INVIRASE Film-coated tablet Ref.[8793] Active ingredients: Saquinavir
Source: European Medicines Agency (EU) Revision Year: 2018 Publisher: Roche Registration GmbH, Emil-Barell-Strasse 1, 79639 Grenzach-Wyhlen, Germany
Contraindications
Invirase is contraindicated in patients with:
- hypersensitivity to the active substance or to any of the excipients listed in section 6.1
- decompensated liver disease (see section 4.4)
- congenital or documented acquired QT prolongation
- electrolyte disturbances, particularly uncorrected hypokalaemia
- clinically relevant bradycardia
- clinically relevant heart failure with reduced left-ventricular ejection fraction
- previous history of symptomatic arrhythmias
- concurrent therapy with any of the following drugs, which may interact and result in potentially life-threatening undesirable effects (see sections 4.4, 4.5 and 4.8):
- drugs that prolong the QT and/or PR interval (see sections 4.4 and 4.5)
- midazolam administered orally (for caution on parenterally administered midazolam, see section 4.5), triazolam (potential for prolonged or increased sedation, respiratory depression)
- simvastatin, lovastatin (increased risk of myopathy including rhabdomyolysis)
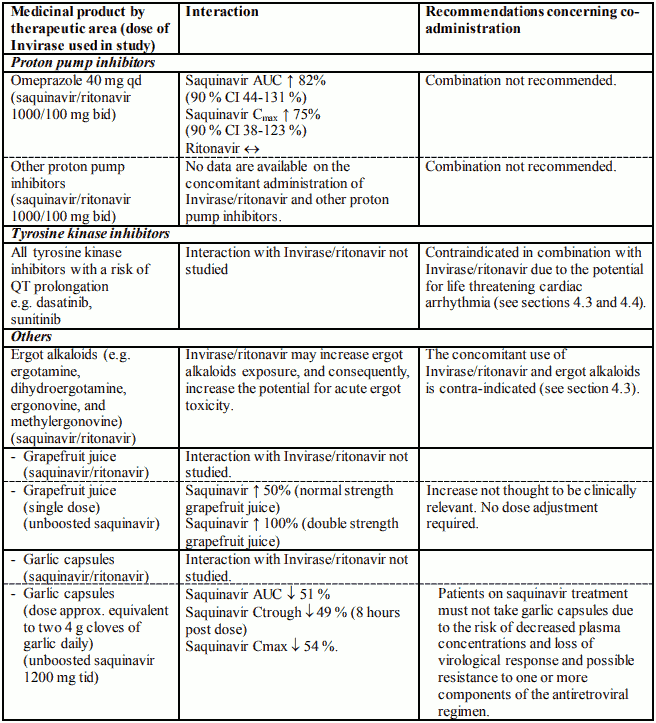
- ergot alkaloids (e.g. ergotamine, dihydroergotamine, ergonovine, and methylergonovine) (potential for acute ergot toxicity)
- rifampicin (risk of severe hepatocellular toxicity) (see sections 4.4, 4.5, and 4.8)
- quetiapine (risk of coma, see section 4.5).
- lurasidone (potential for serious and/or life-threatening reactions, see section 4.5)
Special warnings and precautions for use
Considerations when initiating Invirase therapy
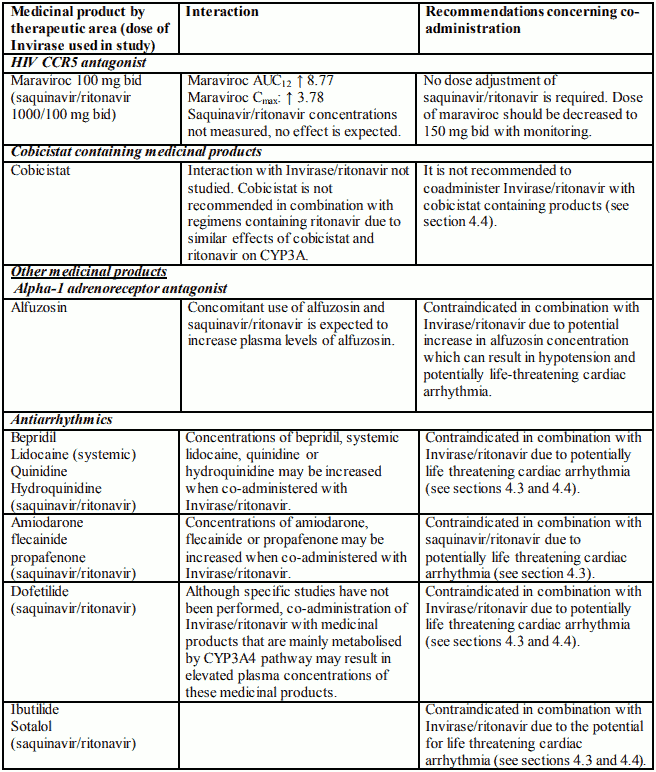
Invirase should not be given as the sole protease inhibitor. Invirase should only be given in combination with ritonavir (see section 4.2). Invirase is not recommended for use in combination with cobicistat as dosing recommendations for this combination have not been established.
Patients should be informed that saquinavir is not a cure for HIV infection and that they may continue to acquire illnesses associated with advanced HIV infection, including opportunistic infections. While effective viral suppression with antiretroviral therapy has been proven to substantially reduce the risk of sexual transmission, a residual risk cannot be excluded. Precautions to prevent transmission should be taken in accordance with national guidelines.
