EXPAREL Suspension for solution for injection Ref.[27449] Active ingredients: Bupivacaine
Source: FDA, National Drug Code (US) Revision Year: 2021
12.1. Mechanism of Action
Local anesthetics block the generation and the conduction of nerve impulses presumably by increasing the threshold for electrical excitation in the nerve, by slowing the propagation of the nerve impulse, and by reducing the rate of rise of the action potential. In general, the progression of anesthesia is related to the diameter, myelination, and conduction velocity of affected nerve fibers. Clinically, the order of loss of nerve function is as follows: (1) pain, (2) temperature, (3) touch, (4) proprioception, and (5) skeletal muscle tone.
12.2. Pharmacodynamics
Systemic absorption of local anesthetics produces effects on the cardiovascular and central nervous systems. At blood concentrations achieved with normal therapeutic doses, changes in cardiac conduction, excitability, refractoriness, contractility, and peripheral vascular resistance are minimal. However, toxic blood concentrations depress cardiac conductivity and excitability, which may lead to atrioventricular block, ventricular arrhythmias, and cardiac arrest, sometimes resulting in fatalities. In addition, myocardial contractility is depressed and peripheral vasodilation occurs, leading to decreased cardiac output and arterial blood pressure. Clinical reports and animal research suggest that these cardiovascular changes are more likely to occur after accidental intravascular injection of bupivacaine.
Following systemic absorption, local anesthetics can produce central nervous system stimulation, depression, or both. Apparent central stimulation is manifested as restlessness, tremors, and shivering progressing to convulsions, followed by depression and coma progressing ultimately to respiratory arrest. However, the local anesthetics have a primary depressant effect on the medulla and on higher centers. The depressed stage may occur without a prior excited state.
12.3. Pharmacokinetics
Administration of EXPAREL results in systemic plasma levels of bupivacaine which can persist for 96 hours after local infiltration and 120 hours after interscalene brachial plexus nerve block. [See Warnings and Precautions (5.2)]. In general, peripheral nerve blocks have shown systemic plasma levels of bupivacaine for extended duration when compared to local infiltration. Systemic plasma levels of bupivacaine following administration of EXPAREL are not correlated with local efficacy.
Absorption
The rate of systemic absorption of bupivacaine is dependent upon the total dose of drug administered, the route of administration, and the vascularity of the administration site.
Pharmacokinetic parameters of EXPAREL after local infiltration and following an interscalene brachial plexus nerve block were evaluated following surgical procedures. Descriptive statistics of pharmacokinetic parameters of representative EXPAREL doses in each study are provided in Table 4 for adult patients after administration of Single Doses of EXPAREL via Local Infiltration and Interscalene Brachial Plexus Nerve Block, and in Table 5 for pediatric patients aged 6 to less than 17 years old after Administration of Single Doses of EXPAREL via Local Infiltration.
Table 4. Summary of Pharmacokinetic Parameters for Bupivacaine after Administration of Single Doses of EXPAREL via Local Infiltration and Interscalene Brachial Plexus Nerve Block in Adult Patients:
| Parameters* | Surgical Site Administration via Local Infiltration | Interscalene Brachial Plexus Nerve Block | |||
|---|---|---|---|---|---|
| Bunionectomy 106 mg (8 mL) | Hemorrhoidectomy 266 mg (20 mL) | Spine Surgery1 266 mg | Cardiac Surgery2 266 mg | Total Shoulder Arthroplasty 133 mg (10 mL) | |
| (N=26) | (N=25) | (N=11) | (N=5) | (N=12) | |
| Cmax (ng/mL) | 166 (93) | 867 (353) | 513 (268) | 445 (120) | 207 (137) |
| Tmax (h) | 2 (0.5, 24) | 0.5 (0.25, 36) | 0.6 (0.2, 37) | 0.6 (0.6, 36) | 48 (3,74) |
| AUC0-40h (h x ng/mL) | NE | NE | 13035 (8782) | 9867 (1332) | NE |
| AUC(0-last) (h x ng/mL) | 5864 (2038)3 | 16867 (7868)3 | 17214 (11621)4 | 14277 (3449)3 | 11484 (8615)5 |
| AUC(inf) (h x ng/mL) | 7105 (2283) | 18289 (7569) | 17917 (12187) | 15768 (4530) | 11590 (8603) |
| t½ (h) | 34 (17) | 24 (39) | 9 (2) | 14 (6) | 11 (5) |
* Arithmetic mean (standard deviation) except Tmax where it is median (minimum, maximum).
