Source: European Medicines Agency (EU) Revision Year: 2020 Publisher: Roche Registration GmbH, Emil-Barell-Strasse 1, 79639, Grenzach-Wyhlen, Germany
Pharmacotherapeutic group: Antineoplastic agents, other antineoplastic agents, monoclonal antibodies
ATC code: L01XC14
Kadcyla, trastuzumab emtansine, is a HER2-targeted antibody-drug conjugate which contains the humanised anti-HER2 IgG1, trastuzumab, covalently linked to the microtubule inhibitor DM1 (a maytansine derivative) via the stable thioether linker MCC (4-[N-maleimidomethyl] cyclohexane-1-carboxylate). Emtansine refers to the MCC-DM1 complex. An average of 3.5 DM1 molecules are conjugated to each molecule of trastuzumab.
Conjugation of DM1 to trastuzumab confers selectivity of the cytotoxic agent for HER2-overexpressing tumour cells, thereby increasing intracellular delivery of DM1 directly to malignant cells. Upon binding to HER2, trastuzumab emtansine undergoes receptor-mediated internalization and subsequent lysosomal degradation, resulting in release of DM1-containing cytotoxic catabolites (primarily lysine-MCC-DM1).
Trastuzumab emtansine has the mechanisms of action of both trastuzumab and DM1:
BO27938 (KATHERINE) was a randomized, multicenter, open-label trial of 1486 patients with HER2-positive, early breast cancer with residual invasive tumor (patients who had not achieved pathological complete response (pCR)) in the breast and/or axillary lymph nodes following completion of preoperative systemic therapy that included chemotherapy and HER2-targeted therapy. Patients may have received more than one HER2-targeted therapy. Patients received radiotherapy and/or hormonal therapy concurrent with study treatment as per local guidelines. Breast tumor samples were required to show HER2 overexpression defined as 3 + IHC or ISH amplification ratio ≥2.0 determined at a central laboratory. Patients were randomized (1:1) to receive trastuzumab or trastuzumab emtansine. Randomization was stratified by clinical stage at presentation (operable vs. inoperable), hormone receptor status, preoperative HER2-directed therapy (trastuzumab, trastuzumab plus additional HER2-directed agent[s]), and pathological nodal status evaluated after preoperative therapy.
Trastuzumab emtansine was given intravenously at 3.6 mg/kg on Day 1 of a 21-day cycle. Trastuzumab was given intravenously at 6 mg/kg on Day 1 of a 21-day cycle. Patients were treated with trastuzumab emtansine or trastuzumab for a total of 14 cycles unless there was recurrence of disease, withdrawal of consent, or unacceptable toxicity, whichever occurred first. Patients who discontinued trastuzumab emtansine could complete the duration of their intended study treatment up to 14 cycles of HER2-directed therapy with trastuzumab if appropriate based on toxicity considerations and investigator discretion.
The primary efficacy endpoint of the study was Invasive Disease-Free Survival (IDFS). IDFS was defined as the time from the date of randomization to first occurrence of ipsilateral invasive breast tumor recurrence, ipsilateral local or regional invasive breast cancer recurrence, distant recurrence, contralateral invasive breast cancer, or death from any cause. Additional endpoints included IDFS including second primary non-breast cancer, disease-free survival (DFS), overall survival (OS), and distant recurrence-free interval (DRFI).
Patient demographics and baseline tumor characteristics were balanced between treatment arms. The median age was approximately 49 years (range 23-80 years), 72.8% were White, 8.7% were Asian and 2.7% were Black or African American. All but 5 patients were women; 3 men were included in the trastuzumab arm and 2 in the trastuzumab emtansine arm. 22.5 percent of patients were enrolled in North America, 54.2% in Europe and 23.3% throughout the rest of the world. Tumor prognostic characteristics including hormone receptor status (positive: 72.3%, negative: 27.7%), clinical stage at presentation (inoperable: 25.3%, operable: 74.8%) and pathological nodal status after preoperative therapy (node positive: 46.4%, node negative or not evaluated: 53.6%) were similar in the study arms.