Patients should also be advised that they might experience undesirable effects associated with coadministered medications.
Cardiac conduction and repolarisation abnormalities
Dose-dependent prolongations of QT and PR intervals have been observed in healthy volunteers receiving ritonavir-boosted Invirase (see section 5.1). Concomitant use of ritonavir-boosted Invirase with other medicinal products that prolong the QT and/or PR interval is therefore contraindicated (see section 4.3).
Since the magnitude of QT and PR prolongation increases with increasing concentrations of saquinavir, the recommended dose of ritonavir-boosted Invirase should not be exceeded. Ritonavirboosted Invirase at a dose of 2000 mg once daily with ritonavir 100 mg once daily has not been studied with regard to the risk of QT prolongation and is not recommended. Other medicinal products known to increase the plasma concentration of ritonavir-boosted Invirase should be used with caution.
Women and elderly patients may be more susceptible to drug-associated effects on the QT and/or PR interval.
Clinical Management
Consideration should be given for performing baseline and follow-up electrocardiograms after initiation of treatment, e.g. in patients taking concomitant medication known to increase the exposure of saquinavir (see section 4.5). If signs or symptoms suggesting cardiac arrhythmia occur, continuous monitoring of ECG should be performed. Ritonavir-boosted Invirase should be discontinued if arrhythmias are demonstrated, or if prolongation occurs in the QT or PR interval.
Patients initiating therapy with ritonavir-boosted Invirase:
- An ECG should be performed on all patients prior to initiation of treatment: patients with a QT interval >450 msec should not use ritonavir-boosted Invirase. For patients with a QT interval <450 msec, an on treatment ECG is recommended.
- For treatment-naïve patients initiating treatment with Invirase/ritonavir 500/100 mg two times daily for the first 7 days of treatment followed by Invirase 1000 mg two times daily with ritonavir 100 mg two times daily after 7 days and with a baseline QT interval <450 msec, an on-treatment ECG is suggested after approximately 10 days of therapy.
- Patients demonstrating a subsequent increase in QT-interval to >480 msec or prolongation over pre-treatment by >20 msec should discontinue ritonavir-boosted Invirase.
Patients stable on ritonavir-boosted Invirase and requiring concomitant medication with potential to increase the exposure of saquinavir or patients on medication with potential to increase the exposure of saquinavir and requiring concomitant ritonavir-boosted Invirase where no alternative therapy is available and the benefits outweigh the risks:
- An ECG should be performed prior to initiation of the concomitant therapy: patients with a QT interval >450 msec should not initiate the concomitant therapy (see section 4.5).
- For patients with a baseline QT interval <450 msec, an on-treatment ECG should be performed. For patients demonstrating a subsequent increase in QT-interval to >480 msec or increase by >20 msec after commencing concomitant therapy, the physician should use best clinical judgment to discontinue either ritonavir-boosted Invirase or the concomitant therapy or both.
Essential Patient Information
Prescribers must ensure that patients are fully informed regarding the following information on cardiac conduction and repolarisation abnormalities:
- Patients initiating therapy with ritonavir boosted Invirase should be warned of the arrhythmogenic risk associated with QT and PR prolongation and told to report any sign or symptom suspicious of cardiac arrhythmia (e.g., chest palpitations, syncope, presyncope) to their physician.
- Physicians should enquire about any known familial history of sudden death at a young age as this may be suggestive of congenital QT prolongation.
- Patients should be advised of the importance not to exceed the recommended dose.
- Each patient (or patient's caregiver) should be reminded to read the Package Leaflet included in the Invirase Package.
Liver disease
The safety and efficacy of saquinavir/ritonavir has not been established in patients with significant underlying liver disorders, therefore saquinavir/ritonavir should be used cautiously in this patient population. Invirase/ritonavir is contraindicated in patients with decompensated liver disease (see section 4.3). Patients with chronic hepatitis B or C and treated with combination antiretroviral therapy are at an increased risk for severe and potentially fatal hepatic adverse events. In case of concomitant antiviral therapy for hepatitis B or C, please refer also to the relevant product information for these medicinal products.
Patients with pre-existing liver dysfunction including chronic active hepatitis have an increased frequency of liver function abnormalities during combination antiretroviral therapy and should be monitored according to standard practice. If there is evidence of worsening liver disease in such patients, interruption or discontinuation of treatment must be considered.
No dosage adjustment seems warranted for patients with moderate hepatic impairment based on limited data. Close monitoring of safety (including signs of cardiac arrhythmia) and of virologic response is recommended due to increased variability of the exposure in this population (see sections 4.2 and 5.2). There have been reports of exacerbation of chronic liver dysfunction, including portal hypertension, in patients with underlying hepatitis B or C, cirrhosis and other underlying liver abnormalities.
Renal impairment
Renal clearance is only a minor elimination pathway, the principal route of metabolism and excretion for saquinavir being via the liver. Therefore, no initial dose adjustment is necessary for patients with renal impairment. However, patients with severe renal impairment have not been studied and caution should be exercised when prescribing saquinavir/ritonavir in this population.
Patients with chronic diarrhoea or malabsorption
No information on boosted saquinavir and only limited information on the safety and efficacy of unboosted saquinavir is available for patients suffering from chronic diarrhoea or malabsorption. It is unknown whether patients with such conditions could receive subtherapeutic saquinavir levels.
