INVEGA Prolonged-release tablet Ref.[7471] Active ingredients: Paliperidone
Source: European Medicines Agency (EU) Revision Year: 2021 Publisher: Janssen-Cilag International NV, Turnhoutseweg 30, B-2340 Beerse, Belgium
Pharmacodynamic properties
Pharmacologic group: Psycholeptics, other antipsychotics
ATC code: N05AX13
INVEGA contains a racemic mixture of (+)- and (-)-paliperidone.
Mechanism of action
Paliperidone is a selective blocking agent of monoamine effects, whose pharmacological properties are different from that of traditional neuroleptics. Paliperidone binds strongly to serotonergic 5-HT2- and dopaminergic D2receptors. Paliperidone also blocks alfa1-adrenergic receptors and blocks, to a lesser extent, H1-histaminergic and alfa2-adrenergic receptors. The pharmacological activity of the (+) and (-)-paliperidone enantiomers are qualitatively and quantitatively similar.
Paliperidone is not bound to cholinergic receptors. Even though paliperidone is a strong D2-antagonist, which is believed to relieve the positive symptoms of schizophrenia, it causes less catalepsy and decreases motor functions to a lesser extent than traditional neuroleptics. Dominating central serotonin antagonism may reduce the tendency of paliperidone to cause extrapyramidal side effects.
Clinical efficacy
Schizophrenia
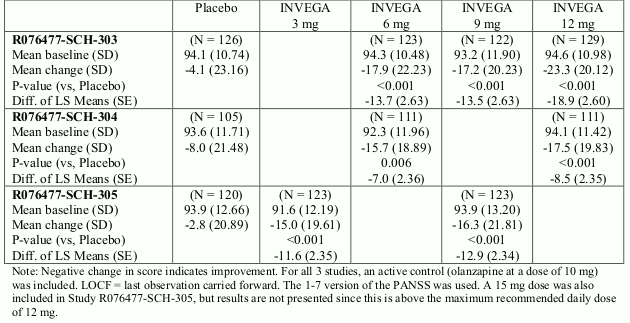
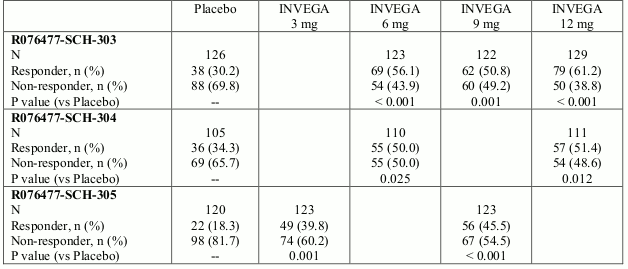
The efficacy of INVEGA in the treatment of schizophrenia was established in three multi-centre, placebo-controlled, double-blind, 6-week trials in subjects who met DSM-IV criteria for schizophrenia. INVEGA doses, which varied across the three studies, ranged from 3 to 15 mg once daily. The primary efficacy endpoint was defined as a decrease in total Positive and Negative Syndrome Scale (PANSS) scores as shown in the following table. The PANSS is a validated multi-item inventory composed of five factors to evaluate positive symptoms, negative symptoms, disorganised thoughts, uncontrolled hostility/excitement, and anxiety/depression. All tested doses of INVEGA separated from placebo on day 4 (p<0.05). Predefined secondary endpoints included the Personal and Social Performance (PSP) scale and the Clinical Global Impression–Severity (CGI-S) scale. In all three studies, INVEGA was superior to placebo on PSP and CGI-S. Efficacy was also evaluated by calculation of treatment response (defined as decrease in PANSS Total Score ≥30%) as a secondary endpoint.