The majority of the patients (76.9%) had received an anthracycline-containing neoadjuvant chemotherapy regimen.19.5% percent of patients received another HER2-targeted agent in addition to trastuzumab as a component of neoadjuvant therapy; 93.8% of these patients received pertuzumab. All of the patients had received taxanes as part of neoadjuvant chemotherapy.
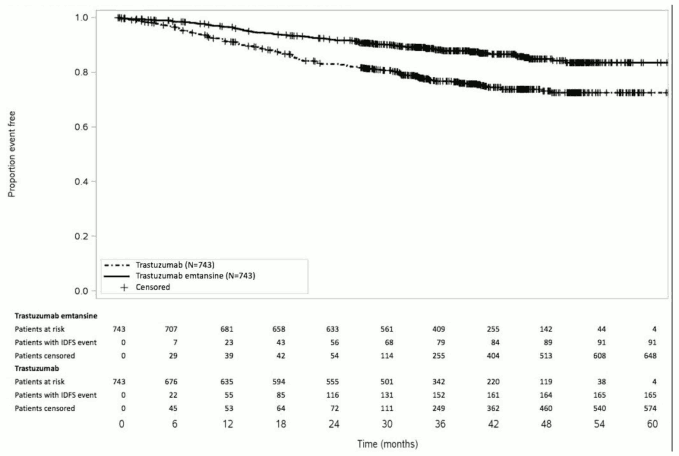
A clinically meaningful and statistically significant improvement in IDFS was observed in patients who received trastuzumab emtansine compared with trastuzumab (HR = 0.50, 95% CI [0.39, 0.64], p<0.0001. Estimates of 3 years IDFS rates were 88.3% vs. 77.0% in trastuzumab emtansine vs. trastuzumab arms, respectively. See Table 6 and Figure 1.
Table 6. Summary of efficacy from study BO27938 (KATHERINE):
| Trastuzumab N=743 | Trastuzumab Emtansine N=743 | |
|---|---|---|
| Primary Endpoint | ||
| Invasive Disease-Free Survival (IDFS) | ||
| Number (%) of patients with event | 165 (22.2%) | 91 (12.2%) |
| HR [95% CI] | 0.50 [0.39, 0.64] | |
| p-value (Log-Rank test, unstratified) | <0.0001 | |
| 3 year event-free rate2, % [95% CI] | 77.02 [73.78, 80.26] | 88.27 [85.81, 90.72] |
| Secondary Endpoints1 | ||
| Overall Survival (OS) | ||
| Number (%) of patients with event | 56 (7.5%) | 42 (5.7%) |
| HR [95% CI] | 0.70 [0.47, 1.05] | |
| p-value (Log-Rank test, unstratified) | 0.0848 | |
| 5 year survival rate2, % [95% CI] | 86.8 [80.95, 92.63] | 92.1 [89.44, 94.74] |
| IDFS including second primary non-breast cancer3 | ||
| Number (%) of patients with event | 167 (22.5%) | 95 (12.8%) |
| HR [95% CI] | 0.51 [0.40, 0.66] | |
| p-value (Log-Rank test, unstratified) | <0.0001 | |
| 3 year event-free rate2, % [95% CI]] | 76.9 [73.65, 80.14] | 87.7 [85.18, 90.18] |
| Disease-Free Survival (DFS)3 | ||
| Number (%) of patients with event | 167 (22.5%) | 98 (13.2%) |
| HR [95% ΔΕ] | 0.53 [0.41, 0.68] | |
| p-value (Log-Rank test, unstratified) | <0.0001 | |
| 3 year event-free rate2,% [95% CI]] | 76.9 [73.65, 80.14] | 87.41 [84.88, 89.93] |
| Distant recurrence-free interval (DRFI)3 | ||
| Number (%) of patients with event | 121 (16.3%) | 78 (10.5%) |
| HR [95% ΔΕ] | 0.60 [0.45, 0.79] | |
| p-value (Log-Rank test, unstratified) | 0.0003 | |
| 3 year event-free rate2, % [95% CI]] | 83.0 [80.10, 85.92] | 89.7 [87.37, 92.01] |
Data from first interim analysis 25 July 2018
Key to abbreviations (Table6): HR: Hazard Ratio; CI: Confidence Intervals,
1 Hierarchical testing applied for IDFS and OS
2 3-year event-free rate and 5-year survival rate derived from Kaplan-Meier estimates
3 These secondary endpoints were not adjusted for multiplicity
Figure 1. Kaplan-Meier Curve of Invasive Disease-Free Survival in KATHERINE:
In KATHERINE, consistent treatment benefit of trastuzumab emtansine for IDFS was seen in all the pre-specified subgroups evaluated, supporting the overall result.