1 Subjects undergoing open posterior spinal fusion or reconstructive surgery
2 Subjects undergoing posterolateral thoracotomy
3 AUC0-last, 0-72h ; 4AUC0-last, 0-96h ; 5AUC0-last, 0-120h
NE: Not evaluated
Table 5. Summary of Pharmacokinetic Parameters for Bupivacaine after Administration of Single Doses of EXPAREL via Local Infiltration in Pediatric Patients Aged 6 to Less Than 17 Years Old:
| Parameters* | Spine Surgery | Cardiac Surgery |
|---|---|---|
| EXPAREL 4 mg/kg (Maximum 266 mg) | EXPAREL 4 mg/kg (Maximum 266 mg) | |
| 6 to <17 years (N=17) | 6 to <12 years (N=21) | |
| Cmax (ng/mL) | 353 (125) | 447 (243) |
| Tmax (h) | 1.2 (0.3-26) | 23 (0.2, 55) |
| AUC(0-40 h) (h x ng/mL) | 8782 (2834) | 11286 (4791) |
| AUC(0-last) (h x ng/mL) | NR1 | 16776 (7936)1 |
| AUC(inf) (h x ng/mL) | NR2 | NR2 |
| t½ (h) | NR2 | NR2 |
Arithmetic mean (standard deviation) except Tmax where it is median (minimum, maximum).
1 AUC0-last, 0-72h
NR1 = Not reported, since the last sampling time point varies among different patients.
NR2 = Not reported, since the terminal elimination phase was not adequately characterized in sufficient number of patients.
Distribution
After bupivacaine has been released from EXPAREL and is absorbed systemically, bupivacaine distribution is expected to be the same as for any bupivacaine HCl solution formulation.
Local anesthetics including bupivacaine are distributed to some extent to all body tissues, with high concentrations found in highly perfused organs such as the liver, lungs, heart, and brain.
Local anesthetics including bupivacaine appear to cross the placenta by passive diffusion. The rate and degree of diffusion is governed by (1) the degree of plasma protein binding, (2) the degree of ionization, and (3) the degree of lipid solubility. Fetal/maternal ratios of local anesthetics appear to be inversely related to the degree of plasma protein binding, because only the free, unbound drug is available for placental transfer. Bupivacaine with a high protein binding capacity (95%) has a low fetal/maternal ratio (0.2 to 0.4). The extent of placental transfer is also determined by the degree of ionization and lipid solubility of the drug. Lipid soluble, non-ionized drugs such as bupivacaine readily enter the fetal blood from the maternal circulation.
Elimination
Metabolism
Amide-type local anesthetics, such as bupivacaine, are metabolized primarily in the liver via conjugation with glucuronic acid. Pipecoloxylidide (PPX) is the major metabolite of bupivacaine; approximately 5% of bupivacaine is converted to PPX. Elimination of drug depends largely upon the availability of plasma protein binding sites in the circulation to carry it to the liver where it is metabolized.
Various pharmacokinetic parameters of the local anesthetics can be significantly altered by the presence of hepatic disease. Patients with hepatic disease, especially those with severe hepatic disease, may be more susceptible to the potential toxicities of the amide-type local anesthetics.
Excretion
After bupivacaine has been released from EXPAREL and is absorbed systemically, bupivacaine excretion is expected to be the same as for other bupivacaine formulations.
The kidney is the main excretory organ for most local anesthetics and their metabolites. Only 6% of bupivacaine is excreted unchanged in the urine.
Urinary excretion is affected by urinary perfusion and factors affecting urinary pH. Acidifying the urine hastens the renal elimination of local anesthetics. Various pharmacokinetic parameters of the local anesthetics can be significantly altered by the presence of renal disease, factors affecting urinary pH, and renal blood flow.
Specific Populations
Hepatic Impairment
Because amide-type local anesthetics, such as bupivacaine, are metabolized by the liver, the effects of decreased hepatic function on bupivacaine pharmacokinetics following administration of EXPAREL were studied in patients with moderate hepatic impairment. Consistent with the hepatic clearance of bupivacaine, mean plasma concentrations were higher in patients with moderate hepatic impairment than in the healthy control volunteers with approximately 1.5- and 1.6-fold increases in the mean values for Cmax and the area under the curve (AUC), respectively. [See Warnings and Precautions (5.1) and Use in Specific Populations (8.6)].
13.1. Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
Long-term studies in animals to evaluate the carcinogenic potential of bupivacaine have not been conducted.
Mutagenesis
The mutagenic potential of bupivacaine has not been determined.
Impairment of Fertility
The effect of bupivacaine on fertility has not been determined.