Schizophrenia Studies: Positive and Negative Syndrome Scale for Schizophrenia (PANSS) Total Score - Change From Baseline to End Point - LOCF for Studies R076477-SCH-303, R076477-SCH-304, and R076477-SCH-305: Intent-to-Treat Analysis Set:
Schizophrenia Studies: Proportion of Subjects with Responder Status at LOCF End Point Studies R076477-SCH-303, R076477-SCH-304, and R076477-SCH-305: Intent-to-Treat Analysis Set:
In a long-term trial designed to assess the maintenance of effect, INVEGA was significantly more effective than placebo in maintaining symptom control and delaying relapse of schizophrenia. After having been treated for an acute episode for 6 weeks and stabilised for an additional 8 weeks with INVEGA (doses ranging from 3 to 15 mg once daily) patients were then randomised in a double-blind manner to either continue on INVEGA or on placebo until they experienced a relapse in schizophrenia symptoms. The trial was stopped early for efficacy reasons by showing a significantly longer time to relapse in patients treated with INVEGA compared to placebo (p=0.0053).
Schizoaffective disorder
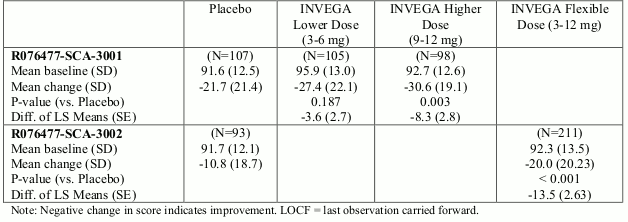
The efficacy of INVEGA in the acute treatment of psychotic or manic symptoms of schizoaffective disorder was established in two placebo-controlled, 6-week trials in non-elderly adult subjects. Enrolled subjects 1) met DSM-IV criteria for schizoaffective disorder, as confirmed by the Structured Clinical Interview for DSM-IV Disorders, 2) had a Positive and Negative Syndrome Scale (PANSS) total score of at least 60, and 3) had prominent mood symptoms as confirmed by a score of at least 16 on the Young Mania Rating Scale (YMRS) and/or Hamilton Rating Scale 21 for Depression (HAM-D 21). The population included subjects with schizoaffective bipolar and depressive types. In one of these trials, efficacy was assessed in 211 subjects who received flexible doses of INVEGA (3-12 mg once daily). In the other study, efficacy was assessed in 203 subjects who were assigned to one of two dose levels of INVEGA: 6 mg with the option to reduce to 3 mg (N=105) or 12 mg with the option to reduce to 9 mg (N=98) once daily. Both studies included subjects who received INVEGA either as monotherapy or in combination with mood stabilisers and/or antidepressants. Dosing was in the morning without regard to meals. Efficacy was evaluated using the PANSS.
The INVEGA group in the flexible-dose study (dosed between 3 and 12 mg/day, mean modal dose of 8.6 mg/day) and the higher dose group of INVEGA in the 2 dose-level study (12 mg/day with option to reduce to 9 mg/day) were each superior to placebo in the PANSS at 6 weeks. In the lower dose group of the 2 dose-level study (6 mg/day with option to reduce to 3 mg/day), INVEGA was not significantly different from placebo as measured by the PANSS. Only few subjects received the 3 mg dose in both studies and efficacy of this dose could not be established. Statistically superior improvements in manic symptoms as measured by YMRS (secondary efficacy scale) were observed in patients from the flexible-dose study and the INVEGA higher dose in the second study.
Taking the results of both studies together (pooled study-data), INVEGA improved the psychotic and manic symptoms of schizoaffective disorder at endpoint relative to placebo when administered either as monotherapy or in combination with mood stabilisers and/or antidepressants. However, overall the magnitude of effect in regard to PANSS and YMRS observed on monotherapy was larger than that observed with concomitant antidepressants and/or mood stabilisers. Moreover, in the pooled population, INVEGA was not efficacious in patients concomitantly receiving mood stabiliser and antidepressants in regard to the psychotic symptoms, but this population was small (30 responders in the paliperidone group and 20 responders in the placebo group). Additionally, in study SCA-3001 in the ITT population the effect on psychotic symptoms measured by PANSS was clearly less pronounced and not reaching statistical significance for patients receiving concomitantly mood stabilisers and/or antidepressants. An effect of INVEGA on depressive symptoms was not demonstrated in these studies, but has been demonstrated in a long-term study with the long-acting injectable formulation of paliperidone (described further down in this section).