Paediatric population
The safety and activity of saquinavir boosted with ritonavir in HIV-infected patients less than 2 years have not been established. No dose recommendations for paediatric patients ≥2 years of age could be established that are both effective and below thresholds of concern for QT and PR interval prolongation. Therefore, use in this population is not recommended.
Adults over 60 years
The experience with Invirase in adults over 60 years is limited. Elderly patients may be more susceptible to drug-associated effects on the QT and/or PR interval.
Lactose intolerance
Invirase 500 mg film-coated tablets contain lactose. Patients with rare hereditary problems of galactose intolerance, the Lapp lactase deficiency or glucose-galactose malabsorption should not take this medicine.
Patients with haemophilia
There have been reports of increased bleeding, including spontaneous skin haematomas and haemarthroses, in haemophiliac patients type A and B treated with protease inhibitors. In some patients additional factor VIII was given. In more than half of the reported cases, treatment with protease inhibitors was continued or reintroduced if treatment had been discontinued. A causal relationship has been evoked, although the mechanism of action has not been elucidated. Haemophiliac patients should therefore be made aware of the possibility of increased bleeding.
Weight and metabolic parameters
An increase in weight and in levels of blood lipids and glucose may occur during antiretroviral therapy. Such changes may in part be linked to disease control and lifestyle. For lipids, there is in some cases evidence for a treatment effect, while for weight gain there is no strong evidence relating this to any particular treatment. For monitoring of blood lipids and glucose reference is made to established HIV treatment guidelines. Lipid disorders should be managed as clinically appropriate.
Osteonecrosis
Although the aetiology is considered to be multifactorial (including corticosteroid use, alcohol consumption, severe immunosuppression, higher body mass index), cases of osteonecrosis have been reported particularly in patients with advanced HIV–disease and/or long-term exposure to combination antiretroviral therapy (CART). Patients should be advised to seek medical advice if they experience joint aches and pain, joint stiffness or difficulty in movement.
Immune Reactivation Syndrome
In HIV-infected patients with severe immune deficiency at the time of institution of combination antiretroviral therapy (CART), an inflammatory reaction to asymptomatic or residual opportunistic pathogens may arise and cause serious clinical conditions, or aggravation of symptoms. Typically, such reactions have been observed within the first few weeks or months of initiation of CART. Relevant examples are cytomegalovirus retinitis, generalised and/or focal mycobacterial infections, and Pneumocystis carinii pneumonia. Any inflammatory symptoms should be evaluated and treatment instituted when necessary.
Autoimmune disorders (such as Graves' disease and autoimmune hepatitis) have also been reported to occur in the setting of immune reactivation; however, the reported time to onset is more variable and can occur many months after initiation of treatment.
CYP3A4 Interactions
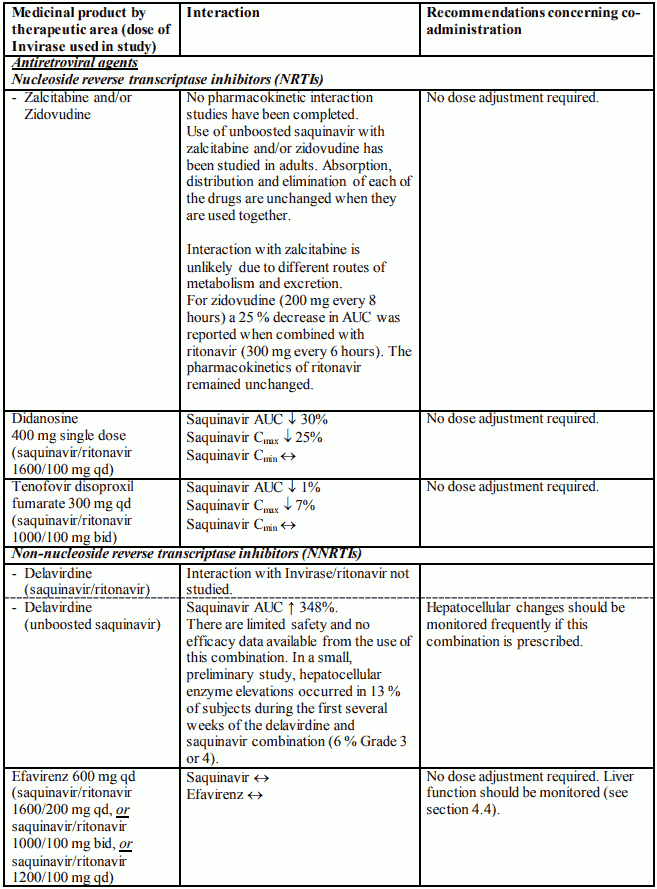
Saquinavir could interact and modify the pharmacokinetics of other drugs that are substrates for CYP3A4 and/or P-gp and should be used with caution. Conversely, other drugs that induce CYP3A4 may also reduce saquinavir plasma concentrations. Monitoring of saquinavir plasma concentration might be indicated. See table 1, section 4.5, for drugs known and/or having the potential to interact with saquinavir and specific recommendations.