A Phase III, randomised, multicentre, international, open-label clinical study was conducted in patients with HER2-positive unresectable locally advanced breast cancer (LABC) or MBC who had received prior taxane and trastuzumab-based therapy, including patients who received prior therapy with trastuzumab and a taxane in the adjuvant setting and who relapsed during or within six months of completing adjuvant therapy. Only patients with Eastern Cooperative Oncology Group (ECOG) Performance Status 0 or 1 were eligible. Prior to enrolment, breast tumour samples were required to be centrally confirmed for HER2-positive status defined as a score of 3 + by IHC or gene amplification by ISH. Baseline patient and tumour characteristics were well balanced between treatment groups. Patients with treated brain metastases were eligible for enrollment if they did not require therapy to control symptoms. For patients randomised to trastuzumab emtansine, the median age was 53 years, most patients were female (99.8%), the majority were Caucasian (72%), and 57% had oestrogen-receptor and/or progesterone-receptor positive disease. The study compared the safety and efficacy of trastuzumab emtansine with that of lapatinib plus capecitabine. A total of 991 patients were randomised to trastuzumab emtansine or lapatinib plus capecitabine as follows:
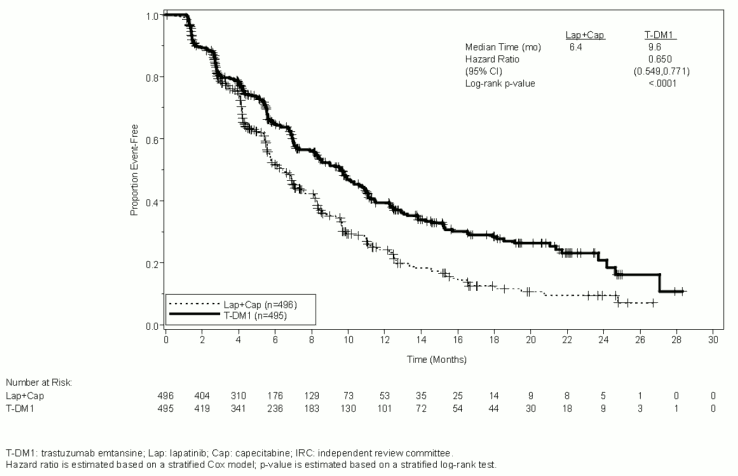
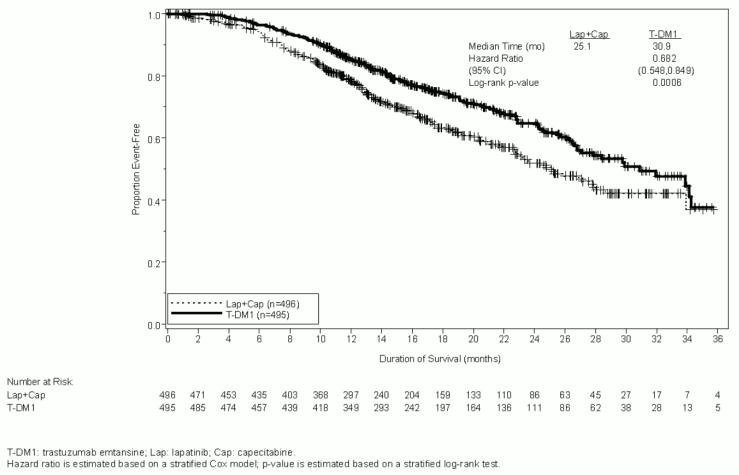
The co-primary efficacy endpoints of the study were progression-free survival (PFS) as assessed by an independent review committee (IRC) and overall survival (OS) (see Table 7 and Figures 2 to 3).
