereas 92% had laBCC. For the metastatic cohort, the majority of patients had prior therapies, including surgery (91%), radiotherapy (62%) and systemic therapy (16%). For the locally advanced cohort, the majority of patients had prior therapies, including surgery (85%), radiotherapy (28%) and systemic therapy (7%). The median duration of treatment for all patients was 8.6 months (range 0 to 44.1).
Among patients in the efficacy-evaluable population with measurable and histologically confirmed disease, 68.5% and 36.9% responded to treatment in the laBCC and mBCC cohorts, respectively, by RECIST v1.1. Of patients who had a confirmed response (partial or complete), the median Duration of Response was 23.0 months (95% CI: 20.4, 26.7) in the laBCC cohort and 13.9 months (95% CI: 9.2, NE) in the mBCC cohort. Complete response was achieved in 4.8% patients in the mBCC cohort and 33.4% in the laBCC cohort. Partial response was achieved in 32.1% patients in the mBCC cohort and 35.1% in the laBCC cohort.
Paediatric population
The European Medicines Agency has waived the obligation to submit the results of studies with Erivedge in all subsets of the paediatric population with basal cell carcinoma (see section 4.2 for information on paediatric use).
Pharmacokinetic properties
Absorption
Erivedge is a highly permeable compound with low aqueous solubility (BCS Class 2). The single dose mean (CV %) absolute bioavailability of Erivedge is 31.8 (14.5) %. Absorption is saturable as evidenced by the lack of dose proportional increase in exposure after a single dose of 270 mg and 540 mg Erivedge. Under clinically relevant conditions (steady state), the PK of vismodegib is not affected by food. Therefore, Erivedge may be taken without regard to meals.
Distribution
The volume of distribution for vismodegib is low, ranging from 16.4 to 26.6 L. In vitro binding of vismodegib to human plasma proteins is high (97%) at clinically relevant concentrations. Vismodegib binds to both human serum albumin and alpha-1-acid glycoprotein (AAG). In vitro binding to AAG is saturable at clinically relevant concentrations. Ex vivo plasma protein binding in human patients is >99%. Vismodegib concentrations are strongly correlated with AAG levels, showing parallel fluctuations of AAG and total vismodegib over time and consistently low unbound vismodegib levels.
Biotransformation
Vismodegib is slowly eliminated by a combination of metabolism and excretion of parent drug substance. Vismodegib is predominant in plasma, with concentrations representing greater than 98% of the total circulating concentrations (including associated metabolites). Metabolic pathways of vismodegib in humans include oxidation, glucuronidation, and an uncommon pyridine ring cleavage. CYP2C9 appears to contribute in part to vismodegib metabolism in vivo.
Elimination
After oral administration of a radiolabelled dose, vismodegib is absorbed and slowly eliminated by a combination of metabolism and excretion of parent drug substance, the majority of which is recovered in the faeces (82% of the administered dose), with 4.4% of the administered dose recovered in urine.
Vismodegib and associated metabolic products are eliminated primarily by the hepatic route. After continuous once-daily dosing, the pharmacokinetics of vismodegib appears to be nonlinear due to saturable absorption and saturable protein binding. After a single oral dose, vismodegib has a terminal half-life of ca. 12 days.
The apparent half-life of vismodegib at steady-state is estimated to be 4 days with continuous daily dosing. Upon continuous daily dosing, there is a 3 fold accumulation of vismodegib total plasma concentrations.
Vismodegib inhibits UGT2B7 in vitro and it may not be excluded that inhibition can take place in vivo in the intestine.
Special populations
Elderly
There are limited data in older people. In clinical trials with aBCC, approximately 40% of patients were of geriatric age (≥65 years). Population pharmacokinetic analyses suggest that age did not have a clinically significant impact on steady-state concentration of vismodegib.
Gender
Based on population pharmacokinetic analysis of combined data from 121 males and 104 females, gender did not appear to affect the pharmacokinetics of vismodegib.
Race
There are limited data in non-Caucasian patients. Since the number of subjects who were not Caucasian comprised only <3% of the total population (6 Black, 219 Caucasian), race was not evaluated as a covariate in the population pharmacokinetic analysis.
Renal impairment
Renal excretion of orally administered vismodegib is low. Therefore, mild and moderate renal impairment is unlikely to have a clinically significant effect on the pharmacokinetics of vismodegib. Based on a population PK analysis in patients with mild (BSA-indexed CrCl 50 to 80 mL/min, n=58) and moderate (BSA-indexed CrCl 30 to 50 mL/min, n=16) renal impairment, mild and moderate impaired renal function had no clinically significant effect on the pharmacokinetics of vismodegib (see section 4.2). Very limited data is available in patients with severe renal impairments.
