KETOCONAZOLE HRA Tablet Ref.[8866] Active ingredients: Ketoconazole
Source: Medicines & Healthcare Products Regulatory Agency (GB) Revision Year: 2017 Publisher: Laboratoire HRA Pharma, 15 rue Béranger, 75003 Paris, France
Contraindications
- Hypersensitivity to ketoconazole and/or to any imidazole antifungal medication, or to any of the excipients listed in section 6.1.
- Acute or chronic liver disease and/or if pre-treatment liver enzymes levels are above 2 times the upper limit of normal (see sections 4.2 and 4.4).
- Pregnant women (see section 4.6).
- Breastfeeding women (see section 4.6).
- Congenital or documented acquired QTc prolongation.
- Concomitant therapy with any of the following medicinal products which may interact and result in potentially life-threatening adverse reactions (sections 4.4 and 4.5):
- CYP3A4 metabolised HMG-CoA reductase inhibitors (eg simvastatin, atorvastatin and lovastatin) due to an increased risk of skeletal muscle toxicity including rhabdomyolysis
- eplerenone due to an increased risk of hyperkalemia and hypotension
- substances that may have their plasma concentrations increased and have QT prolonging potential : methadone, disopyramide, quinidine, dronedarone, pimozide, sertindole, saquinavir (saquinavir/ritonavir 1000/100 mg bid), ranolazine, mizolastine, halofantrine
- dabigatran due to an increased bleeding risk
- triazolam, oral midazolam and alprazolam due to potential for prolonged or increased sedation and respiratory depression
- ergot alkaloids (eg dihydroergotamine, ergometrine (ergonovine), ergotamine and methylergometrine (methylergonovine) due to an increased risk of ergotism and other serious vasospastic adverse events
- lurasidone
- quetiapine due to an increased risk of toxicity
- telithromycin and clarithromycin in patients with severe renal impairment due to an increased risk of hepatotoxicity and QT interval prolongation
- felodipine, nisoldipine due to an increased risk of oedema and congestive heart failure
- colchicine in patients with renal impairment due to an increased risk of severe adverse reactions
- irinotecan due to an alteration of the metabolism of this medicinal product
- everolimus, sirolimus (also known as rapamycin) due to an increase of the plasma concentrations of these medicinal products
- vardenafil in men older than 75-years due to increased risk of adverse events
- paritaprevir/ombitasvir (ritonavir) due to increased risk of adverse reactions
- fesoterodine and solifenacin in patients with renal impairment
The list above is not an inclusive list of compounds that may interact with ketoconazole and result in potentially life-threatening reactions.
Special warnings and precautions for use
Monitoring of liver function
Liver enzymes should be monitored in all patients receiving Ketoconazole HRA. Due to the risk of serious hepatic toxicity, close follow-up of patients is required (see section 4.2).
Monitoring of adrenal function
Adrenal function should be monitored at regular intervals since adrenal insuficiency can occur during the treatment under conditions of a relative cortisol deficiency due to an increased glucocorticoid demand (e.g. in case of stress, surgery, or infection); and/or in case of Ketoconazole HRA overtreatment (for the patients treated with a block-only regimen); or if there is insufficient glucocorticoid replacement therapy (for the patients treated with a block-and-replace regimen). Serum or plasma and/or salivary cortisol and/or urinary free cortisol levels should be monitored, within one week following Ketoconazole HRA initiation as a minimum, and then periodically thereafter. When urinary free/serum/ plasma cortisol levels are normalised or close to target and the effective dose of Ketoconazole HRA is established, monitoring can be undertaken every 3 to 6 months (see section 4.2 for dose adjustment in case of adrenal insufficiency).
All patients should be monitored and informed about the signs and symptoms associated with hypocortisolism (e.g. weakness, fatigue, anorexia, nausea, vomiting, weight-loss, hypotension, hyponatraemia, hyperkalaemia and/or hypoglycaemia).
If clinical symptoms are suggestive of adrenal insufficiency, cortisol levels should be measured and Ketoconazole HRA should be temporarily discontinued or the dose reduced and if necessary corticosteroid substitution should be initiated. Ketoconazole HRA can be resumed thereafter at a lower dose (see section 4.2).
