IMAAVY Concentrate for solution for injection Ref.[115559] Active ingredients: Nipocalimab
Revision Year: 2025
12.1. Mechanism of Action
Nipocalimab-aahu is a human IgG1 monoclonal antibody that binds to neonatal Fc receptor (FcRn), resulting in the reduction of circulating IgG levels.
12.2. Pharmacodynamics
In Study 1 [see Clinical Studies (14)], the pharmacological effect of nipocalimab-aahu was assessed by measuring the decrease in serum IgG levels and anti-AChR and anti-MuSK autoantibody levels. In patients positive for AChR and MuSK autoantibodies who were treated with IMAAVY, there was a reduction in AChR and MuSK autoantibodies relative to baseline. Decreases in total IgG levels followed a similar pattern. A similar reduction in AChR autoantibodies was observed in adolescent patients with gMG compared to adults.
12.3. Pharmacokinetics
Nipocalimab exhibits nonlinear pharmacokinetics. Following a single intravenous infusion of IMAAVY at doses ranging from 0.3 to 60 mg/kg (4 times the recommended maintenance dosage) in healthy participants, Cmax of nipocalimab-aahu increased in a dose-proportional manner while AUC increased in a greater than dose-proportional manner.
Distribution
Mean volume of distribution of nipocalimab is 2.67 L.
Metabolism
Nipocalimab is expected to be degraded by proteolytic enzymes into small peptides and amino acids.
Elimination
Nipocalimab exhibits concentration-dependent pharmacokinetics. After a single intravenous administration of 15 mg/kg nipocalimab-aahu, the mean clearance is 0.0627 L/h and half-life is 29.3 hours.
Specific Populations
Age, Sex, and Race
The pharmacokinetics of nipocalimab were not affected by age, sex, or race based on a population pharmacokinetics analysis.
Pediatric Patients
Following the recommended intravenous doses of IMAAVY in adolescent patients 12 to 16 years of age with gMG (N=7), the observed steady-state serum nipocalimab-aahu concentrations were within the range of those observed for adult patients with gMG [see Use in Specific Populations (8.4)].
Patients with Renal Impairment
No dedicated pharmacokinetic study has been conducted in patients with renal impairment. Renal impairment is not expected to affect the pharmacokinetics of nipocalimab. Based on a population pharmacokinetic analysis, which included healthy volunteers and patients with gMG with mild to moderate renal impairment, renal function (estimated glomerular filtration rate [eGFR] 30–89 mL/min/1.73 m²) had no clinically significant effect on nipocalimab-aahu clearance. No dose adjustment is required in patients with renal impairment.
Patients with Hepatic Impairment
No dedicated pharmacokinetic study has been performed in patients with hepatic impairment. Nipocalimab is not metabolized by cytochrome P450 enzymes, and hepatic impairment is not expected to affect the pharmacokinetics of nipocalimab. Based on a population pharmacokinetic analysis, which included healthy volunteers and patients with gMG with mild to moderate hepatic impairment, there was no clinically significant effect on nipocalimab-aahu clearance. No dose adjustment is required in patients with hepatic impairment.
Drug Interactions with Other Drugs or Biological Products
IgG-Based Monoclonal Antibodies
Nipocalimab decreases concentrations of compounds that bind to the human FcRn, including IgG based monoclonal antibodies.
Cytochrome P450 Enzymes
Nipocalimab is not metabolized by cytochrome P450 enzymes; therefore, interactions with concomitant medications that are substrates, inducers, or inhibitors of cytochrome P450 enzymes are unlikely.
13.1. Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
Studies to assess the carcinogenic potential of nipocalimab-aahu have not been conducted.
Mutagenesis
Studies to assess the genotoxic potential of nipocalimab-aahu have not been conducted. As an antibody, nipocalimab-aahu is not expected to interact directly with DNA.
Impairment of Fertility
Once or twice weekly intravenous administration of nipocalimab-aahu (0, 20, 50, 100, or 300 mg/kg) to male and female monkeys for 26 weeks resulted in no adverse effects on reproductive organs upon histopathological examination. The highest dose tested was 20 times the recommended human maintenance dose (15 mg/kg) on a mg/kg basis.
14. Clinical Studies
The efficacy of IMAAVY for the treatment of gMG in adults who are anti-AChR or anti-MuSK antibody positive was established in a 24-week, multicenter, randomized, double-blind, placebo-controlled study (Study 1; NCT04951622). Patients were treated with IMAAVY with the recommended dosage regimen [see Dosage and Administration (2.1)].
Study 1 enrolled patients with gMG who met the following criteria:
- Myasthenia Gravis Foundation of America (MGFA) Clinical Classification Class II to IV
- Myasthenia Gravis-Activities of Daily Living (MG-ADL) total score of at least 6
- On stable dose of standard of care MG therapy prior to baseline that included acetylcholinesterase (AChE) inhibitors, steroids or non-steroidal immunosuppressive therapies (NSISTs), either in combination or alone.
In Study 1, a total of 196 patients were randomized 1:1 to receive IMAAVY (n=98) or placebo (n=98). Baseline characteristics were similar between treatment groups. For the primary efficacy analysis population (n=153), patients had a median age of 52 years at screening (range 20 to 81 years) and a median time since diagnosis of 6 years. Sixty percent of patients were female; 63% were White; 32% were Asian; 1% were Black or African-American; and <1% were American Indian or Alaskan Native. At baseline, median MG-ADL total score was 9, and median Quantitative Myasthenia Gravis (QMG) total score was 15. Eighty-eight percent (n=134) of patients were positive for AChR antibodies and 10% (n=16) were positive for MuSK antibodies.