Time to symptom progression, as defined by a 5-point decrease in the score derived from the Trials Outcome Index-Breast (TOI-B) subscale of the Functional Assessment of Cancer Therapy-Breast Quality of Life (FACT-B QoL) questionnaire was also assessed during the clinical study. A change of 5 points in the TOI-B is considered clinically significant. Kadcyla delayed patient-reported time to symptom progression for 7.1 months compared with 4.6 months for the control arm (Hazard Ratio 0.796 (0.667, 0.951); p-value 0.0121). The data are from an open-label study and no firm conclusions can be drawn.
Table 7. Summary of efficacy from study TDM4370g/BO21977 (EMILIA):
| Lapatinib + Capecitabine n=496 | Trastuzumab emtansine n=495 | |
|---|---|---|
| Primary endpoints | ||
| IRC-assessed progression-free survival | ||
| Number (%) of patients with event | 304 (61.3%) | 265 (53.5%) |
| Median duration of PFS (months) | 6.4 | 9.6 |
| Hazard ratio (stratified*) | 0.650 | |
| 95% CI for Hazard ratio | (0.549, 0.771) | |
| p-value (Log-rank test, stratified*) | <0.0001 | |
| Overall Survival (OS)** | ||
| Number (%) of patients who died | 182 (36.7%) | 149 (30.1%) |
| Median duration of survival (months) | 25.1 | 30.9 |
| Hazard ratio (stratified*) | 0.682 | |
| 95% CI for Hazard ratio | (0.548, 0.849) | |
| p-value (Log-rank test*) | 0.0006 | |
| Key secondary endpoints | ||
| Investigator-assessed PFS | ||
| Number (%) of patients with event | 335 (67.5%) | 287 (58.0%) |
| Median duration of PFS (months) | 5.8 | 9.4 |
| Hazard ratio (95% CI) | 0.658 (0.560, 0.774) | |
| p-value (Log-rank test*) | <0.0001 | |
| Objective response rate (ORR) | ||
| Patients with measurable disease | 389 | 397 |
| Number of patients with OR (%) | 120 (30.8%) | 173 (43.6%) |
| Difference (95% CI) | 12.7% (6.0, 19.4) | |
| p-value (Mantel-Haenszel chi-squared test*) | 0.0002 | |
| Duration of objective response (months) | ||
| Number of patients with OR | 120 | 173 |
| Median 95% CI | 6.5 (5.5, 7.2) | 12.6 (8.4, 20.8) |
OS: overall survival; PFS: progression-free survival; ORR: objective response rate; OR: objective response; IRC: independent review committee; HR: hazard ratios; CI: confidence interval
* Stratified by: world region (United States, Western Europe, other), number of prior chemotherapeutic regimens for locally advanced or metastatic disease (0-1 vs. >1), and visceral vs. non-visceral disease.
** The interim analysis for OS was conducted when 331 events were observed. Since the efficacy boundary was crossed at this analysis, this is considered the definitive analysis.