Block and replace regimen
Patients treated with a block-and-replace regimen should be taught to adjust their glucocorticoid replacement therapy dose under conditions of stress (see section 4.2). In addition, they should receive an emergency card and be equipped with an emergency glucocorticoid set.
Monitoring of the QTc interval
Monitoring for an effect on the QTc interval is advisable. An ECG should be performed:
- Prior to the start of Ketoconazole HRA
- Within one week after the beginning of the treatment
- As clinically indicated thereafter.
In case of co-administration of an agent known to increase QTc interval (see section 4.5), ECG monitoring is recommended.
Contraception
Women must be provided with comprehensive information on pregnancy prevention. As a minimum requirement, women of childbearing potential must use an effective method of contraception (see section 4.6).
Decreased gastric acidity
Absorption is impaired when gastric acidity is decreased. Acid-neutralising medicines (e.g. aluminium hydroxide) should not be administered for at least 2 hours after the intake of Ketoconazole HRA. In patients with achlorhydria, such as certain AIDS patients and patients on acid secretion suppressors (e.g. H2-antagonists, proton pump inhibitors), it is advised to administer Ketoconazole HRA with an acidic beverage eg cola beverage, orange juice.
If acid secretion suppressors are added to or removed from the concomitant medication then ketoconazole dose should be adjusted according to cortisol levels.
Potential interaction with medicinal products
Ketoconazole HRA has a high potential for clinically important medicinal products interactions.
Ketoconazole HRA is mainly metabolised through CYP3A4. Coadministration of potent enzyme inducers of CYP3A4 may decrease the bioavailibity of Ketoconazole HRA. A review of concomitant medicinal products should be conducted when initiating ketoconazole treatment since ketoconazole is a known strong CYP3A4 inhibitor. The SmPC for concomitantly used products must be consulted for the recommendations regarding co-administration with strong CYP3A4 inhibitors.
Ketoconazole HRA is a potent inhibitor of CYP3A4: inhibition of CYP3A4 by Ketoconazole HRA can increase patients' exposure to a number of medicinal products which are metabolised through this enzymatic system (see section 4.5).
Ketoconazole HRA is also a potent inhibitor of P-gp: inhibition of P-gp by Ketoconazole HRA can increase patients' exposure to medicinal products which are P-gp substrates (see section 4.5).
CYP3A4-metabolised and/or P-gp substrates known to prolong the QT interval may be contraindicated with Ketoconazole HRA, since the combination may lead to an increased risk of ventricular tachyarrhythmias, including occurrences of torsade de pointes, a potentially fatal arrhythmia (see section 4.3).
Use with hepatotoxic medicinal products
Co-administration of Ketoconazole HRA and other medications known to have potentially hepatotoxic effect (eg paracetamol) is not recommended since the combination may lead to increased risk of liver damage.
Use with Pasireotide
Co-administration of Ketoconazole HRA and pasireotide is not recommended since the combination can lead to QT prolongation in patients with known cardiac rhythm disorders (see section 4.5).
Coexisting inflammatory/autoimmune disorders
Exacerbation or development of inflammatory/autoimmune disorders has been described after Cushing's syndrome remission, including after treatment with ketoconazole. Patients with Cushing's syndrome and coexisting inflammatory/autoimmune disorders should be supervised after normalisation of cortisol levels on ketoconazole.
Alcohol
Patients should be advised against alcohol consumption while on treatment (see section 4.5).
Warning regarding excipients
This medicinal product contains lactose. Patients with rare hereditary problems of galactase intolerance, Lapp lactase deficiency or glucose-galactose malabsorption should not take this medicine.
Interaction with other medicinal products and other forms of interaction
See section 4.3 Contraindications for the list of the medicinal products that are contraindicated during treatment with Ketoconazole HRA.
Medicinal products affecting the absorption of Ketoconazole HRA
Medicinal drugs affecting gastric acidity impair the absorption of Ketoconazole HRA (see section 4.4).
Effects of other medicinal products on the metabolism of Ketoconazole HRA
Ketoconazole HRA is mainly metabolised by cytochrome CYP3A4.
Enzyme-inducing drugs such as rifampicin, rifabutin, carbamazepine, isoniazid, nevirapine, mitotane and phenytoin may significantly reduce the bioavailability of Ketoconazole HRA. Use of Ketoconazole HRA with potent enzyme inducers is not recommended.
