ISENTRESS Chewable tablet Ref.[8805] Active ingredients: Raltegravir
Source: European Medicines Agency (EU) Revision Year: 2019 Publisher: Merck Sharp & Dohme B.V., Waarderweg 39, 2031 BN Haarlem, The Netherlands
Pharmacodynamic properties
Pharmacotherapeutic group: antivirals for systemic use, other antivirals
ATC code: J05AX08
Mechanism of action
Raltegravir is an integrase strand transfer inhibitor active against the Human Immunodeficiency Virus (HIV-1). Raltegravir inhibits the catalytic activity of integrase, an HIV-encoded enzyme that is required for viral replication. Inhibition of integrase prevents the covalent insertion, or integration, of the HIV genome into the host cell genome. HIV genomes that fail to integrate cannot direct the production of new infectious viral particles, so inhibiting integration prevents propagation of the viral infection.
Antiviral activity in vitro
Raltegravir at concentrations of 31 ± 20 nM resulted in 95% inhibition (IC95) of HIV-1 replication (relative to an untreated virus-infected culture) in human T-lymphoid cell cultures infected with the cell-line adapted HIV-1 variant H9IIIB. In addition, raltegravir inhibited viral replication in cultures of mitogen-activated human peripheral blood mononuclear cells infected with diverse, primary clinical isolates of HIV-1, including isolates from 5 non-B subtypes, and isolates resistant to reverse transcriptase inhibitors and protease inhibitors. In a single-cycle infection assay, raltegravir inhibited infection of 23 HIV isolates representing 5 non-B subtypes and 5 circulating recombinant forms with IC50 values ranging from 5 to 12 nM.
Resistance
Most viruses isolated from patients failing raltegravir had high-level raltegravir resistance resulting from the appearance of two or more mutations in integrase. Most had a signature mutation at amino acid 155 (N155 changed to H), amino acid 148 (Q148 changed to H, K, or R), or amino acid 143 (Y143 changed to H, C, or R), along with one or more additional integrase mutations (e.g., L74M, E92Q, T97A, E138A/K, G140A/S, V151I, G163R, S230R). The signature mutations decrease viral susceptibility to raltegravir and addition of other mutations results in a further decrease in raltegravir susceptibility. Factors that reduced the likelihood of developing resistance included lower baseline viral load and use of other active anti-retroviral agents. Mutations conferring resistance to raltegravir generally also confer resistance to the integrase strand transfer inhibitor elvitegravir. Mutations at amino acid 143 confer greater resistance to raltegravir than to elvitegravir, and the E92Q mutation confers greater resistance to elvitegravir than to raltegravir. Viruses harbouring a mutation at amino acid 148, along with one or more other raltegravir resistance mutations, may also have clinically significant resistance to dolutegravir.
Clinical experience
The evidence of efficacy of raltegravir was based on the analyses of 96-week data from two randomised, double-blind, placebo-controlled trials (BENCHMRK 1 and BENCHMRK 2, Protocols 018 and 019) in antiretroviral treatment-experienced HIV-1 infected adult patients and the analysis of 240-week data from a randomised, double-blind, active-control trial (STARTMRK, Protocol 021) in antiretroviral treatment-naïve HIV-1 infected adult patients.
Efficacy
Treatment-experienced adult patients
BENCHMRK 1 and BENCHMRK 2 (multi-centre, randomised, double-blind, placebo-controlled trials) evaluated the safety and anti-retroviral activity of raltegravir 400 mg twice daily vs. placebo in a combination with optimised background therapy (OBT), in HIV-infected patients, 16 years or older, with documented resistance to at least 1 drug in each of 3 classes (NRTIs, NNRTIs, PIs) of anti-retroviral therapies. Prior to randomisation, OBT were selected by the investigator based on the patient's prior treatment history, as well as baseline genotypic and phenotypic viral resistance testing.
Patient demographics (gender, age and race) and baseline characteristics were comparable between the groups receiving raltegravir 400 mg twice daily and placebo. Patients had prior exposure to a median of 12 anti-retrovirals for a median of 10 years. A median of 4 ARTs was used in OBT.
Results 48 week and 96 week analyses
Durable outcomes (Week 48 and Week 96) for patients on the recommended dose raltegravir 400 mg twice daily from the pooled studies BENCHMRK 1 and BENCHMRK 2 are shown in Table 4.
