Source: FDA, National Drug Code (US) Revision Year: 2023
The mechanism of the antidepressant effect of EXXUA is not fully understood but is thought to be related to its modulation of serotonergic activity in the CNS through selective agonist activity at 5HT1A receptors.
The pharmacological activity of gepirone is attributed to the parent drug and its major metabolites 3'-OH-gepirone and 1-PP. Gepirone and its 3'-OH metabolite bind to 5HT1A receptors (Ki = 38 nM and 58 nM, respectively), where they act as agonists, while the 1-PP metabolite binds to alpha2 receptors (Ki = 42 nM).
In a thorough QT study, the largest mean increase in baseline- and placebo-corrected QTc interval with administration of 100 mg per day immediate-release formulation of gepirone was 18.4 msec (upper 90% confidence interval [CI] = 22.7 ms) on Day 1 and 16.1 msec (upper 90% CI = 20.7 ms) on Day 7. The exposure in this study was 2-fold the exposure of the maximum recommended dose [see Dosage and Administration (2.1) and Warnings and Precautions (5.2)].
The pharmacokinetics of EXXUA are linear and dose proportional from 18.2 mg to 72.6 mg. Steady-state plasma concentration are typically achieved within two to four days of daily dosing.
The absolute bioavailability is 14% to 17%. The maximal plasma EXXUA concentration (Cmax) after dosing is reached within 6 hours post dose (Tmax).
After a high fat meal, Tmax is reached at 3 hours. A significant effect of food has been observed on the peak plasma concentration (Cmax) of EXXUA and, to a lesser extent, on the total exposure (AUC0-tlast, AUC0-∞) to EXXUA. The magnitude of the food-effect was dependent of the fat content of the meal. The systemic exposure of EXXUA and major metabolites was consistently higher under fed conditions as compared to the fasted state. Gepirone Cmax after intake of low-fat (~200 calories) breakfast was 27% higher, after medium-fat (~500 calories) breakfast 55% higher and after a high-fat (~850 calories) breakfast 62% higher as compared to the fasted state. The AUC after intake of low-fat breakfast was about 14% higher, after a medium-fat breakfast 22% higher and after a high-fat breakfast 32 to 37% higher as compared to the fasted state. The effect of varying amounts of fat on Cmax and AUC of the major metabolites 3-OH-gepirone and 1PP were similar to that found for gepirone [see Dosage and Administration (2.2)].
The apparent volume of distribution of EXXUA is approximately 94.5L. The in vitro plasma protein binding in human is 72% and is not concentration dependent. The in vitro plasma protein binding for metabolite 3'-OH gepirone is 59% and 42% for 1-PP.
The mean terminal half-life is approximately 5 hours.
EXXUA is extensively metabolized and both major metabolites 1-PP and 3'-OH-gepirone are present in plasma in higher concentrations than the parent compound. CYP3A4 is the primary enzyme catalyzing the metabolism of EXXUA to its major pharmacologically active metabolites.
Following a single oral dose of [14C]-labeled gepirone, approximately 81% and 13% of the administered radioactivity was recovered in the urine and feces, respectively as metabolites. 60% of the gepirone was eliminated in the urine within the first 24 hours. The presence of hepatic or renal impairment did affect the apparent clearance of EXXUA.
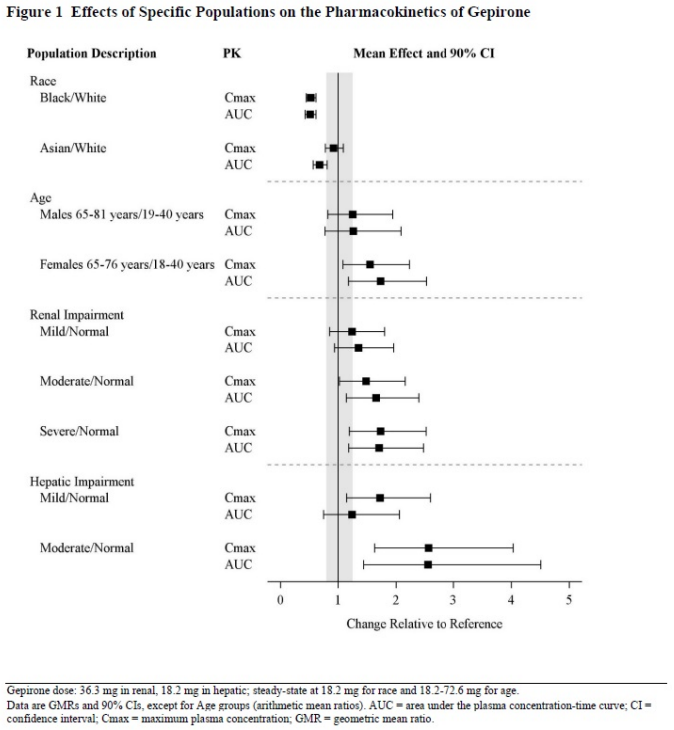
Specific Populations
Exposures of gepirone in specific populations are summarized in Figure 1 [see Dosage and Administration (2.3, 2.4, 2.5), Contraindications (4), and Use in Specific Populations (8.5,8.6, 8.7)].