Potent inhibitors of CYP3A4 (e.g. antivirals such as ritonavir, ritonavir-boosted darunavir and ritonavir-boosted fosamprenavir) may increase the bioavailability of Ketoconazole HRA, these drugs should be used with caution when co-administered with Ketoconazole HRA and patients should be monitored closely for signs and symptoms of adrenal insuficiency. Ketoconazole HRA dose should be adjusted accordingly.
Effects of Ketoconazole HRA on the metabolism of the other medicinal products
Ketoconazole HRA is a potent inhibitor of CYP3A4 and can inhibit the metabolism of drugs metabolised by this enzyme. This can result in an increase and/or prolongation of their effects, including adverse effects.
In vitro data indicate that ketoconazole is an inhibitor of CYP1A2 and does not significantly inhibit CYP 2A6 and 2E1. At clinically relevant concentrations inhibition of CYP2B6, 2C9/C8, 2C19 and 2D6 by ketoconazole cannot be excluded.
Ketoconazole HRA can inhibit the transport of drugs by P-gp, which may result in an increased plasma concentration of these drugs.
Ketoconazole inhibits BCRP (Breast Cancer Resistance Protein) in in vitro studies. Data of inhibition indicate that risk of interaction with BCRP substrates cannot be excluded at the systemic level with very high doses of ketoconazole. However ketoconazole may be an inhibitor of BCRP at the intestinal level at clinically relevant concentrations. Considering the rapid absorption of ketoconazole, intake of BCRP substrates should be postponed for 2 hours after ketoconazole intake.
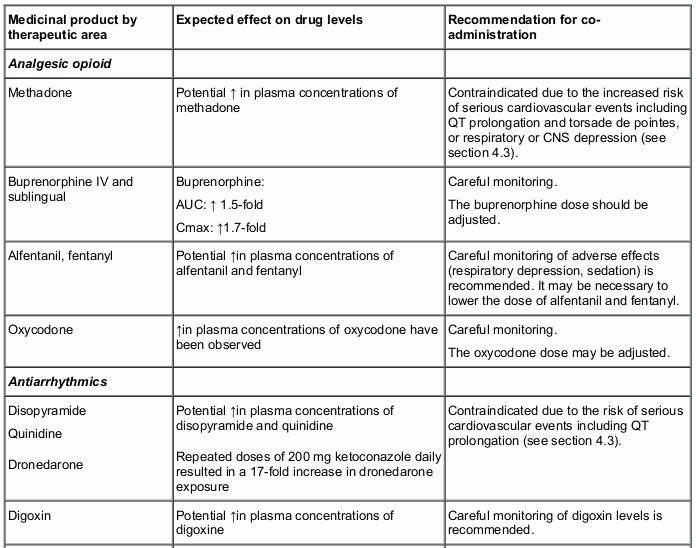
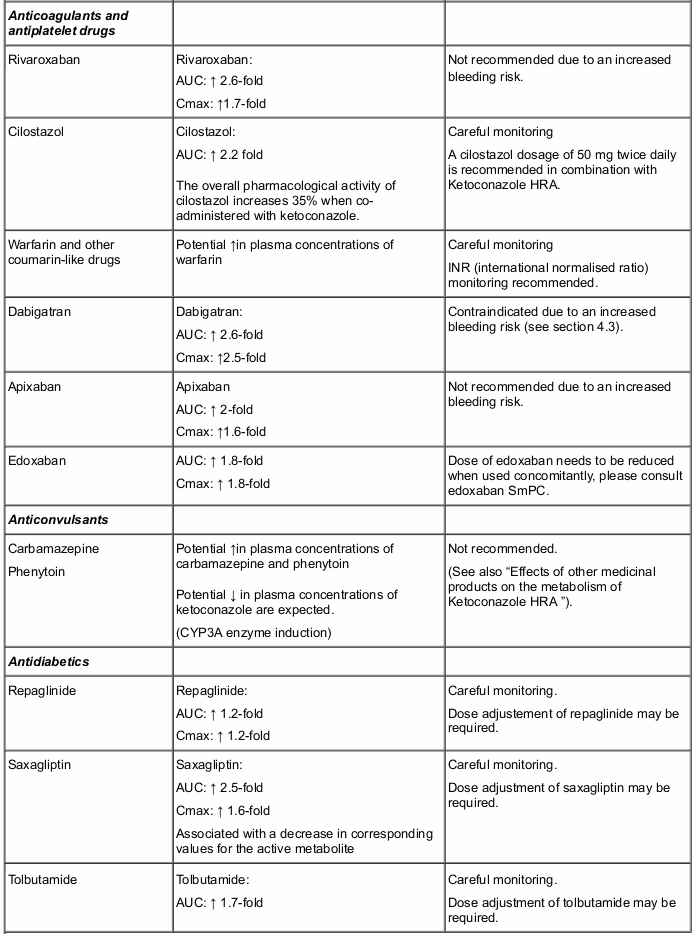
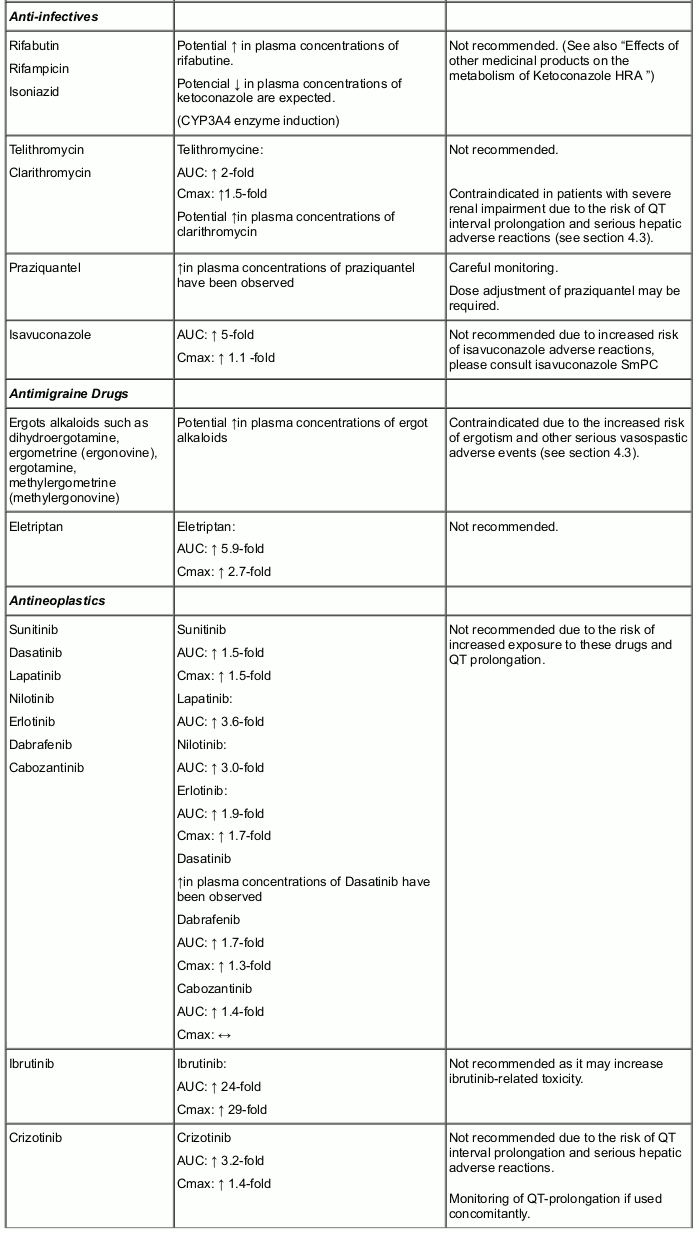
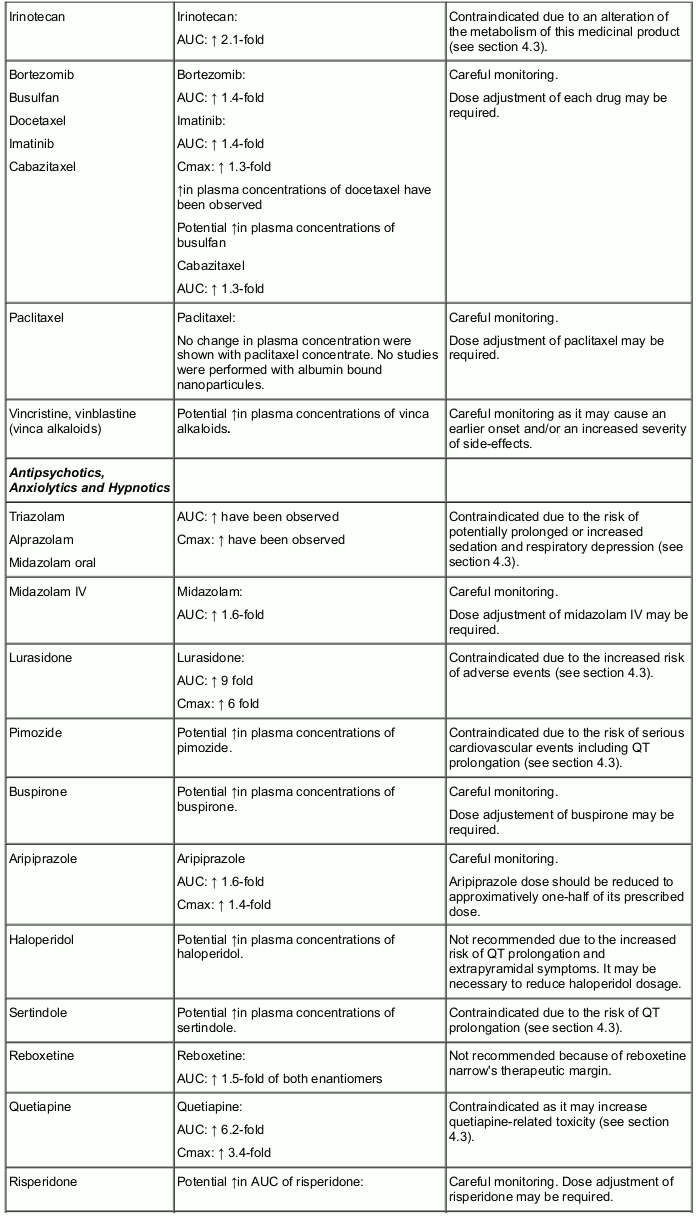
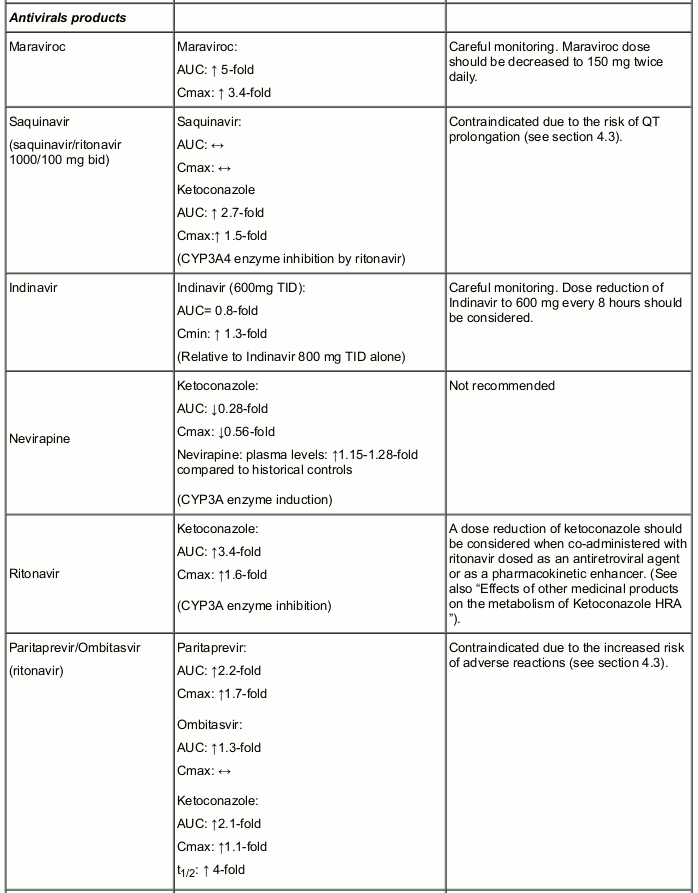
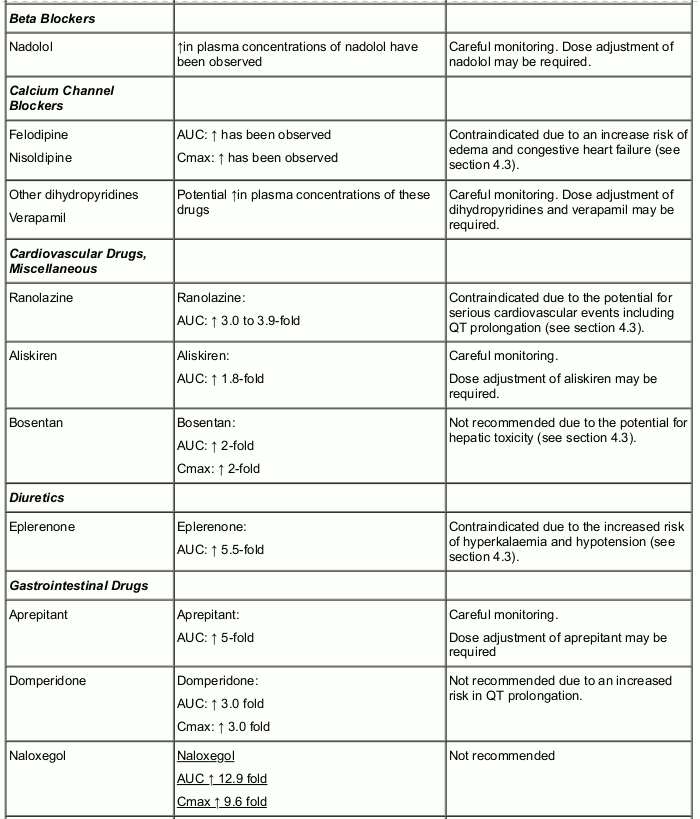
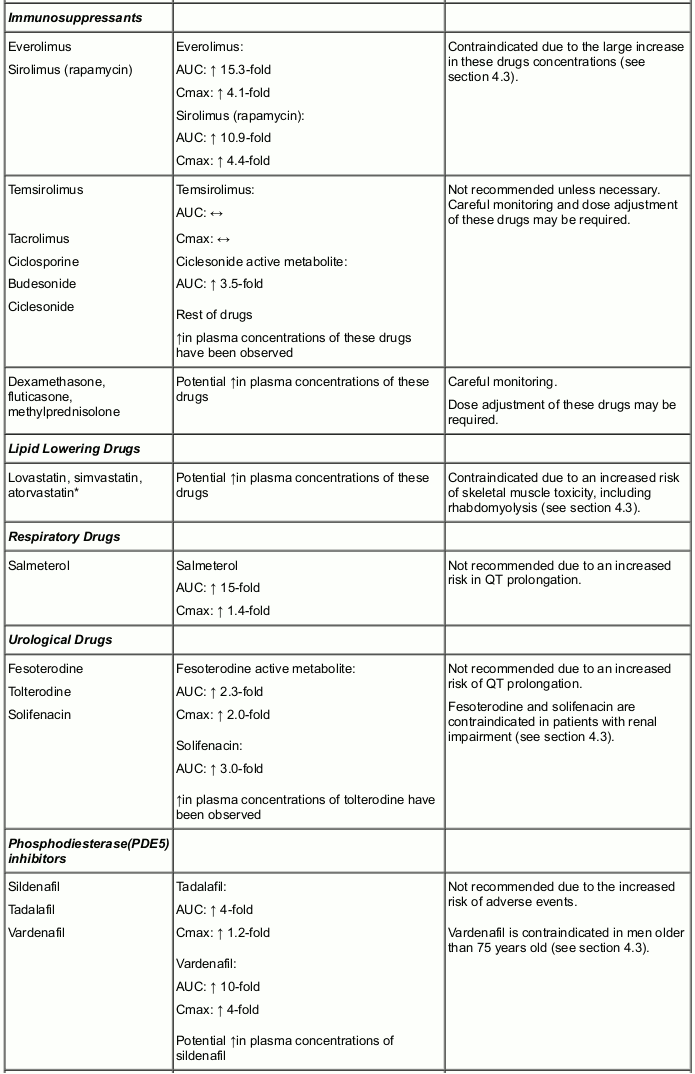
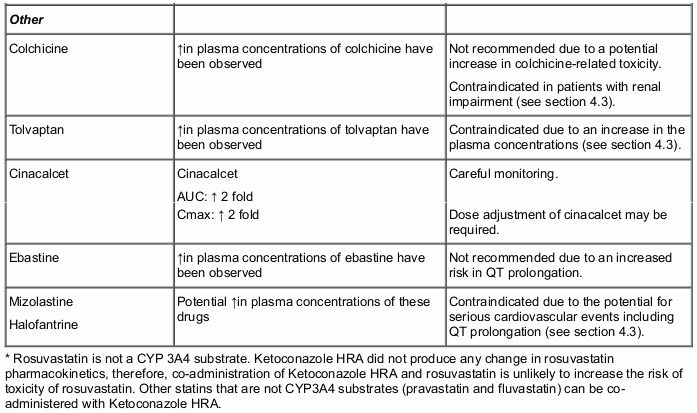
Table 1. Interactions and recommendations for co-administration:
Interactions between ketoconazole and other medicinal products are listed in the table below (increase is indicated as "↑", decrease as "↓", an no change as "↔"). The degrees of interaction mentioned below are not absolute values and may be dependent on the ketoconazole dose given i.e. many results are reported following a ketoconazole dose of 200 mg and a stronger interaction may be expected at a higher dose and/or shorter dosing interval. The following list is not an inclusive list of interactions between ketoconazole and other drugs.