Table 4. Efficacy Outcome at Weeks 48 and 96:
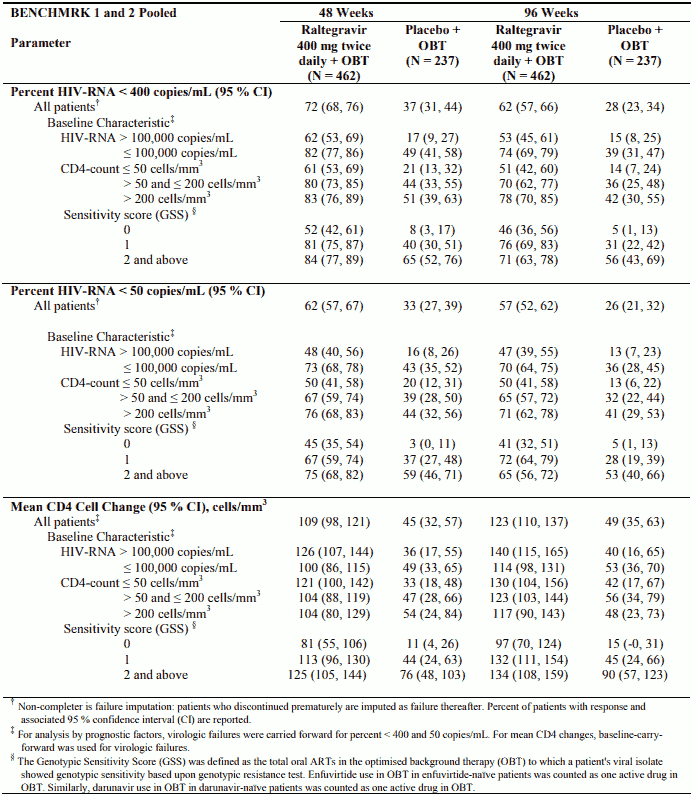
Raltegravir achieved virologic responses (using Not Completer=Failure approach) of HIV RNA <50 copies/mL in 61.7% of patients at Week 16, in 62.1% at Week 48 and in 57.0% at Week 96. Some patients experienced viral rebound between Week 16 and Week 96. Factors associated with failure include high baseline viral load and OBT that did not include at least one potent active agent.
Switch to raltegravir
The SWITCHMRK 1 & 2 (Protocols 032 & 033) studies evaluated HIV-infected patients receiving suppressive (screening HIV RNA <50 copies/mL; stable regimen >3 months) therapy with lopinavir 200 mg ( + ) ritonavir 50 mg 2 tablets twice daily plus at least 2 nucleoside reverse transcriptase inhibitors and randomised them 1:1 to continue lopinavir ( + ) ritonavir 2 tablets twice daily (n=174 and n=178, respectively) or replace lopinavir ( + ) ritonavir with raltegravir 400 mg twice daily (n=174 and n=176, respectively). Patients with a prior history of virological failure were not excluded and the number of previous antiretroviral therapies was not limited.
These studies were terminated after the primary efficacy analysis at Week 24 because they failed to demonstrate non-inferiority of raltegravir versus lopinavir ( + ) ritonavir. In both studies at Week 24, suppression of HIV RNA to less than 50 copies/mL was maintained in 84.4% of the raltegravir group versus 90.6% of the lopinavir ( + ) ritonavir group, (Non-completers = Failure). See section 4.4 regarding the need to administer raltegravir with two other active agents.
Treatment-naïve adult patients
STARTMRK (multi-centre, randomised, double-blind, active-control trial) evaluated the safety and anti-retroviral activity of raltegravir 400 mg twice daily vs. efavirenz 600 mg at bedtime, in a combination with emtricitabine ( + ) tenofovir disoproxil fumarate, in treatment-naïve HIV-infected patients with HIV RNA >5,000 copies/mL. Randomisation was stratified by screening HIV RNA level (≤50,000 copies/mL; and >50,000 copies/mL) and by hepatitis B or C status (positive or negative).
Patient demographics (gender, age and race) and baseline characteristics were comparable between the group receiving raltegravir 400 mg twice daily and the group receiving efavirenz 600 mg at bedtime.