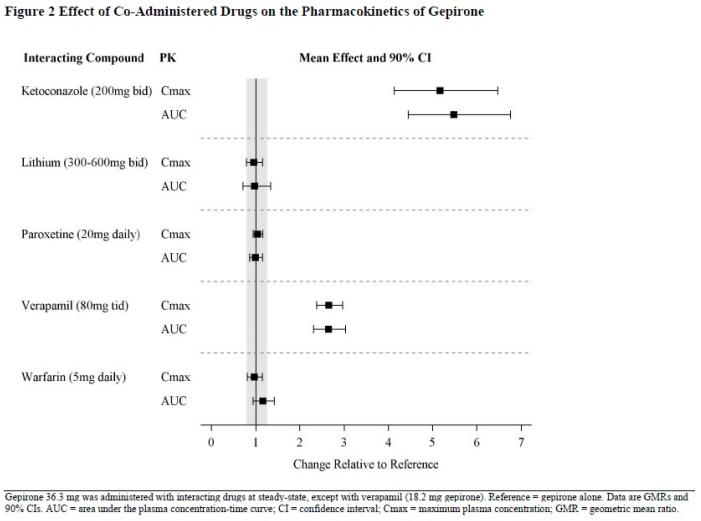
The effect of co-administered drugs on the pharmacokinetics of gepirone is summarized in Figure 2 [see Dosage and Administration (2.6) and Drug Interactions (7)].
Rifampin:
The effect of multiple oral dosing of potent cytochrome P450 3A4 inducer rifampin on the steady-state pharmacokinetics of EXXUA and its major metabolites 1-PP and 3'-OH-gepirone was investigated in 24 subjects. Combined therapy with rifampin (600 mg daily) and EXXUA (20 mg for two days, then 40 mg daily) decreased Cmax and AUC0-24 of EXXUA 20 times (EXXUA Cmax alone 9.63 ng/mL, with rifampin 0.491 ng/mL) and 29 times (EXXUA AUC0-24 alone 123 ng·hr/mL, with rifampin 4.19 ng·hr/mL), respectively. The Cmax and AUC0-24 of 3'-OH gepirone were decreased 2.5 times (3'-OH gepirone Cmax alone 23.0 ng/mL, with rifampin 9.30 ng/mL) and three times (3'-OH gepirone AUC0-24 alone 371 ng·hr/mL, with rifampin 126 ng·hr/mL), respectively. There was no effect on the pharmacokinetics of 1-PP (1-PP Cmax alone 6.37 ng/mL, with rifampin 6.02 ng/mL; 1-PP AUC0-24 alone 92.5 ng·hr/mL, with rifampin 81.1 ng·hr/mL).
Glyburide:
Under steady-state conditions for glyburide, the addition of 36.3 mg daily of EXXUA for six days in 16 patients with stable Type II diabetes resulted in statistically significantly lower AUC (glyburide AUC0-12 alone 574.8 ng·h/mL, with EXXUA 483.0 ng·h/mL) and Cmax (glyburide Cmax alone 121.0 ng/mL, with EXXUA 96.6 ng/mL) values for glyburide.
Drugs that Interfere with Hemostasis:
Following coadministration of stable dose of warfarin (INR 1.4 to 2.0) with multiple daily doses of EXXUA, no significant effect was observed in INR, prothrombin values, or total warfarin (protein bound plus free drug) pharmacokinetics for warfarin.
Drugs that Interfere with Protein Binding:
Gepirone is not highly bound to plasma protein and is not likely to be involved in interactions due to altered protein binding. In a clinical study with coadministration of EXXUA (18.2 mg) and warfarin, a highly protein-bound drug, no significant change in international normalized ratio (INR) was observed.
Gepirone at concentrations of 0.5, 5, and 50 ng/mL was shown to have no significant impact on the plasma protein binding of chlorpromazine, desipramine, diazepam, phenytoin, prazosin, propranolol, verapamil, or warfarin. The binding of digoxin and haloperidol were decreased (at maximum) by 5% and 9%, respectively. The plasma protein binding of lidocaine appeared to be increased by 4.9% in the presence of gepirone.
Alcohol:
An in vitro study showed dissolution rate for both 18.2 mg and 72.6 mg gepirone ER tablets decreased slightly as ethanol concentration increased in 0.01N HCl and 0.1N HCl at 0%, 5%, 10%, 20% and 40% alcohol. At 20 hours and 40% alcohol, approximately (mean) 76.8% and 80.7% were dissolved for the 18.2 mg and 72.6 mg gepirone ER tablets, respectively.