Other interactions
Exceptional cases of a disulfiram-like reaction have been reported when ketoconazole was co-administered with alcohol, characterised by flushing, rash, peripheral oedema, nausea and headache, have been reported. All symptoms resolved completely within a few hours.
Co-administration of ketoconazole and pasireotide is not recommended since the combination can lead to a QT prolongation in patients with known cardiac rhythm disorders.
There is no evidence to suggest that there is an interaction between Ketoconazole HRA and other steroidogenesis inhibitors (ie metyrapone).
Fertility, pregnancy and lactation
Pregnancy
There are insufficient clinical data regarding the use of Ketoconazole HRA in pregnant women. Preclinical data show that Ketoconazole HRA crosses the placenta and is teratogenic. Ketoconazole HRA is contraindicated during pregnancy and it should not be used in women of childbearing potential not using an effective method of contraception (see section 4.3).
Breast-feeding
Since ketoconazole is excreted in the milk, mothers who are under treatment must not breast-feed whilst being treated with Ketoconazole HRA (see section 4.3).
Fertility
Studies in animals have shown effects on male and female reproductive parameters (see section 5.3).
Effects on ability to drive and use machines
No specific studies have been conducted to assess the effect of ketoconazole on the ability to drive or use machines. Patients should be warned about the potential for dizziness and somnolence (see section 4.8) and should be advised not to drive or operate machines if any of these symptoms occur.
Undesirable effects
Summary of the safety profile
The most frequent adverse reactions are adrenal insufficiency, nausea, vomiting, abdominal pain, diarrhoea, pruritus, rash and the hepatic enzymes increased.
The most serious adverse reaction is hepatotoxicity, primarily as acute hepatocellular toxicity but may also result in cholestatic injury or a mixed pattern of toxicity. ASAT, ALAT, gammaGT, bilirubin and alkaline phosphatase should be monitored at frequent intervals during treatment (see sections 4.2 and 4.4).
Tabulated list of adverse reactions
The safety of Ketoconazole HRA has been evaluated based on published literature and use of ketoconazole as an antifungal treatment.
The adverse reactions listed below in table 2 are classified according to System Organ Class. Frequency groupings are defined according to the following convention: very common (≥1/10), common (≥1/100 to <1/10), uncommon: (≥1/1,000 to <1/100), rare: (≥1/10,000 to <1/1,000), very rare (<1/10,000), not known: cannot be estimated from the available data.
Within each frequency grouping, undesirable effects are presented in order of decreasing seriousness.