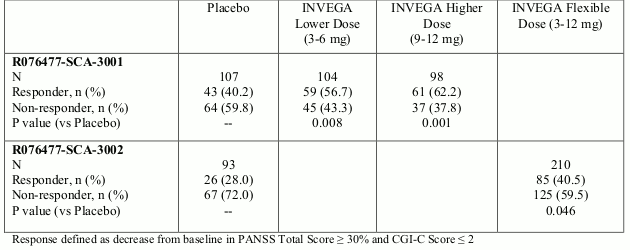
An examination of population subgroups did not reveal any evidence of differential responsiveness on the basis of gender, age, or geographic region. There were insufficient data to explore differential effects based on race. Efficacy was also evaluated by calculation of treatment response (defined as decrease in PANSS Total Score ≥30% and CGI-C Score ≤2) as a secondary endpoint.
Schizoaffective Disorder Studies: Primary Efficacy Parameter, PANSS Total Score Change from Baseline from Studies R076477-SCA-3001 and R076477-SCA-3002: Intent-to-Treat Analysis Set:
Schizoaffective Disorder Studies: Secondary Efficacy Parameter, Proportion of Subjects with Responder Status at LOCF End Point: Studies R076477-SCA-3001 and R076477-SCA-3002: Intent-to-Treat Analysis Set:
In a long-term trial designed to assess the maintenance of effect, the long-acting injectable formulation of paliperidone was significantly more effective than placebo in maintaining symptom control and delaying relapse of psychotic, manic, and depressive symptoms of schizoaffective disorder. After having been successfully treated for an acute psychotic or mood episode for 13 weeks and stabilised for an additional 12 weeks with the long-acting injectable formulation of paliperidone (doses ranging from 50 to 150 mg) patients were then randomised to a 15-month double-blind relapse prevention period of the study to either continue on the long-acting injectable formulation of paliperidone or on placebo until they experienced a relapse of schizoaffective symptoms. The study showed a significantly longer time to relapse in patients treated with the long-acting injectable formulation of paliperidone compared to placebo (p<0.001).
Paediatric population
The European Medicines Agency has waived the obligation to submit the results of studies with INVEGA in all subsets of the paediatric population in the treatment of schizoaffective disorders. See section 4.2 for information on paediatric use.
The efficacy of INVEGA in the treatment of schizophrenia in adolescents between 12 and 14 years old has not been established.
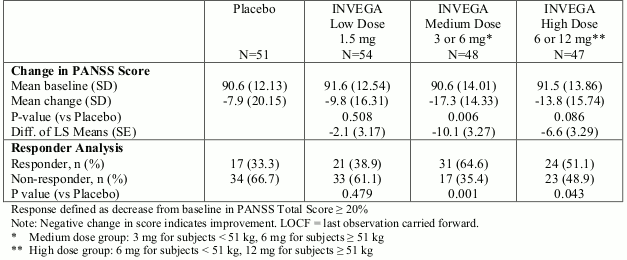
The efficacy of INVEGA in adolescent subjects with schizophrenia (INVEGA N=149, placebo N=51) was studied in a randomised, double-blind, placebo-controlled, 6-week study using a fixed-dose weight-based treatment group design over the dose range of 1.5 mg/day to 12 mg/day. Subjects were 12-17 years of age and met DSM-IV criteria for schizophrenia. Efficacy was evaluated using PANSS. This study demonstrated the efficacy of INVEGA of the medium dose group in adolescent subjects with schizophrenia. Secondary by dose analysis demonstrated the efficacy of 3 mg, 6 mg, and 12 mg dose given once daily.
