GAZYVA Solution for injection Ref.[10820] Active ingredients: Obinutuzumab
Source: FDA, National Drug Code (US) Revision Year: 2021
12.1. Mechanism of Action
Obinutuzumab is a monoclonal antibody that targets the CD20 antigen expressed on the surface of pre-B and mature B lymphocytes. Upon binding to CD20, obinutuzumab mediates B-cell lysis through (1) engagement of immune effector cells, (2) by directly activating intracellular death signaling pathways (direct cell death), and/or (3) activation of the complement cascade. The immune effector cell mechanisms include antibody-dependent cellular cytotoxicity (ADCC) and antibody-dependent cellular phagocytosis.
As an antibody with reduced fucose content, obinutuzumab induces greater ADCC activity than rituximab in vitro using human cancer cell lines. Obinutuzumab also demonstrated an increased ability to induce direct cell death when compared to rituximab. Obinutuzumab binds to FcγRIII using purified proteins with a higher affinity than rituximab. Obinutuzumab and rituximab bind with similar affinity to overlapping epitopes on CD20.
12.2. Pharmacodynamics
In patients with CLL, GAZYVA caused CD19 B-cell depletion (defined as CD19 B cell counts <0.07 × 109/L). Initial CD19 B cell recovery was observed in some patients approximately 9 months after the last GAZYVA dose. At 18 months of follow-up, some patients remain B cell depleted.
Although the depletion of B cells in the peripheral blood is a measurable pharmacodynamic effect, it is not directly correlated with the depletion of B-cells in solid organs or in malignant deposits. B cell depletion has not been shown to be directly correlated to clinical response.
Cardiac Electrophysiology
The potential effects of GAZYVA on the QTc interval have not been studied.
12.3. Pharmacokinetics
The pharmacokinetic parameters of obinutuzumab after 100 mg on day 1 and 900 mg on day 2 of Cycle 1, 1,000 mg on day 8 and 15 of Cycle 1, and 1,000 mg on day 1 of Cycles 2–6 for CLL and after 1,000 mg on day 1, 8 and 15 of Cycle 1, 1,000 mg on day 1 of Cycles 2-6 or Cycles 2-8, and then 1,000 mg every 2 months for up to 2 years for NHL are provided in Table 10. The dosing regimen is within the linear pharmacokinetic behavior of obinutuzumab.
Table 10. Obinutuzumab Measures of Exposure:
| PK Measure | CLL* | Relapsed or refractory FL* | First line FL in combination with chemotherapy | |
|---|---|---|---|---|
| GAZYVA + Bendamustine* | GAZYVA + CHOP or CVP† | |||
| Cmax, µg/mL | 466.3 (35) | 553.5 (32) | 513.4 (28) | 676.4 (30) |
| Ctrough, µg/mL | 192.5 (78) | 295 (56) | 255 (46) | 395 (44) |
| AUC, µg/mL*day | 8701 (51) | 11362 (41) | 10088 (35) | 10723 (37) |
Results are presented as geometric mean (% Coefficient of Variation).
* Induction Cycle 6 of a 28-day cycle;
† Induction Cycle 8 of a 21-day cycle.
Distribution and Elimination
The elimination of obinutuzumab is comprised of a linear clearance pathway and a time-dependent non-linear clearance pathway. As GAZYVA treatment progresses, the impact of the time-dependent pathway diminishes in a manner suggesting target-mediated drug disposition (TMDD) and saturation of the TMDD at the end of the treatment cycle at the proposed clinical dose regimen. The pharmacokinetic properties of obinutuzumab in patients with CLL and NHL are provided in Table 11.
Table 11. Pharmacokinetic Parameters of Obinutuzumab:
| CLL | NHL | |
|---|---|---|
| Distribution | ||
| Volume of Distribution*, L | 4.1 (20) | 4.3 (21) |
| Elimination | ||
| Terminal Half-life, days | 25.5 (48) | 35.3 (35) |
| Clearance, L/day | 0.11 (53) | 0.08 (41) |
Parameters are presented as geometric mean (% Coefficient of Variation).
* At steady state.
Specific Populations
Age (median [range]: 63 [22, 89] years) and baseline creatinine clearance (CLcr) (median [range] 84 [22, >120] mL/min) did not affect the pharmacokinetics of GAZYVA. In patients with CLcr ≤30 mL/min, the pharmacokinetics of GAZYVA was unaffected. GAZYVA has not been studied in patients with hepatic impairment.
