ILUVIEN Intravitreal implant Ref.[7965] Active ingredients: Fluocinolone
Source: Medicines & Healthcare Products Regulatory Agency (GB) Revision Year: 2019 Publisher: Alimera Sciences Limited, Royal Pavilion, Wellesley Road, Aldershot, Hampshire, GU11 1PZ, United Kingdom
Pharmacodynamic properties
Pharmacotherapeutic group: ANTIINFLAMMATORY AGENTS, corticosteroids, plain
ATC code: S01BA15
Corticosteroids inhibit the inflammatory response to a variety of inciting agents. They inhibit the oedema, fibrin deposition, capillary dilation, leukocyte migration, capillary proliferation, fibroblast proliferation, deposition of collagen, and scar formation associated with inflammation.
Corticosteroids are thought to act by the induction of phospholipase A inhibitory proteins, collectively called lipocortins. It is postulated that these proteins control the biosynthesis of potent mediators of inflammation such as prostaglandins and leukotrienes by inhibiting the release of the common precursor arachidonic acid. Arachidonic acid is released from membrane phospholipids by phospholipase A2. Corticosteroids have also been shown to reduce levels of vascular endothelial growth factor, a protein which increases vascular permeability and causes oedema.
Diabetic Macular Oedema
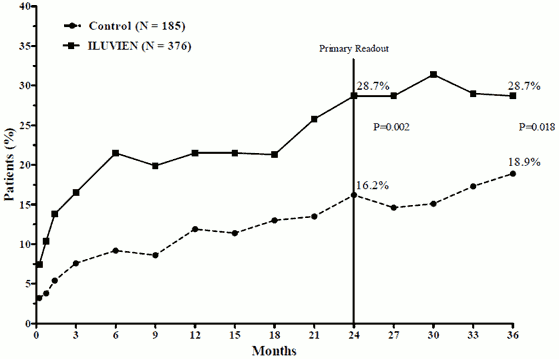
The efficacy of ILUVIEN was assessed in two randomized, multicenter, double-masked, parallel studies enrolling subjects with diabetic macular oedema who had previously been treated with laser photocoagulation at least once, each involving three years of follow-up. There were 74.4% of subjects treated with 1 implant, 21.6% with 2 implants, 3.5% with 3 implants and 0.5% with 4 implants and 0% > 4 implants). The primary efficacy endpoint in both trials was the proportion of subjects whose vision improved by 15 letters or greater after 24 months. In each of these trials, the primary endpoint was met for ILUVIEN (see Figure 1 for the integrated results of the primary efficacy endpoint).
Figure 1: Percentage of Subjects with ≥ 15 Letter Improvement Over Baseline, Integrated FAME Studies
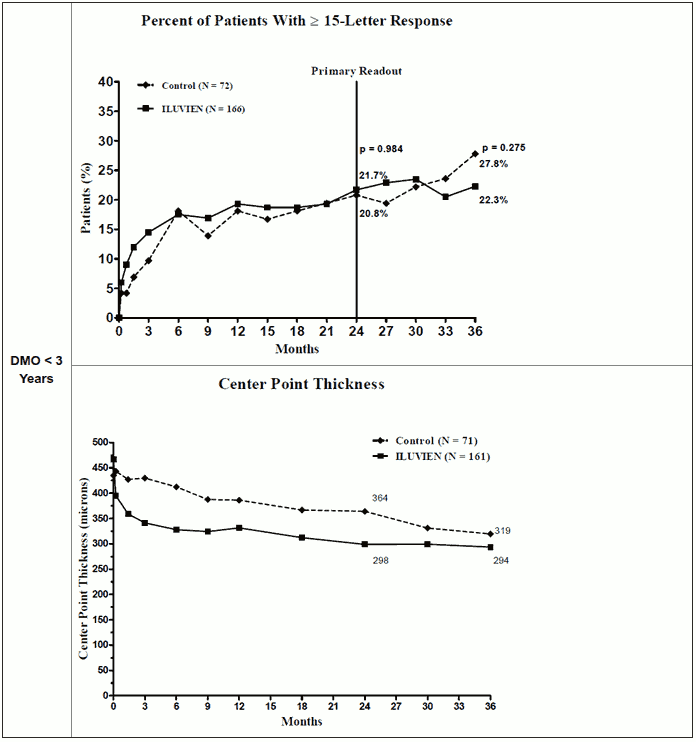
When efficacy was assessed as a function of duration of disease, those subjects with a duration of DMO greater than the median (≥3 years) had a significant beneficial response to ILUVIEN, whilst those with shorter duration DMO did not show an additional benefit over control treatment with regard to visual improvement (Figures 2 and 3). These subgroup data support the indication in Section 4.1, of use in patients with chronic DMO (ie, duration of at least 3 years).