Adolescent Schizophrenia Study: R076477-PSZ-3001: 6-week, fixed-dose, placebo-controlled Intent-to-Treat Analysis Set. LOCF endpoint change from baseline:
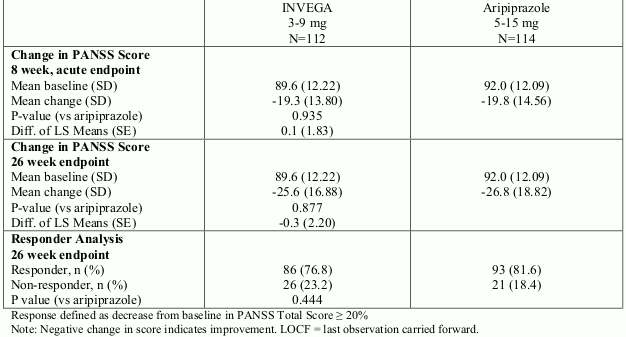
Efficacy of INVEGA over a flexible dose range of 3 mg/day to 9 mg/day in adolescent subjects (12 years and older) with schizophrenia (INVEGA N=112, aripiprazole N=114) was also evaluated in a randomised, double-blind, active-controlled study that included an 8-week, double-blind acute phase and an 18-week, double-blind maintenance phase. The changes in PANSS total scores from baseline to week 8 and week 26 were numerically similar between the INVEGA and aripiprazole treatment groups. In addition, the difference in the percentage of patients demonstrating ≥20% improvement in PANSS total score at week 26 between the two treatment groups was numerically similar.
Adolescent Schizophrenia Study: R076477-PSZ-3003: 26-week, flexible-dose, active-controlled Intent-to-Treat Analysis Set. LOCF endpoint change from baseline:
Pharmacokinetic properties
The pharmacokinetics of paliperidone following INVEGA administration are dose proportional within the available dose range.
Absorption
Following a single dose, INVEGA exhibits a gradual ascending release rate, allowing the plasma concentrations of paliperidone to steadily rise to reach peak plasma concentration (Cmax) approximately 24 hours after dosing. With once-daily dosing of INVEGA, steady-state concentrations of paliperidone are attained within 4-5 days of dosing in most subjects.
Paliperidone is the active metabolite of risperidone. The release characteristics of INVEGA result in minimal peak-trough fluctuations as compared to those observed with immediate-release risperidone (fluctuation index 38% versus 125%).
The absolute oral bioavailability of paliperidone following INVEGA administration is 28% (90% CI of 23%-33%).
Administration of paliperidone prolonged-release tablets with a standard high-fat/high-caloric meal increases Cmax and AUC of paliperidone by up to 50-60% compared with administration in the fasting state.
Distribution
Paliperidone is rapidly distributed. The apparent volume of distribution is 487 L. The plasma protein binding of paliperidone is 74%. It binds primarily to α1-acid glycoprotein and albumin.
Biotransformation and elimination
One week following administration of a single oral dose of 1 mg immediate-release 14C-paliperidone, 59% of the dose was excreted unchanged into urine, indicating that paliperidone is not extensively metabolised by the liver. Approximately 80% of the administered radioactivity was recovered in urine and 11% in the faeces. Four metabolic pathways have been identified in vivo, none of which accounted for more than 6.5% of the dose: dealkylation, hydroxylation, dehydrogenation, and benzisoxazole scission. Although in vitro studies suggested a role for CYP2D6 and CYP3A4 in the metabolism of paliperidone, there is no evidence in vivo that these isozymes play a significant role in the metabolism of paliperidone. Population pharmacokinetics analyses indicated no discernible difference on the apparent clearance of paliperidone after administration of INVEGA between extensive metabolisers and poor metabolisers of CYP2D6 substrates. In vitro studies in human liver microsomes showed that paliperidone does not substantially inhibit the metabolism of medicines metabolised by cytochrome P450 isozymes, including CYP1A2, CYP2A6, CYP2C8/9/10, CYP2D6, CYP2E1, CYP3A4, and CYP3A5. The terminal elimination half-life of paliperidone is about 23 hours.