The volume of distribution and steady-state clearance increased with body weight; however, the expected change in exposure does not warrant a dose modification.
13.1. Carcinogenesis, Mutagenesis, Impairment of Fertility
No carcinogenicity or genotoxicity studies have been conducted with obinutuzumab.
No specific studies have been conducted to evaluate potential effects on fertility; however, no adverse effects on male or female reproductive organs were observed in the 26-week repeat-dose toxicity study in cynomolgus monkeys.
14. Clinical Studies
14.1 Chronic Lymphocytic Leukemia
The efficacy of GAZYVA was evaluated in a three-arm, open-label, active-controlled, randomized, multicenter trial (CLL11; NCT01010061) in 781 patients with previously untreated CD20+ CLL requiring treatment who had coexisting medical conditions or reduced renal function as measured by creatinine clearance (CLcr) <70 mL/min. Patients with CLcr <30 mL/min, active infections, positive hepatitis B (HBsAg or anti-HBc positive; patients positive for anti-HBc could be included if hepatitis B viral DNA was not detectable) and hepatitis C serology, or immunization with live virus vaccine within 28 days prior to randomization were excluded from the trial. Patients were treated with chlorambucil control (Arm 1), GAZYVA in combination with chlorambucil (Arm 2), or rituximab product in combination with chlorambucil (Arm 3). The safety and efficacy of GAZYVA was evaluated in a Stage 1 comparison of Arm 1 vs. Arm 2 in 356 patients and a Stage 2 comparison of Arm 2 vs. Arm 3 in 663 patients.
The majority of patients received 1,000 mg of GAZYVA on days 1, 8 and 15 of the first cycle, followed by treatment on the first day of 5 subsequent cycles (total of 6 cycles, 28 days each). The first dose of GAZYVA was divided between day 1 (100 mg) and day 2 (900 mg) [see Dosage and Administration (2.2)], which was implemented in 140 patients. Chlorambucil was given orally at 0.5 mg/kg on day 1 and day 15 of all treatment cycles (1 to 6).
In CLL11, the median age was 73 years, 62% were male, and 95% were White. Sixty-five percent had a CLcr <70 mL/min and 76% had multiple coexisting medical conditions. Twenty-two percent of patients were Binet stage A, 42% were stage B, and 36% were stage C. The median estimated CLcr was 62 mL/min. Eighty-one percent of patients treated with GAZYVA in combination with chlorambucil received all 6 cycles compared to 89% of patients in the rituximab product treated arm and 67% in the chlorambucil alone arm.
In the Stage 1 analysis of CLL11, the median progression-free survival (PFS) in the GAZYVA in combination with chlorambucil arm was 27.2 months and 11.2 months in the chlorambucil alone arm (median observation time 22.8 months) as assessed by independent review and is consistent with investigator-assessed PFS. The median overall survival (OS) was not yet reached with a total of 46 deaths: 22 (9%) in the GAZYVA in combination with chlorambucil arm and 24 (20%) in the chlorambucil arm. The hazard ratio for OS was 0.41 (95% CI: 0.23-0.74).
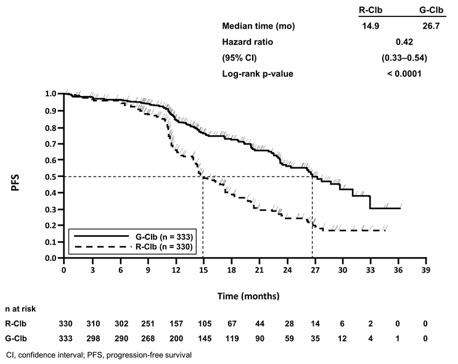
In the Stage 2 analysis of CLL11, the median PFS was 26.7 months in the GAZYVA arm and 14.9 months in the rituximab product arm with a median observation time of 18.7 months (HR: 0.42, 95% CI: 0.33-0.54, p-value<0.0001). These results were assessed by independent review and are consistent with investigator-assessed PFS. Minimal residual disease (MRD) was evaluated using allele-specific oligonucleotide polymerase chain reaction (ASO-PCR). The cutoff for a negative status was one CLL cell per 104 leukocytes in the sample (i.e., an MRD value of <10-4 was considered negative). Among patients who achieved complete response (CR) and complete response with incomplete marrow recovery (CRi; 94 patients in the GAZYVA arm and 34 patients in the rituximab product arm), 18 patients (19%) had negative MRD in the bone marrow in the GAZYVA arm compared to 2 patients (6%) in the rituximab product arm. Out of the patients who achieved CR and CRi, 39 patients (41%) in the GAZYVA arm, and 4 patients (12%) in the rituximab product arm were MRD negative in peripheral blood samples collected at least 3 months after the end of treatment.
