ILUMETRI Solution for injection Ref.[7619] Active ingredients: Tildrakizumab
Source: European Medicines Agency (EU) Revision Year: 2021 Publisher: Almirall, S.A., Ronda General Mitre, 151, 08022, Barcelona, Spain
Pharmacodynamic properties
Pharmacotherapeutic group: Immunosuppressants, interleukin inhibitors
ATC code: L04AC17
Mechanism of action
Tildrakizumab is a humanized IgG1/k monoclonal antibody that specifically binds to the p19 protein subunit of the interleukin-23 (IL-23) cytokine without binding to IL-12 and inhibits its interaction with the IL-23 receptor.
IL-23 is a naturally occurring cytokine that is involved in inflammatory and immune responses. Tildrakizumab inhibits the release of proinflammatory cytokines and chemokines.
Clinical efficacy and safety
The multicentre, randomised, double-blind, placebo-controlled trials reSURFACE 1 and reSURFACE 2 studies enrolled a total of 1,862 patients 18 years of age and older with plaque psoriasis who had a minimum body surface area involvement of 10%, a Physician Global Assessment (PGA) score of ≥3 in the overall assessment (plaque thickness, erythema, and scaling) of psoriasis on a severity scale of 0 to 5, a Psoriasis Area and Severity Index (PASI) score ≥12, and who were candidates for phototherapy or systemic therapy.
In these studies, patients were randomised to either placebo or tildrakizumab (including 200 mg and 100 mg at 0, 4 and every twelve weeks thereafter [Q12W]), up to 52 or 64 weeks. In the active comparator study (reSURFACE 2), patients were also randomised to receive etanercept 50 mg twice weekly for 12 weeks, and weekly thereafter up to 28 weeks.
Overall demographic and baseline characteristics in reSURFACE1 and reSURFACE2 studies were consistent across individual trials. Patients were 18 to 82 years old, with a mean age of 45.9. The median baseline PASI score ranged from 17.7 to 18.4 across treatment groups. Baseline PGA score was marked or severe in 33.4% of patients. Of all patients, 35.8% had received prior phototherapy, 41.1% had received prior conventional systemic therapy, 16.7% had received prior biologic therapy for the treatment of plaque psoriasis. A total of 15.4% of study patients had a history of psoriatic arthritis. Mean baseline Dermatology Life Quality Index (DLQI) ranged from 13.0 to 14.8.
Studies reSURFACE 1 and reSURFACE 2 assessed the changes from baseline at Week 12 in the two coprimary endpoints: 1) PASI 75 and 2) PGA of “0” (cleared) or “1” (minimal), with at least a 2-point improvement from baseline. Other evaluated outcomes included the proportion of patients who achieved PASI 90, PASI 100, the proportion of patients with DLQI 0 or 1, and maintenance of efficacy up to 52/64 weeks.
Results obtained at weeks 12, 28 and beyond (up to week 64 in reSURFACE 1 and up to week 52 in reSURFACE 2) are presented in Table 2 and Table 3.
Table 2. Summary of Response Rates in Studies reSURFACE 1 and reSURFACE 2:
| Week 12 (2 doses)* | Week 28 (3 doses) | ||||||
|---|---|---|---|---|---|---|---|
| 200 mg | 100 mg | Placebo | Etanercept | 200 mg | 100 mg | Etanercept | |
| reSURFACE1 | |||||||
| Number of patients | 308 | 309 | 154 | - | 298 | 299 | - |
| PASI 75a (%) | 62.3b† | 63.8b† | 5.8b | - | 81.9c | 80.4c | - |
| PGA of “clear” or “minimal” with ≥2 grade improvement from Baselinea (%) | 59.1b† | 57.9b† | 7.1b | - | 69.1c | 66.0c | - |
| PASI 90 (%) | 35.4b† | 34.6b† | 2.6b | - | 59.0c | 51.6c | - |
| PASI 100 (%) | 14.0b† | 13.9b† | 1.3b | - | 31.5c | 23.5c | - |
| DLQI Score 0 or 1 (%) | 44.2† | 41.5† | 5.3 | - | 56.7c | 52.4c | - |
| reSURFACE2 | |||||||
| Number of patients | 314 | 307 | 156 | 313 | 299 | 294 | 289 |
| PASI 75a (%) | 65.6b†‡ | 61.2b†‡ | 5.8b | 48.2b | 72.6b‡ | 73.5b‡ | 53.6b |
| PGA of “clear” or “minimal” with ≥2 grade improvement from Baselinea (%) | 59.2†b¥ | 54.7b† | 4.5b | 47.6b | 69.2b‡ | 64.6b‡ | 45.3b |
| PASI 90 (%) | 36.6b†‡ | 38.8b†‡ | 1.3b | 21.4b | 57.7c‡ | 55.5‡c | 29.4c |
| PASI 100 (%) | 11.8b†‡ | 12.4b†‡ | 0 | 4.8b | 27.0c‡ | 22.8c‡ | 10.7c |
| DLQI Score 0 or 1 (%) | 47.4†¥ | 40.2† | 8.0 | 35.5 | 65.0c‡ | 54.1c‡ | 39.4c |
a Co-primary efficacy endpoint at week 12.
b Non responder imputation for missing data.
c No imputation for missing data.