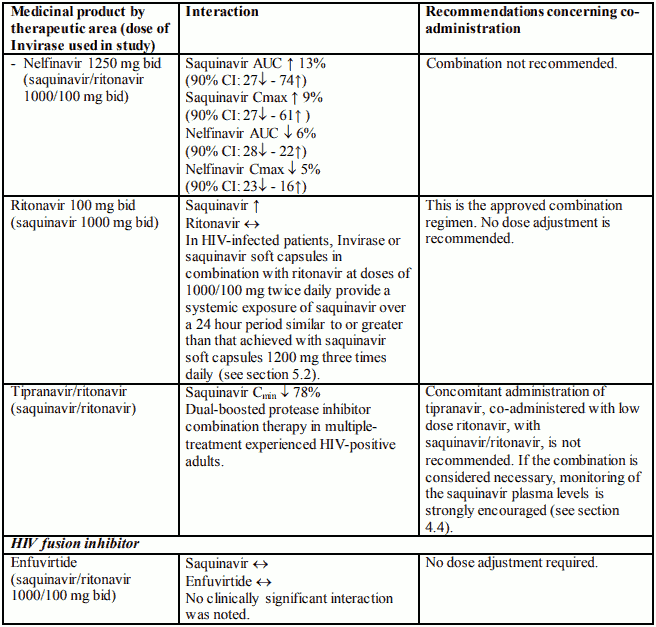
Interaction with ritonavir
The recommended dose of Invirase and ritonavir is 1000 mg Invirase plus 100 mg ritonavir twice daily. Higher doses of ritonavir have been shown to be associated with an increased incidence of adverse events. Co-administration of saquinavir and ritonavir has led to severe adverse events, mainly diabetic ketoacidosis and liver disorders, especially in patients with preexisting liver disease.
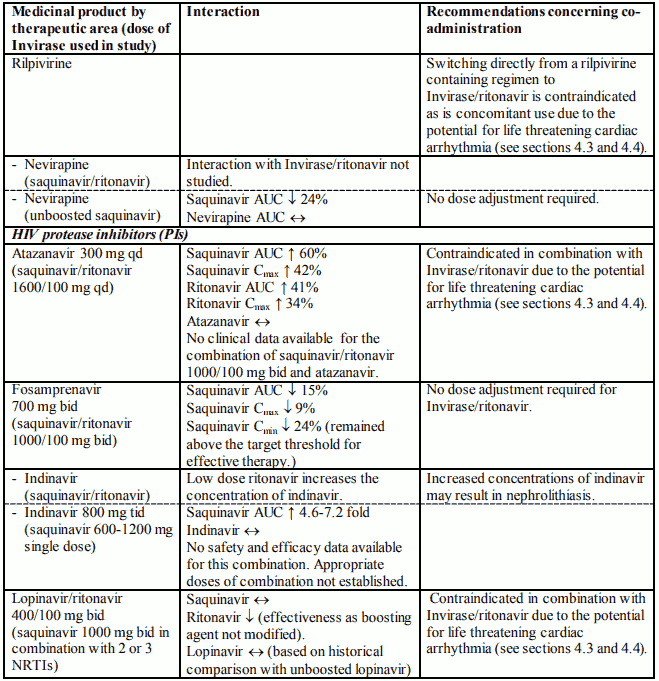
Interaction with tipranavir
Concomitant use of boosted saquinavir and tipranavir, co-administered with low dose ritonavir in a dual-boosted regimen, results in a significant decrease in saquinavir plasma concentrations (see section 4.5). Therefore, the co-administration of boosted saquinavir and tipranavir, co-administered with low dose ritonavir, is not recommended.
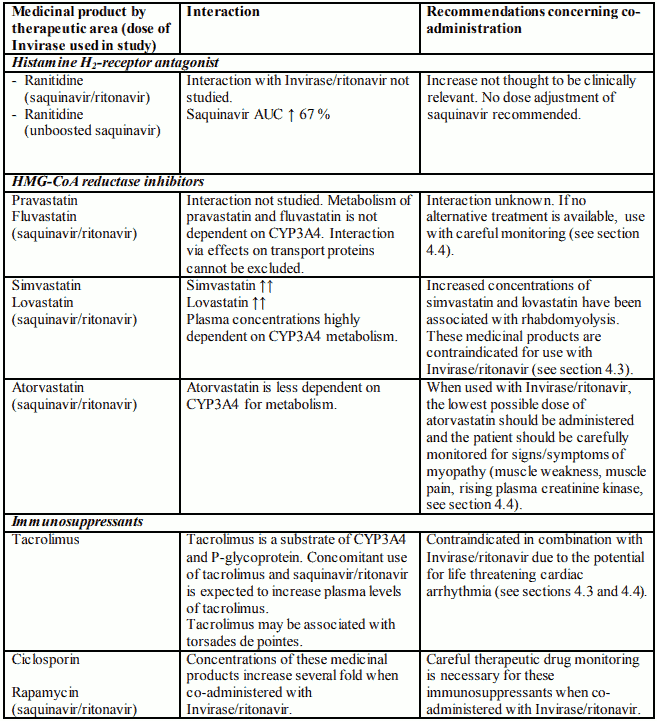
Interaction with HMG-CoA reductase inhibitors
Caution must be exercised if Invirase/ritonavir is used concurrently with atorvastatin, which is metabolised to a lesser extent by CYP3A4. In this situation a reduced dose of atorvastatin should be considered. If treatment with a HMG-CoA reductase inhibitor is indicated, pravastatin or fluvastatin is recommended with careful monitoring (see section 4.5).