Efficacy results are shown in Table 12 and Figures 1 and 2.
Table 12. Efficacy Results from CLL11:
| Endpoint | Stage 1 of CLL11 | Stage 2 of CLL11 | ||
|---|---|---|---|---|
| GAZYVA + Chlorambucil* | Chlorambucil | GAZYVA + Chlorambucil* | Rituximab product + Chlorambucil | |
| n=238 | n=118 | n=333 | n=330 | |
| Median Progression-Free Survival† | 27.2 months | 11.2 months | 26.7 months | 14.9 months |
| (HR 0.19 [0.14; 0.27], p-value<0.0001 stratified log-rank test) | (HR 0.42 [0.33; 0.54], p-value<0.0001 stratified log-rank test) | |||
| Overall Response Rate‡ | 78.2% | 33.1% | 79.6% | 66.3% |
| Complete Response | 28.2% | 0 | 26.1% | 8.8% |
| Complete Response with Incomplete Marrow Recovery | 2.5% | 1.7% | 2.1% | 1.5% |
| Partial Response | 45.0% | 30.5% | 48.6% | 54.1% |
| Nodular Partial Response | 2.5% | 0.8% | 2.7% | 1.8% |
| Median Duration of Response | 22.4 months | 4.7 months | 19.6 months | 9.7 months |
| Overall Survival | HR 0.41 [0.23; 0.74] | Not Yet Mature | ||
* All Stage 1 GClb patients (n=238) were included in the Stage 2 GClb population (n=333).
† As defined by independent review. Investigator-assessed PFS was consistent with data from independent review.
‡ Defined as best overall response rate (ORR = CR + CRi + PR + nPR).
Figure 1. Kaplan-Meier Curve of Overall Survival in Patients with CLL in CLL11 (Stage 1):
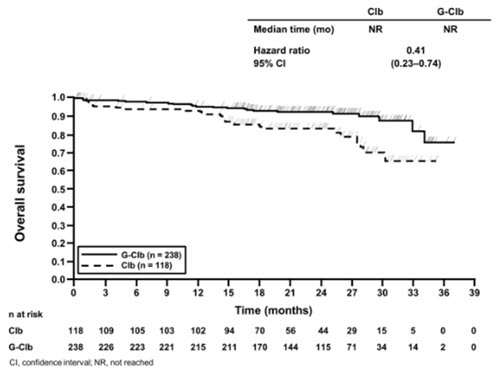
Figure 2. Kaplan-Meier Curve of Progression-Free Survival in Patients with CLL in CLL11 (Stage 2):
14.2 Follicular Lymphoma
GADOLIN
The efficacy of GAZYVA was evaluated in GADOLIN (NCT01059630), an open-label, multicenter, randomized study that included 335 patients with follicular lymphoma (FL) who had no response to or have progressed during or within 6 months of rituximab product or a rituximab product-containing regimen. These patients were randomized to receive either bendamustine alone (n=171) or GAZYVA in combination with bendamustine (n=164) for 6 cycles, each of 28 days duration. Patients in the GAZYVA plus bendamustine arm who did not have disease progression [patients with a complete response (CR), partial response (PR) or stable disease (SD)] at the end of the 6 cycles continued receiving GAZYVA monotherapy for 2 years. Patients were stratified according to the type of refractoriness to rituximab product (refractory to rituximab product monotherapy versus rituximab product in combination with chemotherapy), the number of prior therapies (≤2 versus >2), and geographic region.
GAZYVA was given by intravenous infusion as a flat dose of 1,000 mg on Days 1, 8 and 15 of Cycle 1, on Day 1 of Cycles 2–6, and then every 2 months until disease progression for up to 2 years. Bendamustine was given intravenously on Days 1 and 2 for all treatment cycles (1–6) at 90 mg/m²/day when given in combination with GAZYVA or 120 mg/m²/day when given alone.