14. Clinical Studies
14.1 Studies Confirming Efficacy
The efficacy of EXPAREL compared to placebo was demonstrated in three multicenter, randomized, double-blinded clinical studies. For local analgesia via infiltration, one study evaluated the treatment in patients undergoing bunionectomy; the other study evaluated the treatment in patients undergoing hemorrhoidectomy. For regional analgesia, one study evaluated the use of EXPAREL as a brachial plexus nerve block via interscalene or supraclavicular approach in patients undergoing total shoulder arthroplasty (TSA) or rotator cuff repair (RCR), however, only two subjects had nerve blocks via the supraclavicular approach. Three additional studies did not provide sufficient efficacy and/or safety data to support a nerve block indication: two studies evaluated the use of EXPAREL via femoral block in patients undergoing total knee arthroplasty (TKA), and one study evaluated the use of EXPAREL via intercostal nerve block for patients undergoing posterolateral thoracotomy.
Study 1: Infiltration for Bunionectomy
A multicenter, randomized, double-blind, placebo-controlled, parallel-group clinical trial (NCT00890682) evaluated the safety and efficacy of 106 mg (8 mL) EXPAREL in 193 patients undergoing bunionectomy. The mean age was 43 years (range 18 to 72).
Study medication was administered directly into the site at the conclusion of the surgery, prior to closure. There was an infiltration of 7 mL of EXPAREL into the tissues surrounding the osteotomy and 1 mL into the subcutaneous tissue.
Pain intensity was rated by the patients on a 0 to 10 numeric rating scale (NRS) out to 72 hours. Postoperatively, patients were allowed rescue medication (5 mg oxycodone/325 mg acetaminophen orally every 4 to 6 hours as needed) or, if that was insufficient within the first 24 hours, ketorolac (15 to 30 mg IV). The primary outcome measure was the area under the curve (AUC) of the NRS pain intensity scores (cumulative pain scores) collected over the first 24-hour period. There was a significant treatment effect for EXPAREL compared to placebo. EXPAREL demonstrated a significant reduction in pain intensity compared to placebo for up to 24 hours. There was no significant difference in the amount of morphine equivalents used through 72 hours post-surgery, 43 mg versus 42 mg for placebo and EXPAREL, respectively. In addition, there was not a significant difference in the percentage of patients that used ketorolac, 43% versus 31% for placebo and EXPAREL, respectively.
Study 2: Infiltration for Hemorrhoidectomy
A multicenter, randomized, double-blind, placebo-controlled, parallel-group clinical trial (NCT00890721) evaluated the safety and efficacy of 266 mg (20 mL) EXPAREL in 189 patients undergoing hemorrhoidectomy. The mean age was 48 years (range 18 to 86).
Study medication was administered directly into the site (greater than or equal to 3 cm) at the conclusion of the surgery. Dilution of 20 mL of EXPAREL with 10 mL of saline, for a total of 30 mL, was divided into six 5-mL aliquots. A field block was performed by visualizing the anal sphincter as a clock face and slowly infiltrating one aliquot to each of the even numbers.
Pain intensity was rated by the patients on a 0 to 10 NRS at multiple time points up to 72 hours. Postoperatively, patients were allowed rescue medication (morphine sulfate 10 mg intramuscular every 4 hours as needed).
The primary outcome measure was the AUC of the NRS pain intensity scores (cumulative pain scores) collected over the first 72-hour period.
There was a significant treatment effect for EXPAREL compared to placebo. See Figure 1 for the mean pain intensity over time for the EXPAREL and placebo treatment groups for the 72-hour efficacy period.
Figure 1. Mean Pain Intensity versus Time plot for hemorrhoidectomy study (C-316):
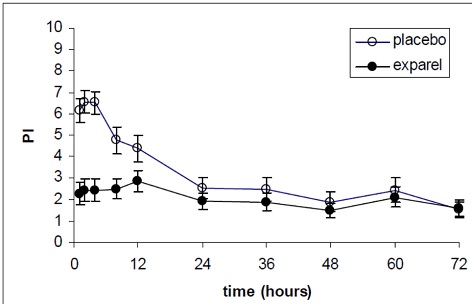
There were statistically significant, but small differences in the amount of opioid rescue analgesia used across the treatment groups, the clinical benefit of which has not been established. The median time to rescue analgesic use was 15 hours for patients treated with EXPAREL and one hour for patients treated with placebo. Twenty-eight percent of patients treated with EXPAREL required no rescue medication at 72 hours compared to 10% treated with placebo. For those patients who did require rescue medication, the mean amount of morphine sulfate intramuscular injections used over 72 hours was 22 mg for patients treated with EXPAREL and 29 mg for patients treated with placebo.