A treatment benefit was seen in the subgroup of patients who had relapsed within 6 months of completing adjuvant treatment and had not received any prior systemic anti-cancer therapy in the metastatic setting (n=118); hazard ratios for PFS and OS were 0.51 (95% CI: 0.30, 0.85) and 0.61 (95% CI: 0.32, 1.16), respectively. The median PFS and OS for the trastuzumab emtansine group were 10.8 months and not reached, respectively, compared with 5.7 months and 27.9 months, respectively, for the lapatinib plus capecitabine group.
Figure 2. Kaplan-meier curve of IRC-assessed progression-free survival:
Figure 3. Kaplan-meier curve of overall survival:
In study TDM4370g/BO21977, consistent treatment benefit of trastuzumab emtansine was seen in the majority of pre-specified subgroups evaluated, supporting the robustness of the overall result. In the subgroup of patients with hormone receptor-negative disease (n=426), the hazard ratios for PFS and OS were 0.56 (95% CI: 0.44, 0.72) and 0.75 (95% CI: 0.54, 1.03), respectively. In the subgroup of patients with hormone receptor-positive disease (n=545), the hazard ratios for PFS and OS were 0.72 (95% CI: 0.58, 0.91) and 0.62 (95% CI: 0.46, 0.85), respectively.
In the subgroup of patients with non-measurable disease (n=205), based on IRC assessments, the hazard ratios for PFS and OS were 0.91 (95% CI: 0.59, 1.42) and 0.96 (95% CI: 0.54, 1.68), respectively. In patients ≥65 years old (n=138 across both treatment arms) the hazard ratios for progression-free survival (PFS) and Overall Survival (OS) were 1.06 (95% CI: 0.68, 1.66) and 1.05 (95% CI: 0.58, 1.91), respectively. In patients 65 to 74 years old (n=113), based on IRC assessments, the hazard ratios for PFS and OS were 0.88 (95% CI: 0.53, 1.45) and 0.74 (95% CI: 0.37, 1.47), respectively. For patients 75 years or above, based on IRC assessments, the hazard ratios for PFS and OS were 3.51 (95% CI: 1.22, 10.13) and 3.45 (95% CI: 0.94, 12.65), respectively. The subgroup of patients 75 years or above did not demonstrate a benefit for PFS or OS, but was too small (n=25) to draw any definitive conclusions.
In the descriptive follow-up overall survival analysis, the hazard ratio was 0.75 (95% CI 0.64, 0.88). The median duration of overall survival was 29.9 months in the trastuzumab emtansine arm compared with 25.9 months in the lapatinib plus capecitabine arm. At the time of the descriptive follow-up overall survival analysis, a total of 27.4% of the patients had crossed over from the lapatinib plus capecitabine arm to the trastuzumab emtansine arm. In a sensitivity analysis censoring patients at the time of cross-over, the hazard ratio was 0.69 (95% CI 0.59, 0.82). The results of this descriptive follow-up analysis are consistent with the confirmatory OS analysis.
A randomised, multicentre, open-label phase II study evaluated the effects of trastuzumab emtansine versus trastuzumab plus docetaxel in patients with HER2-positive MBC who had not received prior chemotherapy for metastatic disease. Patients were randomised to receive trastuzumab emtansine 3.6 mg/kg intravenously every 3 weeks (n=67) or trastuzumab 8 mg/kg intravenous loading dose followed by 6 mg/kg intravenously every 3 weeks plus docetaxel 75-100 mg/m² intravenously every 3 weeks (n=70).
The primary endpoint was investigator assessed Progression-Free Survival (PFS). The median PFS was 9.2 months in the trastuzumab plus docetaxel arm and 14.2 months in the trastuzumab emtansine arm (hazard ratio, 0.59; p=0.035), with a median follow-up of approximately 14 months in both arms. The objective response rate (ORR) was 58.0% with trastuzumab plus docetaxel and 64.2% with trastuzumab emtansine. The median duration of response was not reached with trastuzumab emtansine vs. 9.5 months in the control arm.