The primary analysis included 321 FL patients, including 166 patients randomized to bendamustine alone and 155 patients randomized to GAZYVA in combination with bendamustine. In the primary analysis, patients had a median age of 63 years, 88% were White and 56% were male. Thirty-four percent had bulky disease (>6 cm), 15% had at least one B-symptom at baseline and 95% had an ECOG performance status of 0–1 at baseline. The median time since initial diagnosis was 3 years and the median number of prior therapies was 2 (range 1 to 10). Forty-six percent of patients received 1 prior therapy and 33% of patients received 2 prior therapies. Twenty percent of patients were refractory to prior rituximab product monotherapy, 37% of patients were refractory to prior rituximab product plus chemotherapy induction treatment, and 41% of patients were refractory to rituximab product maintenance treatment received following rituximab product plus chemotherapy induction. Seventy-nine percent of patients were refractory to both rituximab product and an alkylating agent during any prior regimen (double refractory).
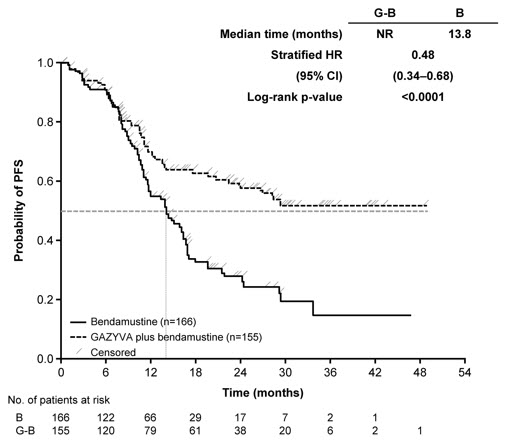
The major efficacy outcome measure was PFS as determined by an independent review committee (IRC). At the time of the primary analysis, median observation time was 21.1 months. The median PFS in the bendamustine arm was 13.8 months. Median PFS was not reached in the GAZYVA plus bendamustine arm (PFS HR = 0.48, 95% CI: 0.34-0.68; stratified log-rank test p-value<0.0001). The investigator assessed PFS result was consistent with the IRC-assessed PFS. The median investigator-assessed PFS in the bendamustine arm was 13.7 months and the median in the GAZYVA containing arm was 29.2 months (PFS HR = 0.48, 95% CI: 0.35-0.67; stratified log-rank test p-value<0.0001).
Efficacy results are summarized in Table 13. The Kaplan-Meier curve for IRC-PFS is shown in Figure 3.
Table 13. Primary Analysis Efficacy Results from GADOLIN*,†:
| Endpoint | GADOLIN | |
|---|---|---|
| GAZYVA + Bendamustine followed by GAZYVA monotherapy n=155 | Bendamustine n=166 | |
| Median Progression-Free Survival (months) | Not Reached | 13.8 |
| (HR = 0.48 [0.34; 0.68], p-value<0.0001 by stratified log-rank test) | ||
| Best Overall Response‡ | 78.7% | 74.7% |
| Complete Response | 15.5% | 18.7% |
| Partial Response | 63.2% | 56.0% |
| Median duration of response (months) | Not Reached | 11.6 |
* Based on FL population.
† As defined by independent review.
‡ Best response of PR or CR within 12 months of study start.
Figure 3. Kaplan-Meier Curve of IRC-Assessed Progression-Free Survival in Patients with FL:
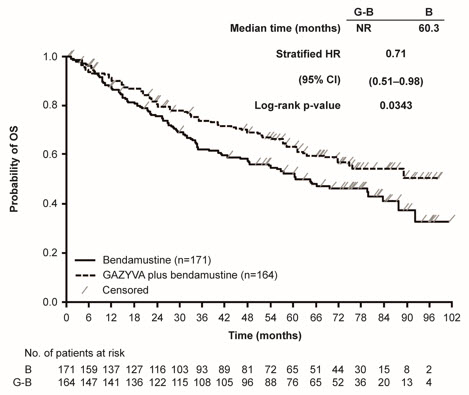
The final analysis included a total of 335 patients with 171 randomized to bendamustine alone and 164 to GAZYVA in combination with bendamustine. With an overall median observation time of 52.2 months (range: 0-100.9 months), there were 66 deaths (40.2%) in the GAZYVA arm and 85 deaths (51.3%) in the bendamustine-alone arm (OS HR = 0.71, 95% CI: 0.51, 0.98). The Kaplan-Meier curve for OS is presented in Figure 4.
