FLUANXOL / FLUANXOL DEPOT Tablet, Solution for injection Ref.[27894] Active ingredients: Flupentixol
Source: Health Products and Food Branch (CA) Revision Year: 2017
Indications and clinical use
Fluanxol tablets (flupentixol dihydrochloride) and Fluanxol Depot (flupentixol decanoate) are indicated for:
- maintenance therapy of chronic schizophrenic patients whose main manifestations do not include excitement, agitation or hyperactivity.
Geriatrics (>65 years of age): The pharmacokinetics, safety, and efficacy of flupentixol in elderly patients with schizophrenia have not been systematically evaluated in clinical trials. Caution should thus be exercised in dose selection for an elderly patient, recognizing the more frequent hepatic, renal and cardiac dysfunctions in this population.
Pediatrics (<18 years): Since the safety and efficacy of flupentixol in children has not been established, its use is not recommended in the pediatric age group.
Dosage and administration
Dosing Considerations
Fluanxol (flupentixol dihydrochloride) tablets
The dosage of Fluanxol tablets should be individualized and adjusted according to the severity of symptoms and tolerance to the drug. The maintenance dose can usually be given as a single morning dose.
The antipsychotic effect increases with increasing dosage; in addition some sedation should be anticipated.
Following stabilization on Fluanxol tablets, patients may be treated with Fluanxol Depot (flupentixol decanoate), administered by the intramuscular route.
When changing the medication from oral flupentixol to maintenance treatment with flupentixol decanoate the following guidelines should be used:
x mg p.o. daily corresponds to 4x mg decanoate every 2 weeks.
x mg p.o. daily corresponds to 8x mg decanoate every 4 weeks.
For example:
3 mg p.o. daily corresponds to 12 mg decanoate every 2 weeks.
3 mg p.o. daily corresponds to 24 mg decanoate every 4 weeks.
Oral flupentixol should be continued during the first week after the first injection but in diminishing dosage.
Patients being transferred from other depot preparations should receive a dose in the ratio of 40 mg flupentixol decanoate equivalent to 25 mg fluphenazine decanoate, to 200 mg zuclopenthixol decanoate, or to 50 mg haloperidol decanoate.
Fluanxol Depot (flupentixol decanoate)
The onset of action usually occurs in the range of 24 to 72 hours after injection and the improvement of symptoms continues for two to four weeks. However, there is considerable variation in the individual response of patients to flupentixol decanoate and its use for maintenance therapy requires careful supervision.
Flupentixol decanoate is administered by deep intramuscular injection into the gluteal region. Injection volumes exceeding 2 ml should be distributed between 2 injection sites. Local tolerability is good.
Fluanxol Depot is NOT for intravenous use.
As a long-acting depot preparation, Fluanxol Depot has been found useful in the maintenance treatment of non-agitated chronic schizophrenic patients who have been stabilized with shortacting neuroleptics and might benefit from transfer to a longer acting injectable medication. The changeover of medication should aim at maintaining a clinical outcome similar to or better than that obtained with the previous therapy. To achieve and maintain the optimum dose, the changeover from other neuroleptic medication should proceed gradually and constant supervision is required during the period of dosage adjustment in order to minimize the risk of overdosage or insufficient suppression of psychotic symptoms before the next injection.
Recommended Dose and Dosage Adjustment
Fluanxol tablets
The initial recommended dose of Fluanxol tablets is one mg three times a day. This may be increased, if necessary, by one mg every 2 to 3 days until there is effective control of psychotic symptoms. The usual maintenance dosage is 3 to 6 mg daily in divided doses, although doses of up to 12 mg daily or more have been used in some patients.
During the initial Fluanxol tablet therapeutic period, disturbance of sleep may occur, especially in those patients who have previously received neuroleptics possessing a marked sedative effect. In this event, the evening dose of Fluanxol tablets may be reduced.
Fluanxol Depot
Patients not previously treated with long-acting depot neuroleptics should be given an initial test dose of 5 mg (0.25 mL) to 20 mg (1.0 mL) of Fluanxol Depot 2%. An initial dose of 20 mg (1.0 mL) of Fluanxol Depot 2% is usually well tolerated; however, a 5 mg (0.25 mL) test dose of Fluanxol Depot 2% is recommended in elderly, frail and cachectic patients, and in patients whose individual or family history suggests a predisposition to extrapyramidal reactions. In the subsequent five to ten days, the therapeutic response and the appearance of extrapyramidal symptoms should be carefully monitored. Oral neuroleptic drugs may be continued, but in diminishing dosage, during this period.
In patients previously treated with long-acting depot neuroleptics who displayed good tolerance to these drugs, an initial dose of 20 to 40 mg (1.0 to 2.0 mL) of Fluanxol Depot 2% may be adequate.
Subsequent doses and the frequency of administration must be determined for each patient. There is no reliable dosage comparability between a shorter acting neuroleptic and depot flupentixol, and, therefore, the dosage of the long-acting drug must be individualized.
Except in particularly sensitive patients, a second dose of 20 (1.0 mL) to 40 mg (2.0 mL) of Fluanxol Depot 2% can be given 4 to 10 days after the initial injection. Subsequent dosage adjustments are made in accordance with the response of the patient, but the majority of patients can be adequately controlled by 20 to 40 mg (1.0 to 2.0 mL) of Fluanxol Depot 2% every two to three weeks. The optimal amount of the drug has been found to vary with the clinical circumstances and individual response. Doses greater than 80 mg (4.0 mL) of Fluanxol Depot 2% are usually not deemed necessary, although higher doses have been used occasionally in some patients.