* The number of doses administered refers only to tildrakizumab groups.
n = number of patients in the full analysis set for which data was available, after imputation when applicable.
p-values calculated using the Cochran-Mantel-Haenszel (CMH) test stratified by body weight (≤90 kg, >90 kg) and prior exposure to biologic therapy for psoriasis (yes/no).
† p≤0.001 versus placebo; ‡p≤0.001 versus etanercept; ¥p≤0.05 versus etanercept.
Maintenance of Response
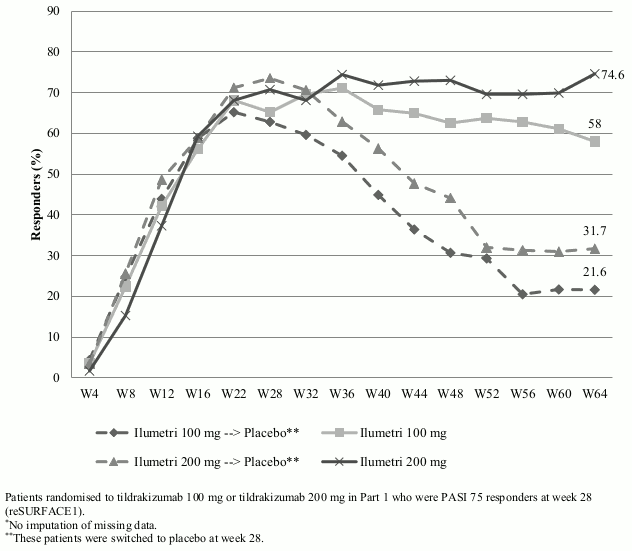
The maintenance of response in studies reSURFACE1 and reSURFACE2 are presented in Table 3. Maintenance and durability of PASI 90 response over time is presented in Figure 1.
Table 3. Maintenance of Response in Studies reSURFACE 1 and reSURFACE 2:
| Long term responsea,b | ||||
|---|---|---|---|---|
| 200 mg | 100 mg | |||
| reSURFACE 1 | Week 28 | Week 64 | Week 28 | Week 64 |
| Number of patients | 116 | 114 | 115 | 112 |
| PGA of “clear” or “minimal” with ≥2 grade improvement from Baseline (%) | 80.2 | 76.3 | 80.9 | 61.6 |
| PASI 90 (%) | 70.7 | 74.6 | 65.2 | 58.0 |
| PASI 100 (%) | 38.8 | 40.4 | 25.2 | 32.1 |
| reSURFACE 2 | Week 28 | Week 52 | Week 28 | Week 52 |
| Number of patients | 108 | 105 | 213 | 204 |
| PGA of “clear” or “minimal” with ≥2 grade improvement from Baseline (%) | 88.0 | 84.8 | 84.0 | 79.4 |
| PASI 90 (%) | 75.0 | 81.9 | 74.2 | 78.4 |
| PASI 100 (%) | 34.3 | 46.7 | 30.2 | 35.3 |
a Long-term response in patients who were responders (had achieved at least PASI 75) to tildrakizumab at week 28.
b No imputation for missing data.
Figure 1. Maintenance and durability of PASI 90 Response. Proportion of Patients with PASI 90 response over time up to Week 64 (Full Analysis Set Part 3*):
Quality of Life/Patient-reported Outcomes
At week 12 and across studies, tildrakizumab was associated with statistically significant improvement in Health-related Quality of Life as assessed by the DLQI (Table 2). Improvements were maintained over time with at week 52, 63.7% (100 mg) and 73.3% (200 mg) in reSURFACE 1, and 68.8% (100 mg) and 72.4% (200 mg) in reSURFACE 2 of patients who were PASI 75 responders at week 28 having a DLQI of 0 or 1.
Paediatric population
The European Medicines Agency has deferred the obligation to submit the results of studies with Ilumetri in one or more subsets of the paediatric population in the treatment of plaque psoriasis (see section 4.2 for information on paediatric use).