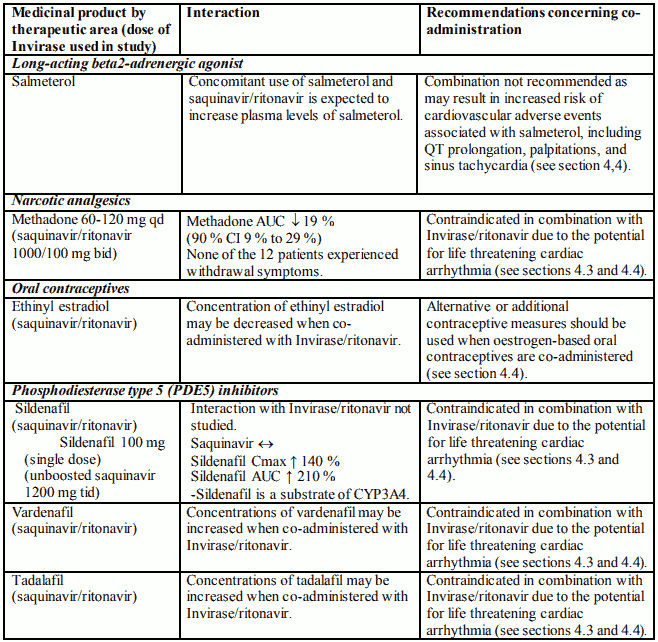
Oral contraceptives
Because concentration of ethinyl estradiol may be decreased when coadministered with Invirase/ritonavir, alternative or additional contraceptive measures should be used when oestrogen-based oral contraceptives are co-administered (see section 4.5).
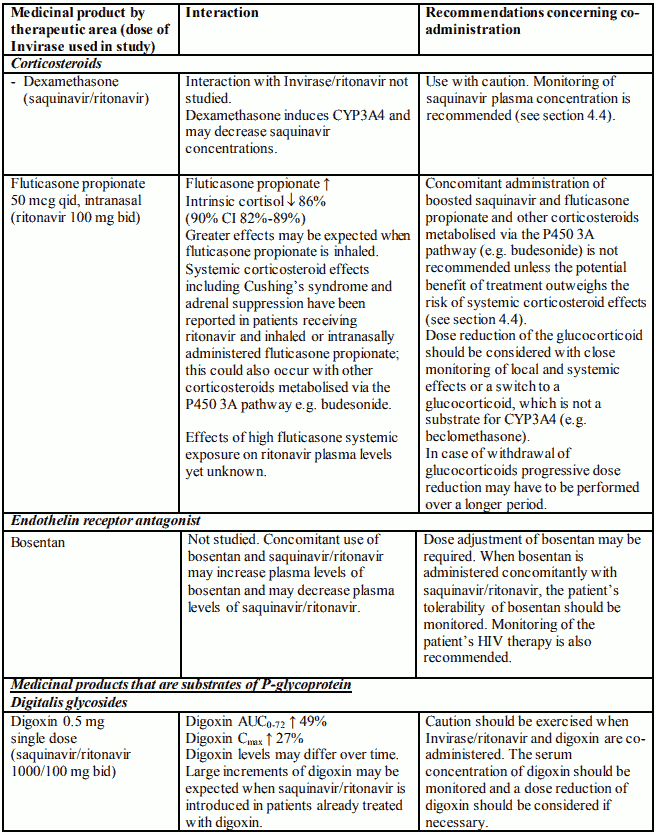
Glucocorticoids
Concomitant use of boosted saquinavir and fluticasone or other glucocorticoids that are metabolised by CYP3A4 is not recommended unless the potential benefit of treatment outweighs the risk of systemic corticosteroid effects, including Cushing's syndrome and adrenal suppression (see section 4.5).
Interaction with efavirenz
The combination of saquinavir and ritonavir with efavirenz has been shown to be associated with an increased risk of liver toxicity; liver function should be monitored when saquinavir and ritonavir are co-administered with efavirenz. No clinically significant alterations of either saquinavir or efavirenz concentration were noted in studies in healthy volunteers or in HIVinfected patients (see section 4.5).
Interaction with other medicinal products and other forms of interaction
Most drug interaction studies with saquinavir have been completed with unboosted Invirase or unboosted saquinavir soft capsules. A limited number of studies have been completed with ritonavir boosted Invirase or ritonavir boosted saquinavir soft capsules.
Observations from drug interaction studies done with unboosted saquinavir might not be representative of the effects seen with saquinavir/ritonavir therapy. Furthermore, results seen with saquinavir soft capsules may not predict the magnitude of these interactions with Invirase/ritonavir.
The metabolism of saquinavir is mediated by cytochrome P450, with the specific isoenzyme CYP3A4 responsible for 90% of the hepatic metabolism. Additionally, in vitro studies have shown that saquinavir is a substrate and an inhibitor for P-glycoprotein (P-gp). Therefore, medicinal products that either share this metabolic pathway or modify CYP3A4 and/or P-gp activity (see "Other potential interactions") may modify the pharmacokinetics of saquinavir. Similarly, saquinavir might also modify the pharmacokinetics of other medicinal products that are substrates for CYP3A4 or P-gp.
Ritonavir can affect the pharmacokinetics of other medicinal products because it is a potent inhibitor of CYP3A4 and P-gp. Therefore, when saquinavir is co-administered with ritonavir, consideration should be given to the potential effects of ritonavir on other medicinal products (see the Summary of Product Characteristics for Norvir).