Although the response to a single injection usually lasts for two to three weeks, it may last for four weeks or more, particularly when higher doses are used. Since higher doses increase the incidence of extrapyramidal reactions and other adverse effects, the amount of drug used should not be increased merely in order to prolong the intervals between injections. With higher doses there may also be more variability in the action of Fluanxol Depot and, therefore, unit dose increments should not exceed 20 mg (1.0 mL) of Fluanxol Depot 2%. After an appropriate dosage adjustment is achieved, regular and continuous supervision and reassessment is considered essential in order to permit any further dosage adjustments that might be required to ensure use of the lowest effective individual dose and avoid troublesome side effects.
Patients who require higher doses of Fluanxol Depot to control symptoms of schizophrenia and/or those who complain of discomfort with a large injection volume may be administered Fluanxol Depot 10% (100 mg/mL) in preference to Fluanxol Depot 2% (20 mg/mL).
Use in the Elderly: The use of flupentixol in elderly patients with schizophrenia has not been systematically evaluated. Caution should thus be exercised in dose selection for an elderly patient, recognizing the more frequent hepatic, renal and cardiac dysfunctions in this population.
Hepatic Impairment: the use of flupentixol is contraindicated in patients with impaired liver function.
Renal Impairment: the use of flupentixol is contraindicated in patients with impaired renal function.
Missed Dose
Fluanxol tablets
A missed dose should be taken at the next scheduled dose. Doses should not be doubled.
Discontinuation of Treatment
Fluanxol Tablets
Abrupt discontinuation of flupentixol may be accompanied by withdrawal symptoms. The most common symptoms are nausea, vomiting, anorexia, diarrhoea, rhinorrhoea, sweating, myalgias, paraesthesias, insomnia, restlessness, anxiety, and agitation. Patients may also experience vertigo, alternate feelings of warmth and coldness, and tremor. Symptoms generally begin within 1 to 4 days of withdrawal and abate within 7 to 14 days.
Abrupt withdrawal after short-term administration of antipsychotic drugs does not generally pose problems. However, transient dyskinetic signs are experienced by some patients on maintenance therapy after abrupt withdrawal. The signs are very similar to those described for tardive dyskinesia (see WARNINGS AND PRECAUTIONS, Tardive Dyskinesia), except for duration.
Although it is not known whether gradual withdrawal of antipsychotic drugs will decrease the incidence of withdrawal emergent neurological signs, gradual withdrawal would appear to be advisable.
Administration
Fluanxol tablets
Fluanxol tablets may be taken with or without food.
Fluanxol Depot
As with all oily injections it is important to ensure, by aspiration before injection, that inadvertent intravascular injection does not occur.
As with all parenteral drug products, the injection should be inspected visually for clarity, particulate matter, precipitate, discoloration and leakage prior to administration, whenever solution and container permit. Solution showing haziness, particulate matter, precipitate, discoloration or leakage should not be used. Discard unused portion.
How to open an ampoule:
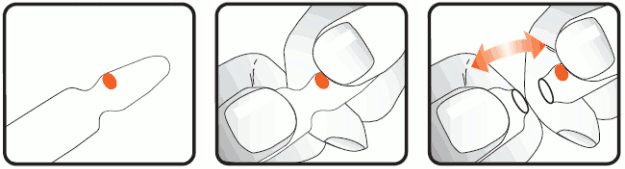
The ampoule can only be broken in one direction. The breaking point can be found on the neck of the ampoule next to the red dot. The pressure must be applied under the red dot.
Hold the ampoule with the red dot facing up. Position your thumbs on each side of the neck of the ampoule, one on the top of the red dot and the other on the label. Apply pressure using your index fingers and snap the ampoule in an upward direction. Keep the ampoule away from you at all times when opening.
Flupentixol decanoate should not be mixed with depot formulations with sesame oil as the vehicle because this would result in definite changes in the pharmacokinetic properties of the involved preparations.
Overdosage
Overdosage can be characterized by sedation, frequently preceded by extreme agitation, excitement, confusion, somnolence, coma, convulsions and hyperthermia/hypothermia. Extrapyramidal symptoms may develop, and respiratory and circulatory collapse may occur.
ECG changes, QT prolongation, Torsades de Pointes, cardiac arrest and ventricular arrhythmias have been reported when flupentixol is administered in overdose together with drugs known to affect the heart.
Treatment is symptomatic.
An airway should be maintained. Severe hypotension calls for the immediate use of an I.V. vasopressor drug, such as levarterenol. Epinephrine should not be used, as a further lowering of blood pressure may result. Antiparkinsonian medication should be administered only if extrapyramidal symptoms develop.
Fluanxol (flupentixol dihydrochloride) tablets
In the case of Fluanxol (flupentixol dihydrochloride) tablet overdose, gastric lavage should be carried out immediately and measures aimed at supporting the respiratory and cardiovascular systems instituted.
Fluanxol Depot (flupentixol decanoate)
No further injections should be given until the patient shows signs of relapse and the dosage then should be decreased.
For management of a suspected drug overdose, contact your regional Poison Control Centre.
Storage and stability
Fluanxol (flupentixol dihydrochloride) tablets: Store at room temperature (15 to 25°C) in a well-closed container.
Fluanxol Depot (flupentixol decanoate): Fluanxol Depot should be stored between 15°C and 25°C and protected from light.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.