Results 48-week and 240-week analyses
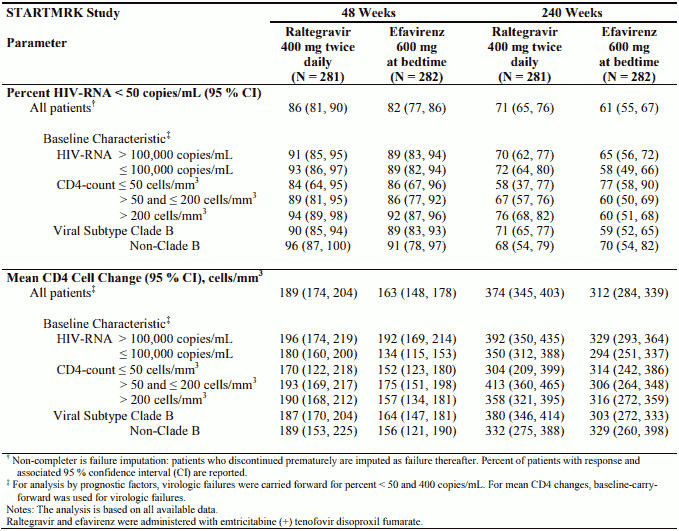
With respect to the primary efficacy endpoint, the proportion of patients achieving HIV RNA <50 copies/mL at Week 48 was 241/280 (86.1%) in the group receiving raltegravir and 230/281 (81.9%) in the group receiving efavirenz. The treatment difference (raltegravir-efavirenz) was 4.2% with an associated 95% CI of (-1.9, 10.3) establishing that raltegravir is non-inferior to efavirenz (pvalue for non-inferiority <0.001). At Week 240, the treatment difference (raltegravir-efavirenz) was 9.5% with an associated 95% CI of (1.7, 17.3). Week 48 and Week 240 outcomes for patients on the recommended dose of raltegravir 400 mg twice daily from STARTMRK are shown in Table 5.
Table 5. Efficacy Outcome at Weeks 48 and 240:
Paediatric population
Children and adolescents 2 to 18 years of age
IMPAACT P1066 is a Phase I/II open label multicenter trial to evaluate the pharmacokinetic profile, safety, tolerability, and efficacy of raltegravir in HIV infected children. This study enrolled 126 treatment experienced children and adolescents 2 to 18 years of age. Patients were stratified by age, enrolling adolescents first and then successively younger children. Patients received either the 400 mg tablet formulation (6 to 18 years of age) or the chewable tablet formulation (2 to less than 12 years of age). Raltegravir was administered with an optimised background regimen.
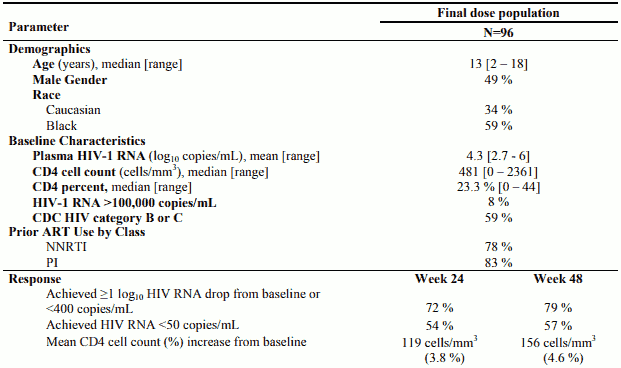
The initial dose finding stage included intensive pharmacokinetic evaluation. Dose selection was based upon achieving similar raltegravir plasma exposure and trough concentration as seen in adults, and acceptable short term safety. After dose selection, additional patients were enrolled for evaluation of long term safety, tolerability and efficacy. Of the 126 patients, 96 received the recommended dose of raltegravir (see section 4.2).
Table 6. Baseline Characteristics and Efficacy Outcomes at Weeks 24 and 48 from IMPAACT P1066 (2 to 18 years of age):
Infants and toddlers 4 weeks to less than 2 years of age
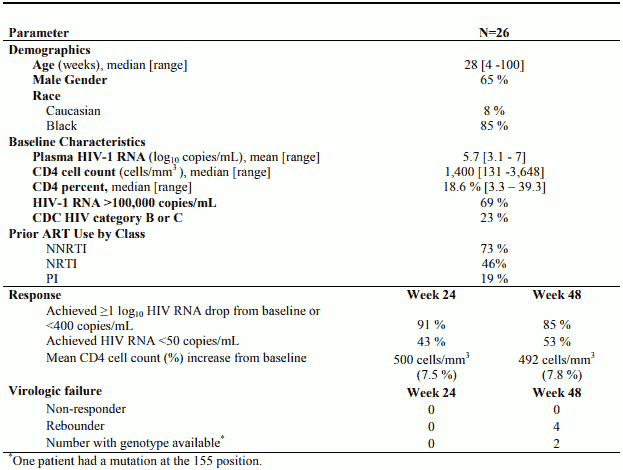
IMPAACT P1066 also enrolled HIV-infected, infants and toddlers 4 weeks to less than 2 years of age who had received prior antiretroviral therapy either as prophylaxis for prevention of mother to child transmission (PMTCT) and/or as combination antiretroviral therapy for treatment of HIV infection. Raltegravir was administered as granules for oral suspension formulation without regard to food in combination with an optimised background regimen that included lopinavir plus ritonavir in two-thirds of patients.