Figure 4. Kaplan-Meier Curve of Overall Survival in Patients with FL:
GALLIUM
The efficacy of GAZYVA was evaluated in GALLIUM (NCT01332968), a multicenter, open-label, randomized study that included 1202 patients with previously untreated, stage II bulky, III or IV FL. Patients were randomized 1:1 to receive either GAZYVA (n=601) or rituximab product (n=601) in combination with chemotherapy (CHOP, CVP, or bendamustine) for 6–8 cycles. Patients were stratified by chemotherapy (selected by each site; all patients at that site received the chosen chemotherapy regimen), FLIPI (Follicular Lymphoma International Prognostic Index) risk group and geographic region. Patients with at least PR to combination therapy received monotherapy with GAZYVA (1,000 mg) or rituximab product every two months until disease progression or for a maximum of two years. The study excluded patients with follicular lymphoma grade 3b or transformed disease; patients having an ANC <1500/µL, platelets <75,000/µL, or CLcr <40 mL/min; and patients with hepatic transaminases >2.5 × upper limit of normal unless attributable to lymphoma.
GAZYVA was given by intravenous infusion as a flat dose of 1,000 mg on Days 1, 8 and 15 of Cycle 1 and Day 1 of subsequent treatment cycles.
GAZYVA and bendamustine were given in six 28-day cycles. Bendamustine was administered at 90 mg/m²/day on Days 1 and 2 of each cycle, with prednisone 100 mg orally or equivalent on Day 1 of Cycle 1.
GAZYVA and CHOP were given in six 21-day cycles. Subsequently, two additional cycles of GAZYVA were given for a total of 8 GAZYVA cycles. CHOP consisted of cyclophosphamide 750 mg/m² intravenously, doxorubicin 50 mg/m², and vincristine 1.4 mg/m² (maximum dose, 2 mg) on Day 1 and prednisone 100 mg orally on Days 1-5.
GAZYVA and CVP were given in eight 21-day cycles. CVP consisted of cyclophosphamide 750 mg/m² intravenously and vincristine 1.4 mg/m² (maximum dose, 2 mg) on Day 1 and prednisone 100 mg orally on Days 1-5.
Patients had a median age of 59 years, 81% were White and 53% were female; 7% had Stage II, 35% had Stage III, and 56% had Stage IV disease, with 44% having bulky disease (≥7 cm) overall; 79% had a FLIPI score of >2; and 97% had an ECOG performance status of 0–1. The chemotherapy was bendamustine in 57%, CHOP in 33%, and CVP in 10% of patients.
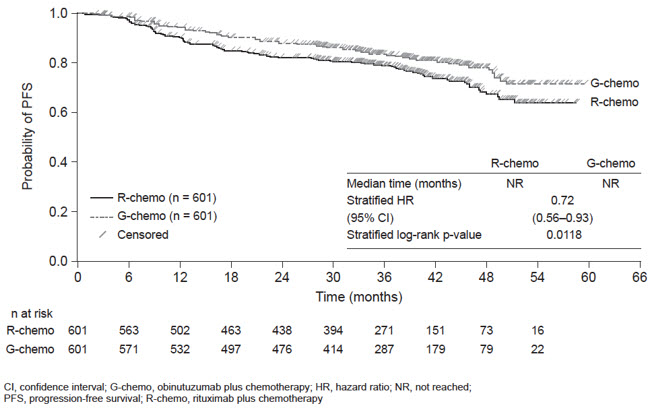
Efficacy was based on PFS per IRC, with a median observation time of 38 months. Upon interim analysis, the risk of progression or death was significantly reduced in the GAZYVA containing arm compared to the rituximab product containing arm (Table 14). Kaplan-Meier curves for PFS are shown in Figure 5. Overall response and complete remission rates were similar.
Table 14. Efficacy in Previously Untreated Follicular Lymphoma (GALLIUM):
| Endpoint per IRC | GAZYVA + chemotherapy followed by GAZYVA monotherapy n=601 | Rituximab product + chemotherapy followed by rituximab product monotherapy n=601 |
|---|---|---|
| Progression-Free Survival* Number of events (%) | 108 (18%) | 141 (23%) |
| HR = 0.72 [95% CI: 0.56, 0.93], p-value=0.0118† | ||
| Overall Response Rate‡ | 91% | 88% |
| Complete Remission Rate‡ | 28% | 27% |
* Investigator-assessed PFS was consistent with data from independent review.
† Stratified log-rank test
‡ After completion of combination therapy. Assessed by CT without positron emission tomography.
Figure 5. Kaplan-Meier Curves of Progression Free Survival in Patients with Previously Untreated FL:
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.