Pharmacokinetic properties
Absorption
The subcutaneous formulation of tildrakizumab showed an absolute bioavailability ranging from 73% (90% CI: 46%-115%, 200 mg SC vs. 3 mg/kg IV) to 80% (90% CI: 62%-103%, 50 mg SC vs. 0.5 mg/kg IV) in healthy subjects, as a result of cross study single dose comparison. Maximum concentration was reached at 6.2 days after injection. Population PK analysis indicated a 31% higher bioavailability in healthy subjects compared to patients.
At steady state, following administration of 100 mg of tildrakizumab in subjects with moderate to severe plaque psoriasis geometric means (% CV) of AUC0-τ and Cmax values were respectively 305 μg·day/mL (41%) and 8.1 μg/mL (34%), whereas they were 612 μg·day/mL (40%) and 16.3 μg/mL (33%) following administration of 200 mg.
Distribution
Tildrakizumab has limited extravascular distribution with volume of distribution (Vd) values ranging from 76.9 to 106 mL/kg.
Biotransformation
Tildrakizumab is catabolized into component amino acids by general protein degradation processes. Small-molecule metabolic pathways (e.g., CYP450 enzymes, glucuronosyltransferases) do not contribute to its clearance.
Elimination
Clearance values range from 2.04 to 2.52 mL/day/kg and the half-life was 23.4 days (23% CV) in subjects with plaque psoriasis.
Linearity/non-linearity
Tildrakizumab exhibited dose-proportional pharmacokinetics in subjects with plaque psoriasis over a dose range from 50 mg to 400 mg following subcutaneous administration, with clearance being independent of dose.
Steady-state is achieved by 16 weeks with the clinical regimen of 0, 4, and every 12 weeks thereafter, with 1.1-fold accumulation in exposure between week-1 and week-12 independent of dose.
Body weight
Population pharmacokinetic modelling indicated that exposure decreased as body weight increased. The geometric mean exposure (AUC0-τ at steady state) in adult patients weighing >90 kg following a 100 mg or 200 mg SC dose was predicted to be about 30% lower than in an adult patient weighing ≤90 kg (see section 4.2).
Pharmacokinetics in special populations
Elderly
Population pharmacokinetic analysis indicated that age did not have a clinically significant influence on the clearance of tildrakizumab in adult subjects with plaque psoriasis. Following administration of 100 mg or 200 mg of tildrakizumab, subjects who are 65 years or older (n=81 and n=82, respectively) had a similar tildrakizumab clearance as compared to subjects less than 65 years old (n=884).
Renal and Hepatic impairment
No formal trial of the effect of hepatic or renal impairment on the pharmacokinetics of tildrakizumab was conducted. Tildrakizumab is catabolized into component amino acids by general protein degradation processes and is not eliminated by renal or hepatic pathways.
Drug interactions
Results from a drug-drug interaction study conducted in plaque psoriasis subjects suggest that tildrakizumab had no clinically relevant effect on CYP1A2, CYP2C9, CYP2C19, CYP2D6 and CYP3A4. Therefore, tildrakizumab does not impact the pharmacokinetics of concomitant medicines metabolized by CYP enzyme (see section 4.5).
Preclinical safety data
Non-clinical data reveal no special hazard for humans based on conventional studies of safety pharmacology, and repeated dose toxicity.
Animal carcinogenicity studies have not been conducted with tildrakizumab. Studies in mouse tumor models showed that selective inhibition of IL-23p19 does not increase carcinogenic risk.
In cynomolgus monkeys, there was negligible secretion of the product into breast milk. One month after birth, the milk/serum ratio was ≤0.002. Tildrakizumab was shown to distribute across the placental barrier. After repeated dosing to pregnant cynomolgus monkeys, serum concentrations were quantifiable in the fetus, but the reproduction toxicity studies did not reveal any untoward effects.
No effects on fertility parameters such as reproductive organs, menstrual cycle length, and/or hormones were observed in male and female cynomolgus monkeys that were administered tildrakizumab at doses resulting in >100 times the human exposure at the recommended clinical dose based on AUC.
In a pre- and postnatal development toxicity study in monkeys, no related increase in pregnancy loss was observed at exposures up to 85 times the human exposure at the recommended dose. No harmful effects were noted in neonates at maternal exposures up to 9 times the human exposure at the recommended dose. Two neonatal deaths from monkeys administered tildrakizumab at maternal exposure of 85 times the human exposure at the recommended dose were attributed to possible viral infection and considered of uncertain relationship to the treatment. The clinical significance of these findings is unknown.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.