Table 7. Baseline Characteristics and Efficacy Outcomes at Weeks 24 and 48 from IMPAACT P1066 (4 weeks to less than 2 years of age):
Pharmacokinetic properties
Absorption
As demonstrated in healthy volunteers administered single oral doses of raltegravir in the fasted state, raltegravir is rapidly absorbed with a tmax of approximately 3 hours postdose. Raltegravir AUC and Cmax increase dose proportionally over the dose range 100 mg to 1,600 mg. Raltegravir C12hr increases dose proportionally over the dose range of 100 to 800 mg and increases slightly less than dose proportionally over the dose range 100 mg to 1,600 mg. Dose proportionality has not been established in patients.
With twice-daily dosing, pharmacokinetic steady state is achieved rapidly, within approximately the first 2 days of dosing. There is little to no accumulation in AUC and Cmax and evidence of slight accumulation in C12hr. The absolute bioavailability of raltegravir has not been established.
Raltegravir may be administered with or without food. Raltegravir was administered without regard to food in the pivotal safety and efficacy studies in HIV-infected patients. Administration of multiple doses of raltegravir following a moderate-fat meal did not affect raltegravir AUC to a clinically meaningful degree with an increase of 13% relative to fasting. Raltegravir C12hr was 66% higher and Cmax was 5% higher following a moderate-fat meal compared to fasting. Administration of raltegravir following a high-fat meal increased AUC and Cmax by approximately 2-fold and increased C12hr by 4.1-fold. Administration of raltegravir following a low-fat meal decreased AUC and Cmax by 46% and 52%, respectively; C12hr was essentially unchanged. Food appears to increase pharmacokinetic variability relative to fasting.
Overall, considerable variability was observed in the pharmacokinetics of raltegravir. For observed C12hr in BENCHMRK 1 and 2 the coefficient of variation (CV) for inter-subject variability = 212% and the CV for intra-subject variability = 122%. Sources of variability may include differences in co-administration with food and concomitant medicines.
Distribution
Raltegravir is approximately 83% bound to human plasma protein over the concentration range of 2 to 10 µM.
Raltegravir readily crossed the placenta in rats, but did not penetrate the brain to any appreciable extent.
In two studies of HIV-1 infected patients who received raltegravir 400 mg twice daily, raltegravir was readily detected in the cerebrospinal fluid. In the first study (n=18), the median cerebrospinal fluid concentration was 5.8% (range 1 to 53.5%) of the corresponding plasma concentration. In the second study (n=16), the median cerebrospinal fluid concentration was 3% (range 1 to 61%) of the corresponding plasma concentration. These median proportions are approximately 3- to 6-fold lower than the free fraction of raltegravir in plasma.
Biotransformation and excretion
The apparent terminal half-life of raltegravir is approximately 9 hours, with a shorter α-phase half-life (~1 hour) accounting for much of the AUC. Following administration of an oral dose of radiolabeled raltegravir, approximately 51 and 32% of the dose was excreted in faeces and urine, respectively. In faeces, only raltegravir was present, most of which is likely to be derived from hydrolysis of raltegravir-glucuronide secreted in bile as observed in preclinical species. Two components, namely raltegravir and raltegravir-glucuronide, were detected in urine and accounted for approximately 9 and 23% of the dose, respectively. The major circulating entity was raltegravir and represented approximately 70% of the total radioactivity; the remaining radioactivity in plasma was accounted for by raltegravir-glucuronide. Studies using isoform-selective chemical inhibitors and cDNA-expressed UDP-glucuronosyltransferases (UGT) show that UGT1A1 is the main enzyme responsible for the formation of raltegravir-glucuronide. Thus, the data indicate that the major mechanism of clearance of raltegravir in humans is UGT1A1-mediated glucuronidation.
UGT1A1 Polymorphism
In a comparison of 30 subjects with *28/*28 genotype to 27 subjects with wild-type genotype, the geometric mean ratio (90% CI) of AUC was 1.41 (0.96, 2.09) and the geometric mean ratio of C12hr was 1.91 (1.43, 2.55). Dose adjustment is not considered necessary in subjects with reduced UGT1A1 activity due to genetic polymorphism.