Study 3: Interscalene Brachial Plexus Nerve Block for Total Shoulder Arthroplasty or Rotator Cuff Repair
A multicenter, randomized, double-blind, placebo-controlled study (NCT02713230) was conducted in 156 patients undergoing primary unilateral total shoulder arthroplasty or rotator cuff repair with general anesthesia. The mean age was 61 years (range 33 to 80). Prior to the surgical procedure, patients received 10 mL of EXPAREL (133 mg) expanded with normal saline to 20 mL as a brachial plexus nerve block via interscalene or supraclavicular approach with ultrasound guidance. Only two patients received nerve block with EXPAREL by supraclavicular approach. Postsurgically, patients were administered acetaminophen/paracetamol up to 1000 mg PO or IV every 8 hours (q8h) unless contraindicated. Patients were allowed opioid rescue medication administered initially as oral immediate-release oxycodone (initiating at 5-10 mg every 4 hours or as needed). If a patient could not tolerate oral medication, IV morphine (2.5-5 mg) or hydromorphone (0.5-1 mg) could be administered every 4 hours or as needed.
In this study, there was a statistically significant treatment effect for EXPAREL compared to placebo in cumulative pain scores through 48 hours as measured by the AUC of the visual analog scale (VAS) pain intensity scores. There were statistically significant, but small differences in the amount of opioid consumption through 48 hours, the clinical benefit of which has not been demonstrated For those patients who required rescue medication, the mean amount of morphine-equivalent opioid rescue used over 48 hours was 12 mg for patients treated with EXPAREL and 54 mg for patients treated with placebo and 23 mg with EXPAREL vs. 70 mg for placebo over 72 hours.
Although at 48 hours, 9 subjects (13%) in the EXPAREL group remained opioid-free compared to 1 subject (1%) in the placebo group, a difference which was statistically significant, at 72 hours, there were 4 (6%) subjects in the EXPAREL group who remained opioid-free compared to 1 (1%) subject in the placebo group, a difference that is not statistically significant.
14.2 Studies That Do Not Support an Indication in Nerve Block
Studies 4 and 5: Femoral Nerve Block in Total Knee Arthroplasty
EXPAREL was administered via a femoral nerve block in two placebo-controlled studies. The results of these studies did not support a femoral nerve block indication due to inadequate safety data (Study 4 and Study 5) or due to inadequate efficacy findings (Study 5). In addition, patient falls were reported only in the EXPAREL treatment groups and none was reported in placebo groups.
Study 4
Study 4, a multicenter, randomized, double-blind, parallel-group, placebo-controlled study (NCT01683071), was conducted in 196 patients undergoing primary unilateral total knee arthroplasty (TKA) under general or spinal anesthesia. The mean age was 65 years (range 42 to 88). Prior to the surgical procedure, 20 mL of EXPAREL (266 mg) was administered as a femoral nerve block with ultrasound guidance. Postsurgically, patients were allowed opioid rescue medication administered initially by intravenous injection of hydromorphone and subsequently by a patient-controlled analgesia (PCA) pump containing morphine or hydromorphone only. Once patients were tolerating oral medication, oral immediate-release oxycodone was administered on an as-needed basis (but not more than 10 mg every 4 hours) or, if that was insufficient, a third rescue of bupivacaine HCl (0.125%, 1.25 mg/mL) was administered at a rate of 8 mL per hour via the previously placed femoral nerve catheter.
In this study, there was a statistically significant treatment effect for EXPAREL compared to placebo in cumulative pain scores through 72 hours as measured by the AUC of the NRS pain (at rest) intensity scores.
There was a statistically significant, although small decrease in opioid consumption for the EXPAREL treatment group compared to the placebo group, the clinical benefit of which has not been established. All patients in both the EXPAREL and placebo treatment groups required opioid rescue medication during the first 72 hours. The mean amount of opioid rescue used over 72 hours was 76 mg for patients treated with EXPAREL and 103 mg for patients treated with placebo.
The study was inadequate to fully characterize the safety of EXPAREL when used for femoral nerve block due to patient falls, which occurred only in the EXPAREL-treated patients and not the placebo-treated patients.