In vitro studies have shown that paliperidone is a P-gp substrate and a weak inhibitor of P-gp at high concentrations. No in vivo data are available and the clinical relevance is unknown.
Hepatic impairment
Paliperidone is not extensively metabolised in the liver. In a study in subjects with moderate hepatic impairment (Child-Pugh class B), the plasma concentrations of free paliperidone were similar to those of healthy subjects. No data are available in patients with severe hepatic impairment (Child-Pugh class C).
Renal impairment
Elimination of paliperidone decreased with decreasing renal function. Total clearance of paliperidone was reduced in subjects with impaired renal function by 32% in mild (Creatinine Clearance [CrCl] = 50 to <80 mL/min), 64% in moderate (CrCl = 30 to <50 mL/min), and 71% in severe (CrCl = <30 mL/min) renal impairment. The mean terminal elimination half-life of paliperidone was 24, 40, and 51 hours in subjects with mild, moderate, and severe renal impairment, respectively, compared with 23 hours in subjects with normal renal function (CrCl ≥80 mL/min).
Elderly
Data from a pharmacokinetic study in elderly subjects (≥65 years of age, n=26) indicated that the apparent steady-state clearance of paliperidone following INVEGA administration was 20% lower compared to that of adult subjects (18-45 years of age, n=28). However, there was no discernable effect of age in the population pharmacokinetic analysis involving schizophrenia subjects after correction of age-related decreases in CrCl.
Adolescents
Paliperidone systemic exposure in adolescent subjects (15 years and older) was comparable to that in adults. In adolescents weighing <51 kg, a 23% higher exposure was observed than in adolescents weighing ≥51 kg. Age alone did not influence the paliperidone exposure.
Race
Population pharmacokinetics analysis revealed no evidence of race-related differences in the pharmacokinetics of paliperidone following INVEGA administration.
Gender
The apparent clearance of paliperidone following INVEGA administration is approximately 19% lower in women than men. This difference is largely explained by differences in lean body mass and creatinine clearance between men and women.
Smoking status
Based on in vitro studies utilising human liver enzymes, paliperidone is not a substrate for CYP1A2; smoking should, therefore, not have an effect on the pharmacokinetics of paliperidone. A population pharmacokinetic analysis showed a slightly lower exposure to paliperidone in smokers compared with non-smokers. The difference is unlikely to be of clinical relevance, though.
Preclinical safety data
Repeat-dose toxicity studies of paliperidone in rat and dog showed mainly pharmacological effects, such as sedation and prolactin-mediated effects on mammary glands and genitals. Paliperidone was not teratogenic in rat and rabbit. In rat reproduction studies using risperidone, which is extensively converted to paliperidone in rats and humans, a reduction was observed in the birth weight and survival of the offspring. Other dopamine antagonists, when administered to pregnant animals, have caused negative effects on learning and motor development in the offspring. Paliperidone was not genotoxic in a battery of tests. In oral carcinogenicity studies of risperidone in rats and mice, increases in pituitary gland adenomas (mouse), endocrine pancreas adenomas (rat), and mammary gland adenomas (both species) were seen. These tumours can be related to prolonged dopamine D2 antagonism and hyperprolactinemia. The relevance of these tumour findings in rodents in terms of human risk is unknown.
In a 7-week juvenile toxicity study in rats administered oral doses of paliperidone up to 2.5 mg/kg/day, corresponding to an exposure approximately equal to the clinical exposure based on AUC, no effects on growth, sexual maturation and reproductive performance were observed. Paliperidone did not impair the neurobehavioural development in males at doses up to 2.5 mg/kg/day. At 2.5 mg/kg/day in females, an effect on learning and memory was observed. This effect was not observed after discontinuation of treatment. In a 40-week juvenile toxicity study in dogs with oral doses of risperidone (which is extensively converted to paliperidone) up to 5 mg/kg/day, effects on sexual maturation, long bone growth and femur mineral density were observed from 3 times the clinical exposure based on AUC.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.