Figure 2: Comparison of Percent of Subjects with ≥15 letter Improvement from Baseline BCVA and Mean Change from Baseline Excess Center Point Thickness by Duration of DMO Subgroup ≥ 3 years
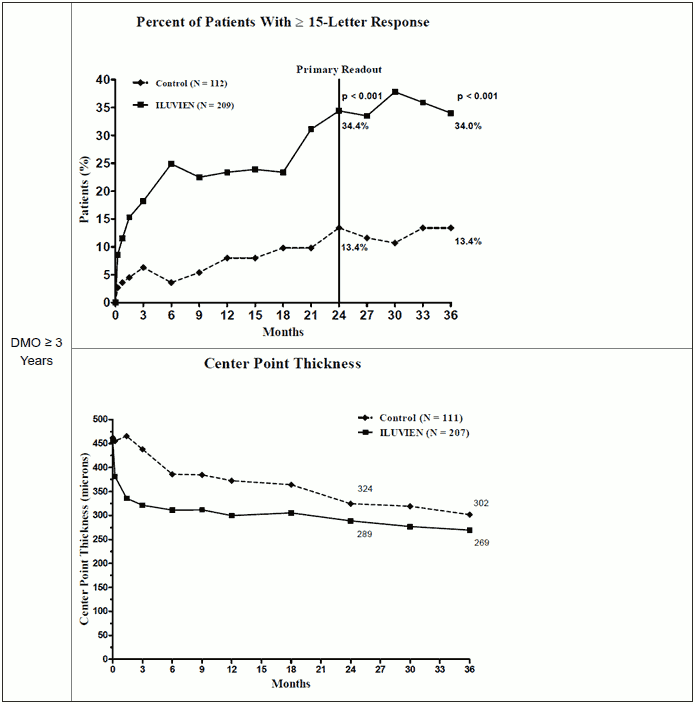
Figure 3: Comparison of Mean Change from Baseline Excess Center Point Thickness and Percent of Subjects with ≥15 letter Improvement from Baseline BCVA by Duration of DMO Subgroup < 3 years
Non-Infectious Uveitis-Posterior Segment
The ILUVIEN development programme for non-infectious uveitis affecting the posterior segment of the eye consists of two phase 3 studies to assess the safety and efficacy of 0.2 µg/day fluocinolone acetonide compared to sham injection over a 36-month period. Both studies are prospective, randomised, double-masked, sham-injection controlled, multicentre studies, of 282 patients in total who received either a single treatment with fluocinolone acetonide (188 subjects) or sham injection (94 subjects). The eligibility criteria were designed to enrol subjects with recurrent and persistent disease. At baseline, the ocular characteristics of patients enrolled in the studies are included inTable 2.