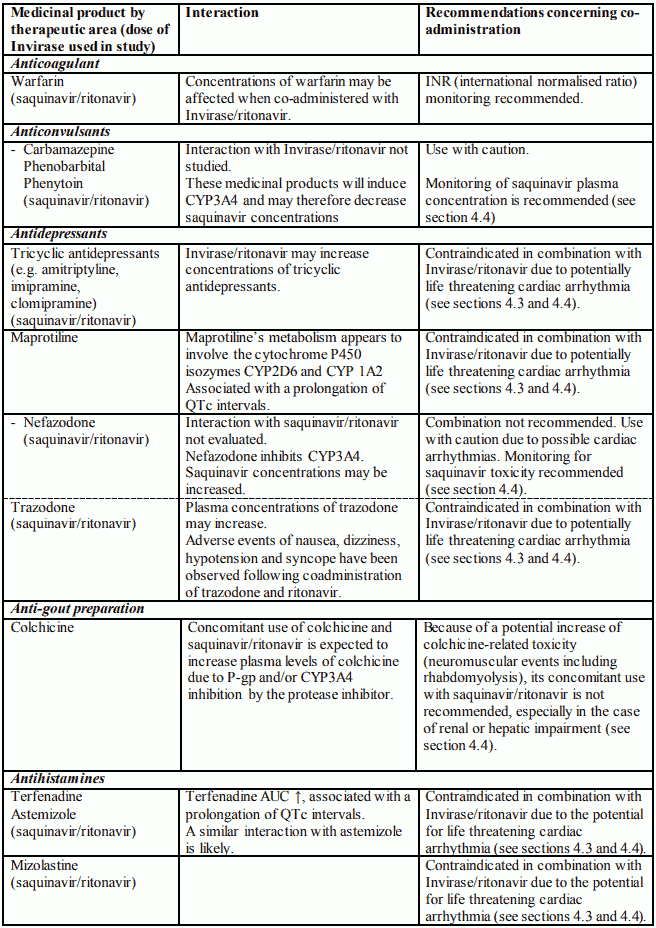
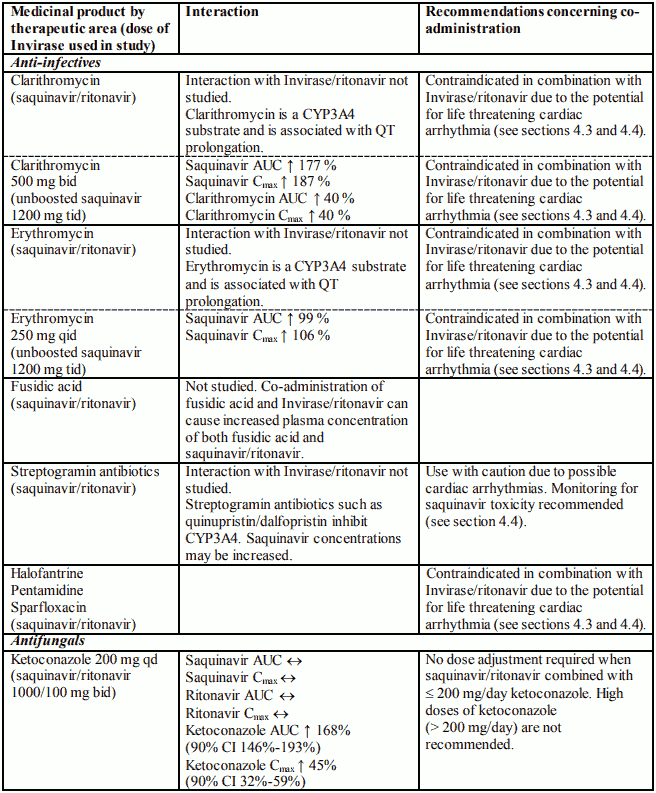
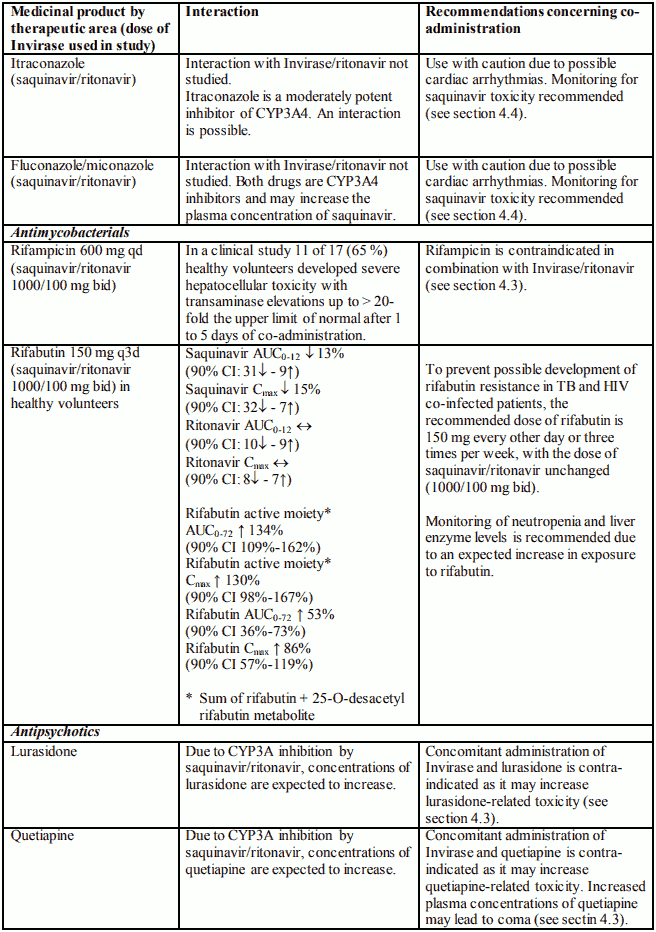
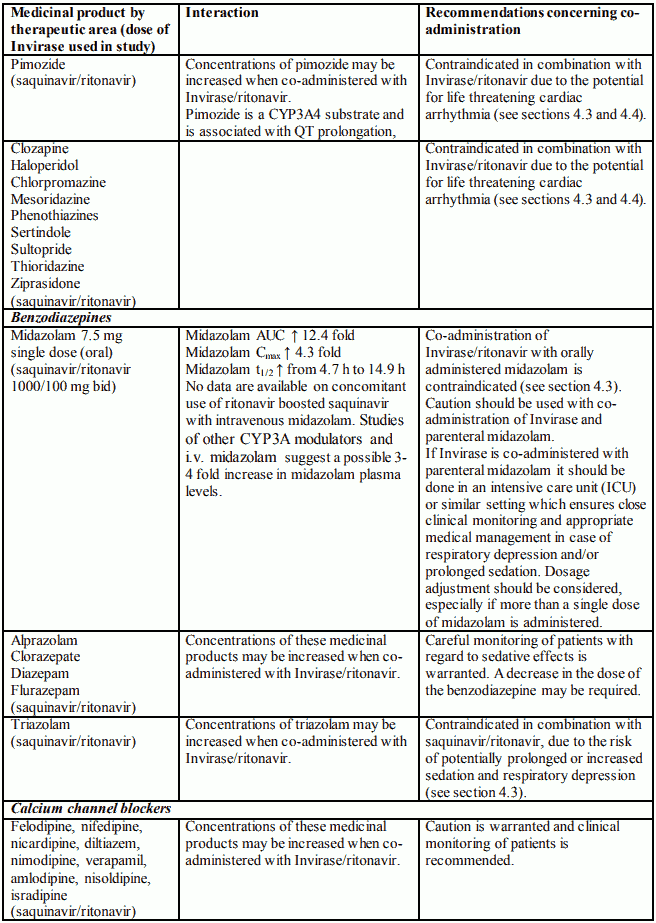
Based on the finding of dose-dependent prolongations of QT and PR intervals in healthy volunteers receiving Invirase/ritonavir (see sections 4.3, 4.4 and 5.1), additive effects on QT and PR interval prolongation may occur. Therefore, concomitant use of ritonavir-boosted Invirase with other medicinal products that prolong the QT and/or PR interval is contraindicated. The combination of Invirase/ritonavir with drugs known to increase the exposure of saquinavir is not recommended and should be avoided when alternative treatment options are available. If concomitant use is deemed necessary because the potential benefit to the patient outweighs the risk, particular caution is warranted (see section 4.4; for information on individual drugs, see Table 1).
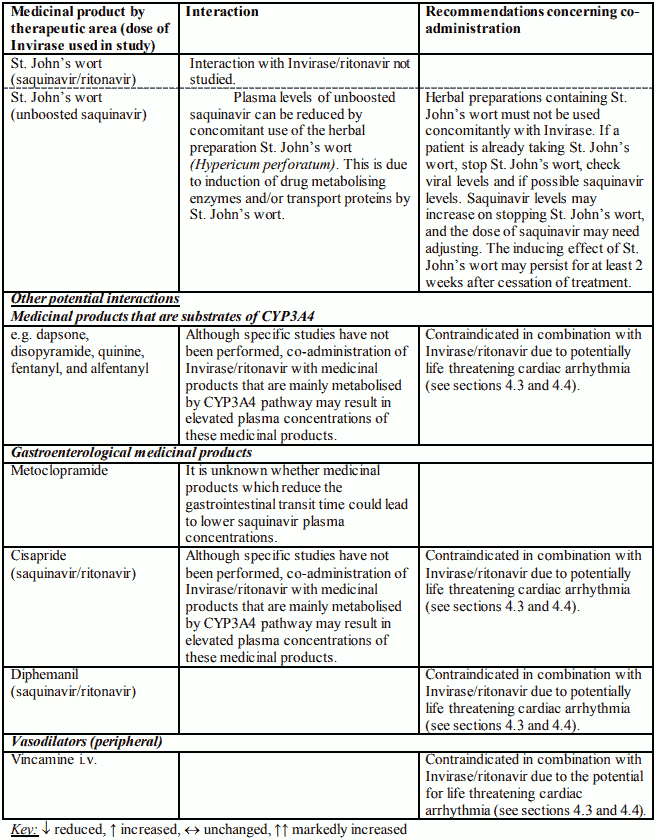
Table 1. Interactions and dose recommendations with other medicinal products:
Fertility, pregnancy and lactation
Pregnancy
Evaluation of experimental animal studies does not indicate direct or indirect harmful effects with respect to the development of the embryo or foetus, the course of gestation and peri- and post-natal development. Clinical experience in pregnant women is limited: Congenital malformations, birth defects and other disorders (without a congenital malformation) have been reported rarely in pregnant women who had received saquinavir in combination with other antiretroviral agents.
However, so far the available data are insufficient and do not identify specific risks for the unborn child. Saquinavir should be used during pregnancy only if the potential benefit justifies the potential risk to the foetus (see section 5.3).
Breast-feeding
There are no laboratory animal or human data available on secretion of saquinavir in breast milk. The potential for adverse reactions to saquinavir in nursing infants cannot be assessed, and therefore, breast-feeding should be discontinued prior to receiving saquinavir. It is recommended that HIV-infected women do not breast feed their infants under any circumstances in order to avoid transmission of HIV.