Study 5
Study 5, a multicenter, randomized, double-blind, parallel-group, placebo-controlled study (NCT02713178), was conducted in 230 patients undergoing primary unilateral total knee arthroplasty (TKA) under general or spinal anesthesia. The mean age was 65 years (range 39 to 89). Prior to the surgical procedure, either 20 mL of EXPAREL (266 mg) or 10 mL of EXPAREL (133 mg) plus 10 mL of normal saline was administered as a femoral nerve block with ultrasound guidance. In addition to study drug, 8 mL of bupivacaine HCl (0.5%) diluted with 8 mL of normal saline was administered by the surgeon as a periarticular infiltration to the posterior capsule (8 mL each behind the medial and lateral condyles) before placement of the prosthesis. Postsurgically, patients were allowed opioid rescue medication consisting of oral immediate-release oxycodone (initiated at 5 to 10 mg every 4 hours or as needed). If a subject could not tolerate oral medication, IV morphine (2.5 to 5 mg) or hydromorphone (0.5 to 1 mg) was permitted every 4 hours or as needed. Patient-controlled analgesia was not permitted. No other analgesic agents, including NSAIDs, were permitted through 108 hours. However, to reflect the current standard of care of postsurgical multimodal therapy, all subjects received cyclobenzaprine (a single dose of 10 mg orally or as needed) and acetaminophen/paracetamol (up to 1000 mg orally or IV every 8 hours for a maximum total daily dose of 3000 mg) postsurgically.
In this study there were no statistically significant treatment effects for the EXPAREL group compared to the placebo group in cumulative pain intensity scores or total opioid consumption. All patients in the EXPAREL and placebo treatment groups required opioid rescue medication over 72 hours. The mean amount of opioid rescue used over 72 hours was 69 mg for patients treated with EXPAREL 133 mg; 74 mg for patients treated with EXPAREL 266 mg, and 81 mg for patients treated with placebo. The median Tmax of bupivacaine observed in this study was 72 h with a range of 2.5 h to 108 h. Similarly to Study 4, patient falls only occurred in the EXPAREL-treated patients and not the placebo-treated patients.
Study 6: Intercostal Nerve Block for Posterolateral Thoracotomy
A multicenter, randomized, double-blind, placebo-controlled study was conducted in 191 patients undergoing posterolateral thoracotomy under general anesthesia (NCT01802411). The mean age was 58 years (range 18 to 82).
After the surgical procedure was completed but prior to the surgical site closure, 20 mL of EXPAREL was administered by the surgeon as an intercostal nerve block divided into three equal doses in three syringes of approximately 88 mg in 6.6 mL volume per nerve, and administered to each of three nerve segments (index nerve, nerve above, and nerve below). Postsurgically, patients were allowed opioid rescue medication administered initially by intravenous fentanyl 100 mcg, which was to be administered once via bolus only. For the US sites, the second rescue medication was to be PCA-administered morphine or hydromorphone. For the European sites, the second rescue medication was to be intramuscular administered morphine up to 10 mg every 4 hours. At all sites, once a subject was tolerating oral medication, oral immediate-release oxycodone was administered (but not more than 10 mg every 4 hours). Subjects who did not achieve adequate pain relief with this regimen were to be withdrawn from the study and followed for safety only.
In this study there were no statistically significant treatment effects for EXPAREL 266 mg compared to placebo in cumulative pain intensity scores or total opioid consumption. Four percent of patients treated with EXPAREL required no rescue medication at 72 hours compared to 1% treated with placebo. For those patients who did require rescue medication, the mean amount of opioid rescue used over 72 hours was 71 mg for patients treated with EXPAREL and 71 mg for patients treated with placebo. The median Tmax of bupivacaine observed in this study was 1 h with a range of 0.5 h to 50 h.
14.3 Study in Pediatric Patients Aged 6 Years and Older
Study 7
Study 7 was a multicenter, randomized, open-label, two-part study (NCT03682302) to evaluate the PK and safety of EXPAREL in pediatric subjects aged 6 to less than 17 years who were undergoing spine or cardiac surgery.
Sixty-one (61) subjects aged 12 to less than 17 years (Group 1), undergoing spine surgeries, were randomized 1:1 to receive either EXPAREL 4 mg/kg (maximum 266 mg) or bupivacaine HCl 2 mg/kg (maximum 175 mg). Postsurgically, patients were administered opioid rescue medication according to the study site’s standard of care.
Thirty-four (34) subjects aged 6 to less than 12 years (Group 2), undergoing either spine or cardiac surgeries, received EXPAREL 4 mg/kg (maximum up to 266 mg). Postsurgically, patients were administered opioid rescue medication according to the study site’s standard of care.
This study evaluated the safety of EXPAREL for local infiltration for pediatric subjects aged 6 and older [see Adverse Reactions (6.1), Pediatric Use (8.4), and Clinical Pharmacology (12.3)].
The efficacy of EXPAREL for local infiltration for pediatric subjects (6 to less than 17 years of age) was extrapolated from the efficacy of EXPAREL for local infiltration for adult subjects.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.