Table 2. Incidence of adverse reactions and marked laboratory abnormalities reported in the literature in adults and adolescents patients:
Blood and lymphatic system disorders
Uncommon: Thrombocytopenia
Immune system disorders
Uncommon: Allergic conditions including anaphylactic shock, anaphylactoid reaction and anaphylactic reaction and angioedema
Endocrine disorders
Common: Adrenal insufficiency
Psychiatric disorders
Not Known: Insomnia, nervousness
Metabolism and nutrition disorders
Not known: Alcohol intolerance, anorexia, increased appetite
Nervous system disorders
Uncommon: Headache, dizziness, somnolence
Not known: Intracranial pressure increased (papilloedema, fontanelle bulging), paraesthesia
Eye disorders
Not known: Photophobia
Respiratory, thoracic and mediastinal disorders
Not known: Epistaxis
Gastrointestinal disorders
Common: Nausea, abdominal pain, vomiting, diarrhoea
Not known: Dyspepsia, flatulence, tongue discoloration, dry mouth, dysgeusia
Hepatobiliary disorders
Very common: Liver function tests abnormal
Rare: Serious hepatotoxicity, including jaundice, hepatitis, hepatic necrosis, hepatic cirrhosis, hepatic failure including cases necessitating transplantation or resulting in death. (see 4.4 Special warnings and special precautions for use)
Skin and subcutaneous tissue disorders
Common: Pruritus, rash
Uncommon: Urticaria, alopecia
Not known: Photosensitivity, erythema multiforme, dermatitis, erythema, xeroderma
Musculoskeletal and connective tissue disorder
Not known: Myalgia, arthralgia
Reproductive system and breast disorders
Not known: Menstrual disorder, azoospermia, erectile dysfunction, gynaecomastia
General disorders and administration site conditions
Uncommon: Asthenia
Very rare: Pyrexia
Not known: Oedema peripheral, malaise, hot flush
Investigations
Very common: Hepatic enzyme increased
Uncommon: Platelet count decreased
Not known: Transient decrease of testosterone concentrations
Description of selected adverse reactions
Hepatotoxicity
Serious hepatic toxicity caused by ketoconazole treatment is rare (1/15000). Acute hepatocellular injury has been primarily observed as has cholestatic injury or a mixed pattern of toxicity. Fatal cases have been reported particularly when treatment is continued despite liver enzyme elevation. Increases in liver enzymes (≤5N and >5N) were observed in ~13.5% and ~2.5% of patients respectively occurring mostly within the first 6 months of treatment. Liver enzyme levels returned to normal within 2-12 weeks after a dose decrease or withdrawal of ketoconazole. Hepatotoxicity does not appear to be dose dependent. All potential associated factors of hepatotoxicity, and abnormal liver enzyme levels detected before Ketoconazole HRA initiation, should be taken into account before considering Ketoconazole HRA treatment. Ketoconazole HRA should not be administered when liver enzymes are greater than 2 times the upper limit of normal or in association with other hepatotoxic drugs. Liver enzyme monitoring should be performed once weekly during the first month of treatment and then monthly for 6 months. In the case an increase of liver enzymes is detected which is less than 3 times the upper limit of normal, closer monitoring of liver function should be performed and the daily dose should be decreased by at least 200 mg. In the case of increase of liver enzymes levels above 3 times the upper limit of normal, Ketoconazole HRA should be stopped immediately and should not be reintroduced because of the risk of serious hepatic toxicity.
Adrenal Insufficiency
Adrenal insufficiency may occur in patients on ketoconazole without corticosteroid substitution (block-only regimen) or if there is an insufficient glucocorticoid replacement therapy (for the patients treated with a block-and-replace regimen). Monitor and instruct patients on the signs and symptoms associated with hypocortisolism (e.g. weakness, fatigue, anorexia, nausea, vomiting, hypotension, hyperkalemia, hyponatraemia, hyperkalaemia or hypoglycaemia). Adrenal insufficiency may be detected by periodic clinical assessment and monitoring of plasma/serum or salivary cortisol levels. In case of adrenal insufficiency, Ketoconazole HRA treatment should be temporarily discontinued or the dose reduced and, if needed, a corticosteroid substitution therapy added.
Paediatric population
Frequency of hepatotoxicity could be higher in adolescents than in adults. In the literature, among 24 paediatric patients treated with ketoconazole, two developed severe hepatoxicity. A 14 year-old girl who was treated for Cushing's disease with ketoconazole 200 mg twice daily presented one month later with jaundice, fever anorexia, nausea and vomiting. Ketoconazole was stopped but she deteriorated rapidly and died. A 17 years old girl was treated on ketoconazole 1200 mg/day for an adrenal carcinoma with liver metastasis and had altered liver function tests at 22 days. After ketoconazole withdrawal, liver enzymes returned to normal levels within 3 weeks (section 5.1).
Reporting of suspected adverse reactions
Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via the national reporting system listed in Appendix V.
Incompatibilities
Not applicable.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.