Special populations
Paediatric population
Based on a formulation comparison study in healthy adult volunteers, the chewable tablet and granules for oral suspension have higher oral bioavailability compared to the 400 mg tablet. In this study, administration of the chewable tablet with a high fat meal led to an average 6% decrease in AUC, 62% decrease in Cmax, and 188% increase in C12hr compared to administration in the fasted state. Administration of the chewable tablet with a high fat meal does not affect raltegravir pharmacokinetics to a clinically meaningful degree and the chewable tablet can be administered without regard to food. The effect of food on the granules for oral suspension formulation was not studied.
Table 8 displays pharmacokinetic parameters in the 400 mg tablet, the chewable tablet), and the granules for oral suspension, by body weight.
Table 8. Raltegravir Pharmacokinetic Parameters IMPAACT P1066 Following Administration of Doses in Section 4.2 (excluding neonates):
| Body weight | Formulation | Dose | N* | Geometric mean (%CV†) AUC0-12hr (μM●hr) | Geometric mean (%CV†) C12hr (nM) |
|---|---|---|---|---|---|
| ≥25 kg | Film-coated tablet | 400 mg twice daily | 18 | 14.1 (121%) | 233 (157%) |
| ≥25 kg | Chewable tablet | Weight based dosing, see dosing tables for the chewable tablet. | 9 | 22.1 (36%) | 113 (80%) |
| 11 to less than 25 kg | Chewable tablet | Weight based dosing, see dosing tables for the chewable tablet | 13 | 18.6 (68%) | 82 (123%) |
| 3 to less than 20 kg | Oral suspension | Weight based dosing, see dosing table for granules for oral suspension. | 19 | 24.5 (43%) | 113 (69%) |
* Number of patients with intensive pharmacokinetic (PK) results at the final recommended dose.
† Geometric coefficient of variation.
Elderly
There was no clinically meaningful effect of age on raltegravir pharmacokinetics in healthy subjects and patients with HIV-1 infection over the age range studied (19 to 84 years, with few individuals over the age of 65).
Gender, race and BMI
There were no clinically important pharmacokinetic differences due to gender, race or body mass index (BMI) in adults.
Renal impairment
Renal clearance of unchanged medicinal product is a minor pathway of elimination. In adults, there were no clinically important pharmacokinetic differences between patients with severe renal insufficiency and healthy subjects (see section 4.2). Because the extent to which raltegravir may be dialysable is unknown, dosing before a dialysis session should be avoided.
Hepatic impairment
Raltegravir is eliminated primarily by glucuronidation in the liver. In adults, there were no clinically important pharmacokinetic differences between patients with moderate hepatic insufficiency and healthy subjects. The effect of severe hepatic insufficiency on the pharmacokinetics of raltegravir has not been studied (see sections 4.2 and 4.4).
Preclinical safety data
Non-clinical toxicology studies, including conventional studies of safety pharmacology, repeated-dose toxicity, genotoxicity, developmental toxicity and juvenile toxicity, have been conducted with raltegravir in mice, rats, dogs and rabbits. Effects at exposure levels sufficiently in excess of clinical exposure levels indicate no special hazard for humans.
Mutagenicity
No evidence of mutagenicity or genotoxicity was observed in in vitro microbial mutagenesis (Ames) tests, in vitro alkaline elution assays for DNA breakage and in vitro and in vivo chromosomal aberration studies.
Carcinogenicity
A carcinogenicity study of raltegravir in mice did not show any carcinogenic potential. At the highest dose levels, 400 mg/kg/day in females and 250 mg/kg/day in males, systemic exposure was similar to that at the clinical dose of 400 mg twice daily. In rats, tumours (squamous cell carcinoma) of the nose/nasopharynx were identified at 300 and 600 mg/kg/day in females and at 300 mg/kg/day in males. This neoplasia could result from local deposition and/or aspiration of drug on the mucosa of the nose/nasopharynx during oral gavage dosing and subsequent chronic irritation and inflammation; it is likely that it is of limited relevance for the intended clinical use. At the NOAEL, systemic exposure was similar to that at the clinical dose of 400 mg twice daily. Standard genotoxicity studies to evaluate mutagenicity and clastogenicity were negative.
Developmental toxicity
Raltegravir was not teratogenic in developmental toxicity studies in rats and rabbits. A slight increase in incidence of supernumerary ribs, a variant in the normal developmental process, was observed in rat foetuses of dams exposed to raltegravir at approximately 4.4-fold human exposure at 400 mg twice daily based on AUC0-24hr. No development effects were seen at 3.4-fold human exposure at 400 mg twice daily based on AUC0-24hr. Similar findings were not observed in rabbits.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.