At baseline, in each group, 85% of patients received AChE inhibitors, 66% of patients received steroids, and 54% of patients received NSISTs at stable doses.
The efficacy of IMAAVY was measured using the MG-ADL scale, which assesses the impact of gMG on daily functions of 8 signs and symptoms that are typically affected in gMG. Each item is assessed on a 4-point scale, where a score of 0 represents normal function and a score of 3 represents loss of ability to perform that function. A total score ranges from 0 to 24, with the higher scores indicating more impairment.
The primary efficacy endpoint was the comparison of the mean change from baseline to Weeks 22, 23, and 24 between treatment groups in the MG-ADL total score. A statistically significant difference favoring IMAAVY was observed in MG-ADL total score change from baseline (p=0.002; see Table 2 and Figure 1).
The efficacy of IMAAVY was also measured using the QMG total score, which is a 13-item categorial grading system that assesses muscle weakness. Each item is assessed on a 4 -point scale, where a score of 0 represents no weakness, and a score of 3 represents severe weakness. A total possible score ranges from 0 to 39, where higher scores indicate more severe impairment.
The secondary endpoint was the comparison of the mean change from baseline to Weeks 22 and 24 between treatment groups in the QMG total score. A statistically significant difference favoring IMAAVY was observed in the QMG total score change from baseline (p<0.001; see Table 2).
The results are presented shown in Table 2.
Table 2. Least Squares Mean Change from Baseline to Week 24 in MG-ADL and QMG Total Scores in Study 1:
| Efficacy Endpoints | IMAAVY N=77 LS Mean (SE) | Placebo N=76 LS Mean (SE) | IMAAVY Change Relative to Placebo LS Mean Difference (95% CI) | p-value |
|---|---|---|---|---|
| Primary Endpoint | ||||
| MG-ADL Total Score* | -4.7 (0.33) | -3.3 (0.34) | -1.5 (-2.4, -0.5) | 0.002 |
| Secondary Endpoint | ||||
| QMG Total Score† | -4.9 (0.5) | -2.1 (0.5) | -2.8 (-4.2, -1.4) | <0.001 |
Key: CI=confidence interval; MG-ADL = Myasthenia Gravis – Activities of Daily Living; QMG = Quantitative Myasthenia Gravis; LS mean = Least squares mean; SE = standard error
* Mean change from baseline over weeks 22, 23, and 24
† Mean change from baseline over weeks 22 and 24
Figure 1 shows the mean change from baseline to Week 24 in MG-ADL total score in Study 1, and Figure 2 shows the mean change from baseline to Week 24 in QMG total score in Study 1.
Figure 1. Least Squares Mean Change from Baseline in MG-ADL Total Score Over 24 Weeks in Study 1:
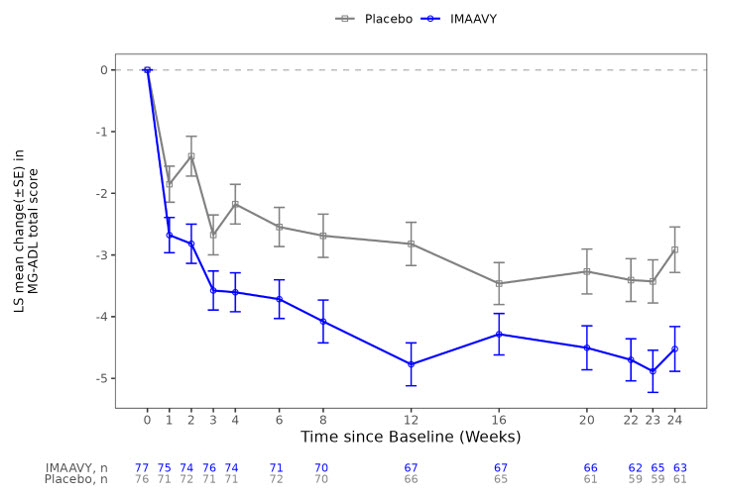
LS = least squares, SE = standard error, MG-ADL = Myasthenia Gravis Activities of Daily Living
Figure 2. Least Squares Mean Change from Baseline in QMG Total Score Over 24 Weeks in Study 1:
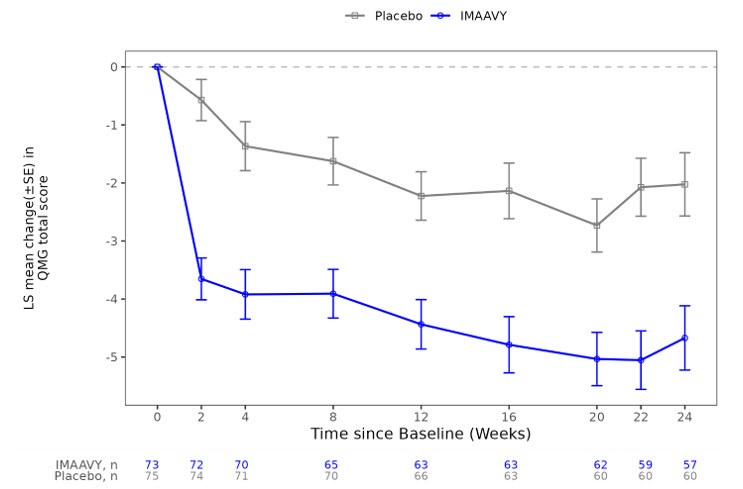
LS = least squares, SE = standard error, QMG = Quantitative Myasthenia Gravis.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.