Table 2: Baseline Ocular Characteristics for the Study Eye (Intent To Treat (ITT) Population): PSV-FAI-001 and PSV-FAI-005
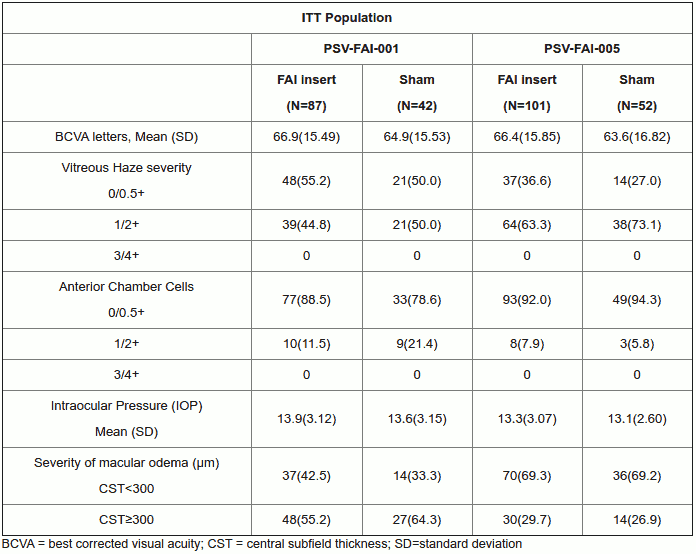
Data are No. (%) except where specified.
The primary efficacy endpoint was based on the proportion of subjects with an absence of recurrence of uveitis between randomization and month 6, where recurrence was defined as:
(a) ≥ 2 step increase in number of cells per high powered field compared with baseline or any visit time point prior to month 6; or
(b) an increase in vitreous haze of ≥ 2 steps compared to baseline or any visit time point prior to month 6; or
(c) a loss of best-corrected visual acuity of ≥ 15 letters compared to baseline at any visit time point prior to month 6.
Any criterion used to define recurrence was required to be attributable only to non-infectious uveitis. A subject who had not previously experienced a recurrence as defined in (a), (b), (c), and took a systemic corticosteroid or immunosuppressant, or a intra/peri-ocular or topical corticosteroid in the study eye at any time during the study prior to Month 6 was considered as having a recurrence. Recurrence could be treated using standard of care according to protocol defined criteria.
In each phase 3 clinical trial, the primary endpoint was met. See Tables 3 and 4 for the results of the primary efficacy endpoint comparing the proportion of recurrence of uveitis in the study eye versus the sham control. See figure 4 for a comparison of the time to recurrence of uveitis in these treatment groups.