Hepatic impairment
The major elimination pathways of vismodegib involve hepatic metabolism and biliary/intestinal secretion. In a clinical study in patients with hepatic impairment (degree of impairment based on subject's AST and total bilirubin levels) following multiple doses of vismodegib, it was shown that in patients with mild (NCI-ODWG criteria, n=8), moderate (NCI-ODWG criteria, n=6), and severe (NCI-ODWG criteria, n=3) hepatic impairment, the pharmacokinetic profile of vismodegib was comparable to that of subjects with normal hepatic function (n=9) (see section 4.2).
Paediatric population
There are insufficient pharmacokinetic data in paediatric patients.
Preclinical safety data
The preclinical safety profile of Erivedge was assessed in mice, rats, and dogs.
Repeat-dose toxicity
In general, the tolerability of Erivedge in repeat-dose toxicity studies in rats and dogs was limited by nonspecific manifestations of toxicity including decreased body weight gain and food consumption. Additional findings at clinically relevant exposures included faecal changes; skeletal muscle twitching or tremors; alopecia; swelling, follicular hyperkeratosis, and inflammation in paw pads; and increased LDL and HDL cholesterol. Decreased haematocrit or platelet count were observed in some dogs at clinically relevant exposures; however, there was no evidence of a primary effect on bone marrow in affected animals.
Carcinogenicity
Carcinogenicity studies were performed in mice and rats. Carcinogenic potential was identified in rats only and was limited to benign hair follicle tumors, including pilomatricomas and keratoacanthomas respectively at ≥0.1-fold and ≥0.6-fold of the steady-state AUC(0-24h) of the recommended human dose. No malignant tumors were identified in either species tested. Benign hair follicle tumors have not been reported in clinical trials with Erivedge, and the relevance of this finding to humans is uncertain.
Mutagenicity
There was no evidence of genotoxicity in in vitro assays (reverse bacterial mutagenesis [Ames] and human lymphocyte chromosome aberration assays) or in the in vivo rat bone marrow micronucleus assay.
Fertility
In the dedicated 26-week vismodegib rat fertility study, significantly increased absolute weights of seminal vesicles and reduced absolute weights of prostate were observed. In addition, the ratio of organ weight to terminal body weight was significantly increased for epididymis, cauda epididymis, testes and seminal vesicles. In the same study there were no histopathological findings in male reproductive organs and no effects on male fertility endpoints, including percent motile sperm, observed at 100 mg/kg/day at the end of dosing or recovery phase (corresponding to 1.3-fold of the steady-state AUC0-24h at the recommended human dose). In addition, in the vismodegib general toxicity studies up to 26-week in sexually mature rats and dogs, no effects on male reproductive organs were observed. Increased number of degenerating germ cells and hypospermia in sexually immature dogs observed at ≥50 mg/kg/day in the 4-week general toxicity study was of undetermined relationship to vismodegib.
In the dedicated 26-week vismodegib rat fertility study, vismodegib-related effects on female reproductive organs were observed at 100 mg/kg/day immediately after treatment discontinuation, including decreased implantations, increased percent preimplantation loss, and decreased number of dams with viable embryos. Similar findings were not observed after a 16 week recovery period. No correlative histopathologic changes were observed. The exposure in female rats at 100 mg/kg corresponds to 1.2-fold of the steady-state AUC0-24h at the recommended human dose. In addition, in the vismodegib general 26-week toxicity study, decreased number of corpora lutea was observed at 100 mg/kg/day; the effect was not reversed by the end of an 8 week recovery period.
Teratogenicity
In an embryo-foetal development study in which pregnant rats were administered vismodegib daily during organogenesis, vismodegib crossed the placenta and was severely toxic to the conceptus. Malformations, including craniofacial anomalies, open perineum, and absent and/or fused digits, were observed in foetuses of dams at a dose which corresponded to 20% of the typical steady-state exposure in patients, and a 100% incidence of embryolethality was observed at higher doses.
Post-natal development
Dedicated studies to assess the potential of vismodegib to affect post-natal development have not been performed. However, irreversible defects in growing teeth and premature closure of the femoral epiphyseal plate, observed in rat toxicity studies at clinically relevant exposures, represent risks to post-natal development.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.