Transporter Systems:
EXXUA and its metabolites are unlikely to cause clinically significant inhibition of the following transporters based on in vitro data: P-gp, BCRP, BSEP, OATP1B1, OATP1B3, OAT1, OAT3, OCT2, MATE1, and MATE2-K. As such, no clinically relevant interactions with drugs metabolized/transported by these CYP enzymes or transporters would be expected.
Enzyme systems:
In addition, EXXUA has not been shown to be an inhibitor or inducer of any of the cytochrome P450 enzymes [see Clinical Pharmacology (12.3)]. Chronic administration of EXXUA is unlikely to induce the metabolism of drugs metabolized by these CYP isoforms.
No evidence of carcinogenic potential was observed in lifetime carcinogenicity studies performed in rats and mice at doses up to 43.6 and 317.8 mg/kg/day, respectively. These doses are approximately 6 and 18 times the maximum recommended human dose (MRHD), respectively, on a mg/m2 basis.
Gepirone showed no mutagenicity in three different in vitro genotoxicity assays (bacterial gene mutation, mammalian gene mutation, or DNA repair). No clastogenicity was observed in a rat micronucleus assay.
When gepirone was administered orally to male and female rats prior to and throughout mating at daily doses of 5, 27, 64, and 150 mg/kg, the latency to mating was increased at doses of 64 mg/kg (8 times the MRHD on a mg/m2 basis) and above.
The efficacy of EXXUA for the treatment for major depressive disorder (MDD) in adults was evaluated in two eight-week randomized, double-blind, placebo-controlled, flexible-dose studies in adults (age 18 to 69 years) meeting Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) criteria for MDD.
In Study 1, adult patients (18 to 69 years) who met DSM-IV diagnostic criteria for MDD were included in the trial. Patients in Study 1 had a median age of 39 years and were 61% female, 73% Caucasian, 9% Black, 2% Asian, and 16% Other (Hispanic or Native American). After an initial dosage of 18.2 mg once daily, the dosage was titrated to 36.3 mg once daily on Day 4 of treatment. The dosage could then be increased to 54.5 mg once daily after Day 7, and to 72.6 mg once daily after an additional 7 days. In patients that received EXXUA, the final daily dose of EXXUA was 72.6 mg in 64% of patients, 54.5 mg in 20% of patients, and 36.3 mg in 17% of patients.
In Study 2, adult patients (18 to 64 years) who met DSM-IV diagnostic criteria for MDD were included in the trial. Patients in Study 2 had a median age of 39 years and were 69% female, 65% Caucasian, 23% Black, 1% Asian, and 11% Hispanic. After an initial dosage of 18.2 mg daily, the dosage was titrated to 36.3 mg daily on Days 4 to 7 of treatment. The dosage could then be increased to 54.5 mg daily after Day 7, and to 72.6 mg daily after an additional 7 days. In patients that received EXXUA, the final daily dose of EXXUA was 72.6 mg in 66% of patients, 54.5 mg in 22% of patients, 36.3 mg in 10% of patients, and 18.2 mg in 2% of patients.
In Study 1 and Study 2, the primary efficacy measure was the change from baseline in the Hamilton Depression Rating Scale (HAMD-17) total score at Week 8. In both studies, patients in the EXXUA groups experienced statistically significantly greater improvement on the primary endpoint compared to patients in the placebo groups (see Table 4).
Table 4. Results for the Primary Endpoint: Change from Baseline in the HAMD-17 Total Score at Week 8 in Adult Patients with MDD (Study 1 and Study 2):
| Study Number | Treatment Group | N | Mean Baseline Score (SD) | LS Mean CFB (SE) | Placebo-subtracted Difference (95% CI) | |
|---|---|---|---|---|---|---|
| 1 | EXXUA (18.2 to 72.6 mg/day) | 101 | 22.7 (2.45) | -9.04 (0.78) | -2.47 (-4.41, -0.53) | |
| Placebo | 103 | 22.8 (2.51) | -6.75 (0.77) | |||
| 2 | EXXUA (18.2 to 72.6 mg/day) | 116 | 23.9 (2.69) | -10.22 (0.75) | -2.45 (-4.47, -0.43) | |
| Placebo | 122 | 24.2 (2.93) | -7.96 (0.73) | |||
N=number of patients in the primary efficacy analysis set; CFB=Change from baseline; LS=Least Squares; SD=Standard Deviation; SE=Standard Error
In Study 1, the final dose of EXXUA was 72.6, 54.5, and 36.3 mg/day in 64%, 20%, and 17% of patients, respectively.
In Study 2, the final dose of EXXUA was 72.6, 54.5, 36.3, and 18.2 mg/day in 66%, 22%, 10%, and 2% of patients, respectively.
The change from baseline in HAMD-17 total score by week compared to placebo for Study 2 in shown in Figure 3.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.