Table 3: Proportion of Subjects with Recurrence of Uveitis in the Study Eye within 6 Months (ITT Population): PSV-FAI-001 and PSV-FAI-005
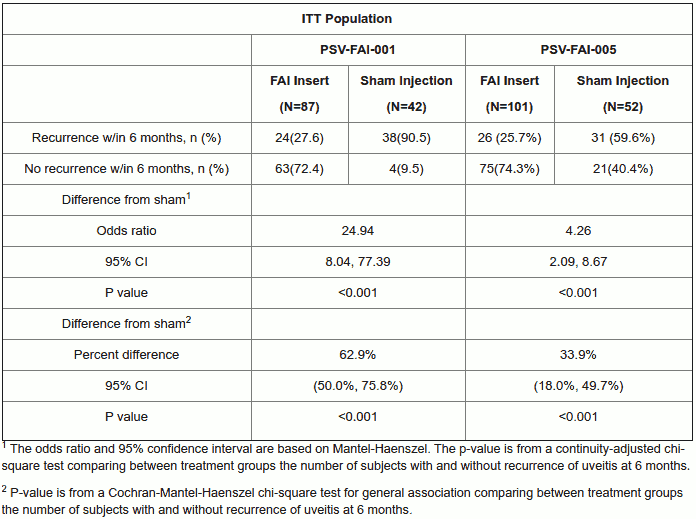
Table 4: Proportion of Subjects with Recurrence of Uveitis in the Study Eye within 6 Months (ITT Population): Pooled Uveitis Studies
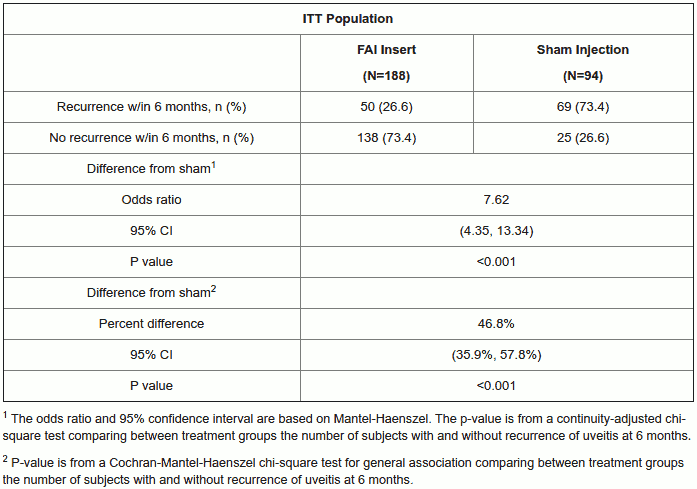
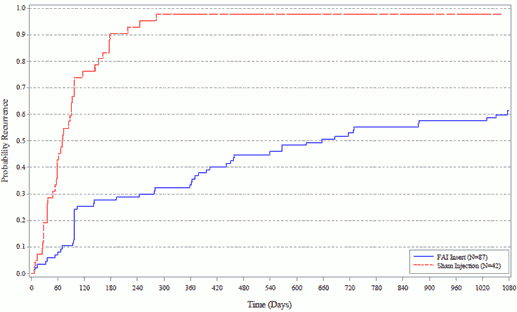
Figure 4: Kaplan-Meier Plot of Time to First Recurrences of Uveitis in the Study Eye within 6 Months (ITT Population): Pooled Uveitis Studies
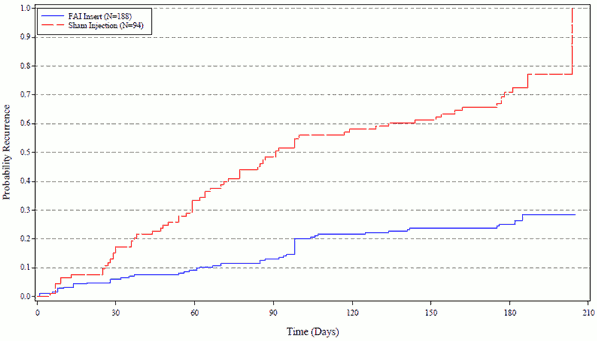
The p-value (p<0.001) comparing the two distributions of time-to-recurrence of uveitis are based on a log-rank test.
In the ITT population, the recurrence of uveitis in the study eye reported at 6 months was notably (p<0.001) lower in the ILUVIEN group (37.9%) compared with the sham injection group (97.6%); the odds ratio for the difference from sham injection was 67.09 (95% CI: 8.81, 511.06).
Persistence of efficacy was demonstrated using the 36-month results of the phase 3 study initiated first (PSV-FAI-001), (see table for PSV-FAI-001 results of the primary efficacy endpoint comparing the proportion of recurrence of uveitis in the study eye versus the sham control and figure for a comparison of the time to recurrence of uveitis in these treatment groups).