Effects on ability to drive and use machines
Invirase may have a minor influence on the ability to drive and use machines. Dizziness, fatigue and visual impairment have been reported during treatment with Invirase. No studies on the effects on the ability to drive and use machines have been performed.
Undesirable effects
a. Summary of the safety profile
Limited data is available from two clinical studies where the safety of saquinavir soft capsule (1000 mg twice daily) used in combination with low dose ritonavir (100 mg twice daily) for at least 48 weeks was studied in 311 patients.
The following adverse events with an at least possible relationship to ritonavir boosted saquinavir (i.e. adverse reactions) were reported most frequently: nausea, diarrhoea, fatigue, vomiting, flatulence, and abdominal pain.
The following adverse events were reported with the highest severity (grades 3 and 4): anaemia, diabetes mellitus, diarrhoea, nausea, vomiting and fatigue.
For comprehensive dose adjustment recommendations and drug-associated adverse reactions for ritonavir and other medicinal products used in combination with saquinavir, physicians should refer to the Summary of Product Characteristics for each of these medicinal products.
b. Tabulated list of adverse reactions
Adverse reactions from two pivotal studies of saquinavir soft capsule (1000 mg twice daily) used in combination with low dose ritonavir (100 mg twice daily) for at least 48 weeks are summarised in Table 2. Also included are serious and non-serious adverse reactions from post-marketing spontaneous reports for which a causal relationship to saquinavir cannot be excluded. Adverse reactions are presented according to the MedDRA system organ classification. The frequency groupings according to MedDRA convention are: Very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1,000 to <1/100); rare (≥1/10,000 to <1/1,000); very rare (<1/10,000); not known (frequency cannot be estimated from the available data).
Table 2. Incidences of Adverse Reactions and marked laboratory abnormalities in clinical studies and post-marketing experience in adult patients:
Blood and the lymphatic system disorders
Very common: Decreased platelet count
Common: Anaemia, decreased haemoglobin, decreased lymphocyte count, decreased white blood cell count
Uncommon: Neutropenia
Eye Disorders
Uncommon: Visual impairment
Immune System Disorders
Common: Hypersensitivity
Metabolism and nutrition disorders
Very common: Increased blood cholesterol, increased blood triglycerides
Common: Diabetes mellitus, anorexia, increased appetite
Uncommon: Decreased appetite
Psychiatric Disorders
Common: Decreased libido, sleep disorder
Nervous System Disorder
Common: Paraesthesia, peripheral neuropathy, dizziness, dysgeusia, headache
Uncommon: Somnolence, convulsions
Respiratory, thoracic and mediastinal disorders
Common: Dyspnoea
Gastrointestinal disorders
Very common: Diarrhoea, nausea
Common: Vomiting, abdominal distension, abdominal pain, upper abdominal pain, constipation, dry mouth, dyspepsia, eructation, flatulence, lip dry, loose stools
Uncommon: Pancreatitis
Hepato-biliary disorders
Very common: Increased alanine aminotransferase, increased aspartate aminotransferase, increased low density lipoprotein
Common: Increased blood bilirubin, increased blood amylase
Uncommon: Hepatitis, jaundice
Renal and urinary disorders
Common: Increased blood creatinine
Uncommon: Renal impairment
Skin and subcutaneous tissue disorders
Common: Alopecia, dry skin, eczema, lipoatrophy, pruritus, rash
Uncommon: Stevens Johnson syndrome, dermatitis bullous
Musculoskeletal and connective tissue disorders
Common: Muscle spasms
General disorders and administration site conditions
Common: Asthenia, fatigue, increased fat tissue, malaise
Uncommon: Mucosal ulceration
c. Description of selected adverse reactions
Metabolic parameters
Weight and levels of blood lipids and glucose may increase during antiretroviral therapy (see section 4.4).
There have been reports of increased bleeding, including spontaneous skin haematomas and haemarthroses, in haemophilic patients type A and B treated with protease inhibitors (see section 4.4).
Increased CPK, myalgia, myositis and rarely, rhabdomyolysis have been reported with protease inhibitors, particularly in combination with nucleoside analogues. Cases of osteonecrosis have been reported, particularly in patients with generally acknowledged risk factors, advanced HIV disease or long-term exposure to combination antiretroviral therapy (CART). The frequency of this is unknown (see section 4.4).
In HIV-infected patients with severe immune deficiency at the time of initiation of combination antiretroviral therapy (CART), an inflammatory reaction to asymptomatic or residual opportunistic infections may arise. Autoimmune disorders (such as Graves' disease and autoimmune hepatitis) have also been reported; however, the reported time to onset is more variable and these events can occur many months after initiation of treatment (see section 4.4).
d. Paediatric population
Limited safety data are available from a paediatric study (NV20911, n=18) in which the safety of saquinavir hard capsules (50 mg/kg bid, not to exceed 1000 mg bid) used in combination with low dose ritonavir oral solution (3 mg/kg bid for body weight from 5 to <15 kg, 2.5 mg/kg bid for body weight from 15 to 40 kg and 100 mg bid for body weight >40 kg) has been studied in paediatric patients aged 4 months to 6 years old.
Four patients in the study experienced five adverse events that were considered related to trial treatment. These events were vomiting (3 patients), abdominal pain (1 patient) and diarrhoea (1 patient). No unexpected adverse events were observed in this study.
Reporting of suspected adverse reactions
Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via the national reporting system listed in Appendix V.
Incompatibilities
Not applicable.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.