A Phase II, single-arm, open-label study evaluated the effects of trastuzumab emtansine in patients with HER2-positive incurable, LABC or MBC. All patients were previously treated with HER2-directed therapies (trastuzumab and lapatinib), and chemotherapy (anthracycline, taxane, and capecitabine) in the neoadjuvant, adjuvant, locally advanced, or metastatic setting. The median number of anti-cancer agents that patients had received in any setting was 8.5 (range, 5-19) and in the metastatic setting was 7.0 (range, 3-17), including all agents intended for the treatment of breast cancer.
Patients (n=110) received 3.6 mg/kg of trastuzumab emtansine intravenously every 3 weeks until disease progression or unacceptable toxicity.
The key efficacy analyses were ORR based on independent radiologic review and duration of objective response. The ORR was 32.7% (95% CI: 24.1, 42.1), n = 36 responders, by both IRC and investigator review. The median duration of response by IRC was not reached (95% CI, 4.6 months to not estimable).
The European Medicines Agency has waived the obligation to submit the results of studies with trastuzumab emtansine in all subsets of the paediatric population in breast cancer (see section 4.2 for information on paediatric use).
The population pharmacokinetic analysis suggested no difference in trastuzumab emtansine exposure based on disease status (adjuvant vs. metastatic setting).
Trastuzumab emtansine is administered intravenously. There have been no studies performed with other routes of administration.
Patients in Study TDM4370g/BO21977 and Study BO29738 who received 3.6 mg/kg of trastuzumab emtansine intravenously every 3 weeks had a mean Cycle 1 maximum serum concentration (Cmax) of trastuzumab emtansine of 83.4 (± 16.5) μg/mL and 72.6 (± 24.3) μg/mL, respectively. Based on population PK analysis, following intravenous administration, the central volume of distribution of trastuzumab emtansine was (3.13 L) and approximated that of plasma volume.
Trastuzumab emtansine is expected to undergo deconjugation and catabolism by means of proteolysis in cellular lysosomes.
In vitro metabolism studies in human liver microsomes suggest that DM1, a small molecule component of trastuzumab emtansine, is metabolised mainly by CYP3A4 and to a lesser extent by CYP3A5. DM1 did not inhibit major CYP450 enzymes in vitro. In human plasma, trastuzumab emtansine catabolites MCC-DM1, Lys-MCC-DM1, and DM1 were detected at low levels. In vitro, DM1 was a substrate of P-glycoprotein (P-gp).
Based on population pharmacokinetic (PK) analysis, following intravenous administration of trastuzumab emtansine in patients with HER2-positive metastatic breast cancer, the clearance of trastuzumab emtansine was 0.68 L/day and the elimination half-life (t½) was approximately 4 days. No accumulation of trastuzumab emtansine was observed after repeated dosing of intravenous infusion every 3 weeks.
Based on population PK analysis, body weight, albumin, sum of longest diameter of target lesions by Response Evaluation Criteria In Solid Tumors (RECIST), HER2 shed extracellular domain (ECD), baseline trastuzumab concentrations, and aspartate aminotransferase (AST) were identified as statistically significant covariates for trastuzumab emtansine PK parameters. However, the magnitude of effect of these covariates on trastuzumab emtansine exposure suggests that these covariates are unlikely to have any clinically meaningful effect on trastuzumab emtansine exposure. In addition, exploratory analysis showed that the impact of covariates (i.e., renal function, race and age) on the pharmacokinetics of total trastuzumab and DM1 was limited and was not clinically relevant. In nonclinical studies, trastuzumab emtansine catabolites including DM1, Lys-MCC-DM1, and MCC-DM1 are mainly excreted in the bile with minimal elimination in urine.
Trastuzumab emtansine when administered intravenously every 3 weeks exhibited linear PK across doses ranging from 2.4 to 4.8 mg/kg; patients who received doses less than or equal to 1.2 mg/kg had faster clearance.