Table 5: Proportion of Subjects with Recurrence of Uveitis in the Study Eye within 36 Months (ITT Population) PSV-FAI-001
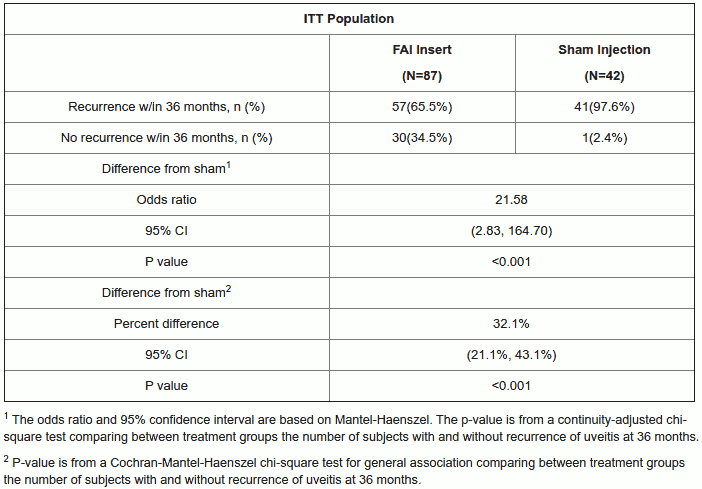
Figure 5: Kaplan-Meier Plot of Time to First Recurrences of Uveitis in the Study Eye within 36 Months (ITT Population): PSV-FAI-001
In the ITT population, the recurrence of uveitis in the study eye within 36 months was significantly lower (p<0.001) in the ILUVIEN group compared with the sham injection group.
Table 6: Number of Recurrence of Uveitis in the Study Eye within 6 Months (ITT Population): PSV-FAI-001 and PSV-FAI-005
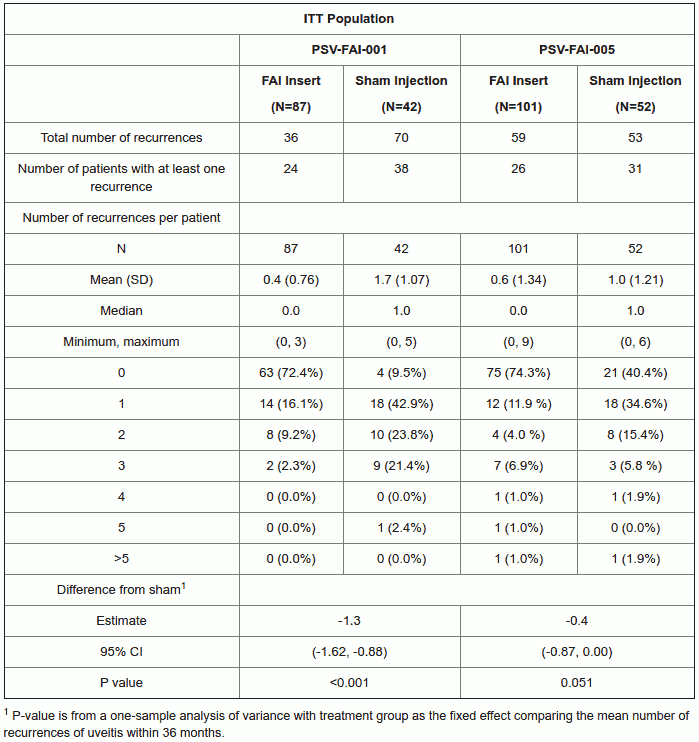
Table 7: Number of Recurrence of Uveitis in the Study Eye within 36 Months (ITT Population): PSV-FAI-001
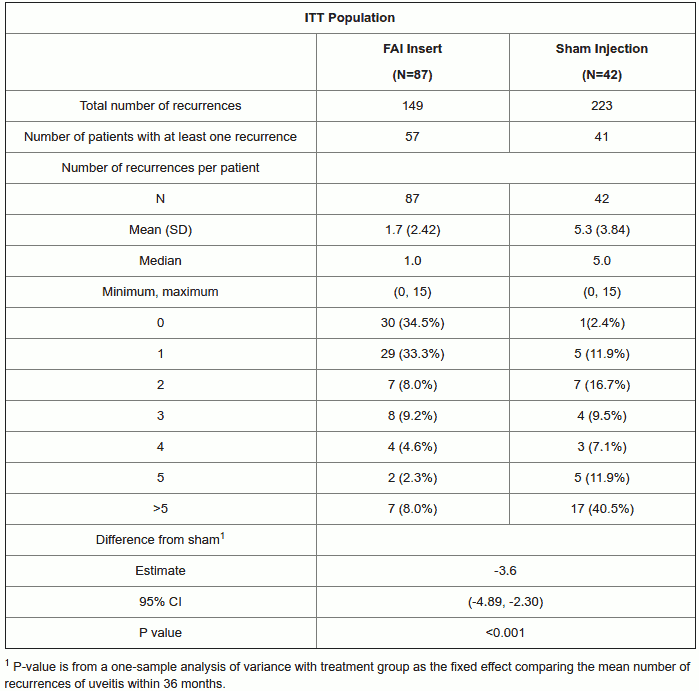
Patients treated with ILUVIEN experienced significantly fewer recurrences within 36 months than those treated with sham (1.7 recurrences vs. 5.3 recurrences, respectively, p<0.001).
Table 8: Number of Adjunctive Therapies for Uveitis in the Study Eye within 6 Months (ITT Population): PSV-FAI-001 and PSV-FAI-005
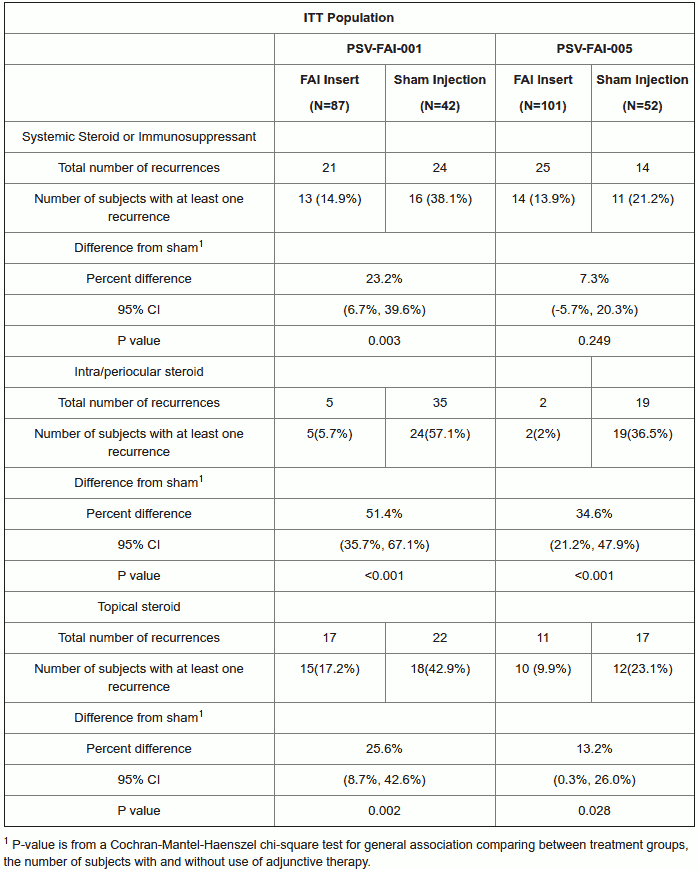
Table 9: Number of Adjunctive Therapies for Uveitis in the Study Eye within 36 Months (ITT Population): PSV-FAI-001
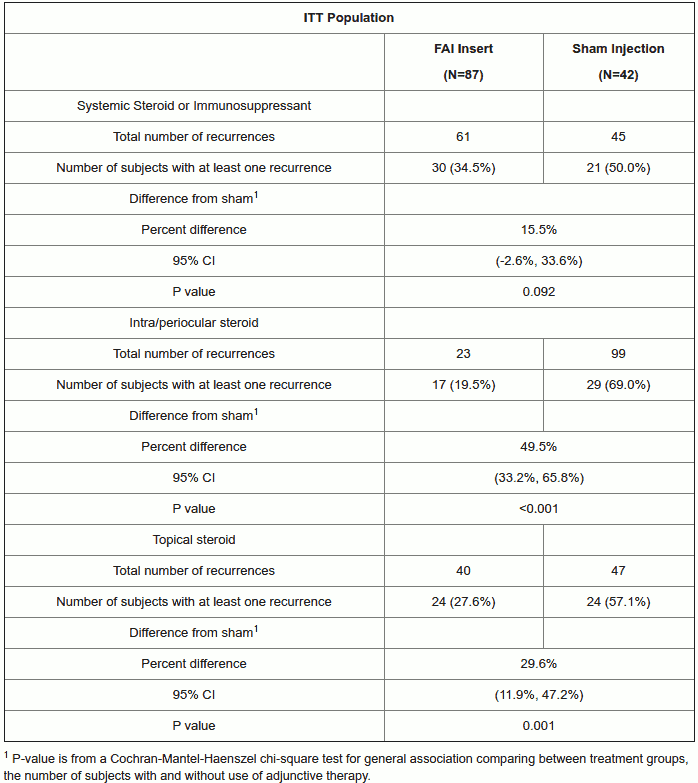
Significantly fewer patients treated with ILUVIEN versus sham required adjunctive intra/peri-ocular steroids (19.5% vs 69.0% respectively, p<0.001) or topical steroids (27.6% vs 57.1% respectively, p=0.001). Fewer patients required adjunctive systemic steroid or immunosuppressive therapy (34.5% vs 50.0% respectively, p=0.092).
The European Medicines Agency has waived the obligation to submit results of studies with intravitreally administered fluocinolone acetonide in all subsets of the paediatric population for the treatment of diabetic macular oedema. See Section 4.2 for information on paediatric use.
Pharmacokinetic properties
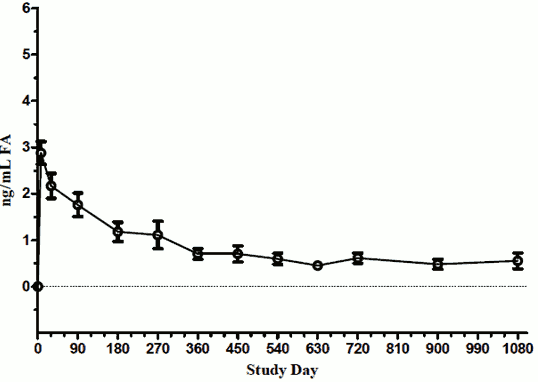
In a human pharmacokinetic study (C-01-06-002, the FAMOUS Study) fluocinolone acetonide concentrations in plasma were below the lower limit of quantitation of the assay (100 pg/mL) at all time points from Day 1 through Month 36. The maximal aqueous humor fluocinolone acetonide concentrations were observed on Day 7 for most of the subjects. Aqueous humor fluocinolone acetonide concentrations decreased over the first 3−6 months and remained essentially the same through Month 36 for subjects who were not retreated. Subjects who were retreated experienced a second fluocinolone acetonide peak concentration similar to that following the initial dose. After retreatment, aqueous humor concentrations of fluocinolone acetonide returned to levels approximately similar to those observed at the time of first treatment.
Figure 6: FA Levels in Human Aqueous Humor in Subjects Receiving 1 ILUVIEN Implant (FAMOUS Study)
Preclinical safety data
Fluocinolone acetonide has been shown to be teratogenic in mice and rabbits following systemic administration. No mutagenicity, carcinogenicity or developmental toxicity data are available for intravitreally administered fluocinolone acetonide. However, intravitreally administered fluocinolone acetonide was not detectable systemically and thus no systemic effects are anticipated.
Local effects (focal degenerative lesions affecting fibers in the posterior polar and posterior cortical regions of the lens) were observed in rabbits at doses of intravitreal fluocinolone acetonide in excess of the clinically used dose. Local effects (focal retinal scarring) were also seen in rabbits treated with both placebo and fluocinolone acetonide containing device. This scarring was not seen clinically in humans and is postulated to be due to anatomical differences between the rabbit and human eye.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.