The population PK analysis showed that age did not affect the PK of trastuzumab emtansine. No significant difference was observed in the PK of trastuzumab emtansine among patients <65 years (n=577), patients between 65-75 years (n=78) and patients >75 years (n=16).
No formal PK study has been conducted in patients with renal impairment. The population PK analysis showed that creatinine clearance does not affect the PK of trastuzumab emtansine. Pharmacokinetics of trastuzumab emtansine in patients with mild (creatinine clearance CLcr 60 to 89 mL/min, n=254) or moderate (CLcr 30 to 59 mL/min, n=53) renal impairment were similar to those in patients with normal renal function (CLcr ≥90 mL/min, n=361). Pharmacokinetic data in patients with severe renal impairment (CLcr 15 to 29 mL/min) are limited (n=1), therefore no dosage recommendations can be made.
The liver is a primary organ for eliminating DM1 and DM1-containing catabolites. The pharmacokinetics of trastuzumab emtansine and DM1-containing catabolites were evaluated after the administration of 3.6 mg/kg of trastuzumab emtansine to metastatic HER2+ breast cancer patients with normal hepatic function (n=10), mild (Child-Pugh A; n=10) and moderate (Child-Pugh B; n=8) hepatic impairment.
Plasma concentrations of DM1 and DM1-containing catabolites (Lys-MCC-DM1 and MCC-DM1) were low and comparable between patients with and without hepatic impairment.
Systemic exposures (AUC) of trastuzumab emtansine at Cycle 1 in patients with mild and moderate hepatic impairment were approximately 38% and 67% lower than that of patients with normal hepatic function, respectively. Trastuzumab emtansine exposure (AUC) at Cycle 3 after repeated dosing in patients with mild or moderate hepatic dysfunction was within the range observed in patients with normal hepatic function.
No formal pharmacokinetic study has been conducted and no population PK data was collected in patients with severe hepatic impairment (Child-Pugh class C).
The population PK analysis showed that race did not appear to influence the PK of trastuzumab emtansine. Because most of the patients in trastuzumab emtansine clinical studies were females, the effect of gender on the PK of trastuzumab emtansine was not formally evaluated.
Administration of trastuzumab emtansine was well tolerated in rats and monkeys at doses up to 20 and 10 mg/kg, respectively, corresponding to 2040 μg DM1/m² in both species, which is approximately equivalent to the clinical dose of trastuzumab emtansine in patients. In the GLP toxicity studies, with the exception of irreversible peripheral axonal toxicity (observed only in monkeys at ≥10 mg/kg) and reproductive organ toxicity (observed only in rats at 60 mg/kg), partially or completely reversible dose dependent toxicities were identified in both animal models. Principal toxicities included liver (liver enzyme elevations) at ≥20 mg/kg and ≥10 mg/kg, bone marrow (reduced platelet and white blood cell count)/hematologic at ≥20 mg/kg and ≥10 mg/kg, and lymphoid organs at ≥20 mg/kg and ≥3 mg/kg, in rat and monkey, respectively.
DM1 was aneugenic or clastogenic in an in vivo single-dose rat bone marrow micronucleus assay at exposures that were comparable to mean maximum concentrations of DM1 measured in humans administered trastuzumab emtansine. DM1 was not mutagenic in an in vitro bacterial reverse mutation (Ames) assay.
No fertility studies in animals have been performed to evaluate the effect of trastuzumab emtansine. However, based on results from general animal toxicity studies, adverse effects on fertility can be expected.
Dedicated embryo-foetal development studies have not been conducted in animals with trastuzumab emtansine. Developmental toxicity of trastuzumab has been identified in the clinical setting although it was not predicted in the non-clinical program. In addition, developmental toxicity of maytansine has been identified in non-clinical studies which suggests that DM1, the microtubule-inhibiting cytotoxic maytansinoid component of trastuzumab emtansine, will be similarly teratogenic and potentially embryotoxic.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.