KIMMTRAK Concentrate for solution for infusion Ref.[49841] Active ingredients: Tebentafusp
Source: European Medicines Agency (EU) Revision Year: 2022 Publisher: Immunocore Ireland Limited, Unit 1, Sky Business Centre, Dublin 17, D17 FY82, Ireland
5.1. Pharmacodynamic properties
Pharmacotherapeutic group: Antineoplastic agents, other antineoplastic agents
ATC code: not yet assigned
Mechanism of action
Tebentafusp is a bispecific fusion protein, comprised of a T cell receptor (TCR; targeting domain) fused to an antibody fragment targeting CD3 (cluster of differentiation 3; effector domain). The TCR end binds with high affinity to a gp100 peptide presented by human leukocyte antigen – A*02:01 (HLA-A*02:01) on the cell surface of uveal melanoma tumour cells, and the effector domain binds to the CD3 receptor on the polyclonal T cell.
An immune synapse is formed when the TCR targeting domain of tebentafusp binds to uveal melanoma cells and the CD3 effector domain binds to polyclonal T cells. This immune synapse results in redirection and activation of polyclonal T cells regardless of their native TCR specificity. Tebentafusp activated polyclonal T cells release inflammatory cytokines and cytolytic proteins, which result in direct lysis of uveal melanoma tumour cells.
Pharmacodynamic effects
Transient and clinically nonsignificant reduction in lymphocyte counts in blood was observed after treatment with tebentafusp. Lymphocytes decreased the day after the first 3 doses and returned to baseline prior to subsequent doses. After treatment with tebentafusp, transient increases in serum levels of proinflammatory cytokines and chemokines were observed in samples collected after the first three doses. Peak levels were observed between 8 to 24 hours after treatment with tebentafusp and levels returned to baseline prior to subsequent doses.
Clinical efficacy and safety
Study IMCgp100-202: Previously untreated metastatic uveal melanoma
Study IMCgp100-202 was a randomised, open label, multicentre study that enrolled HLA-A*02:01 positive metastatic uveal melanoma patients who were naïve to systemic therapy. Patient could not have received previous systemic treatment or localized (liver--directed) therapy for metastatic uveal melanoma except for a prior surgical resection of oligometastatic disease. Patient were excluded for presence of symptomatic or untreated brain metastasis, symptomatic congestive heart failure, QT interval corrected by Fridericia's formula (QTcF) >470 msec or congenital long QT syndrome, acute myocardial infarction, or unstable angina pectoris less than 6 months prior to treatment initiation.
Patients were randomised (2:1) to receive tebentafusp weekly by intravenous infusion according to the recommended intra-patient dosing regimen section 4.2 or investigator's choice treatment (pembrolizumab, ipilimumab, or dacarbazine) at the approved doses of these agents until disease progression or unacceptable toxicity.
Patients could receive tebentafusp, pembrolizumab, or ipilimumab treatment beyond disease progression if the patients were clinically stable, deriving clinical benefit and showed no signs of unacceptable toxicity as determined by the investigator. Treatment breaks for up to 2 consecutive weeks were allowed. Randomisation was stratified by lactate dehydrogenase (LDH) status, a known prognostic factor for unresectable or metastatic UM.
The primary efficacy outcome was overall survival (OS) in all patients randomised in the study. Tumour assessments were conducted every 12 weeks. Additional efficacy outcomes were investigator assessed progression free survival (PFS) A total of 378 patients were randomised; 252 to tebentafusp-treated group and 126 to the investigator's choice treated group (pembrolizumab: 82%; ipilimumab: 12%; or dacarbazine: 6 %). The median age was 64 years (range 23 to 92 years); with 49.5% of patients ≥65 years, 87% were white, 50% were female. Baseline ECOG performance status was 0 (72%) or 1 (20.4%) or 2 (0.3%), 36% had elevated LDH level, and 95% had liver metastasis.
In this study IMCgp100-202, 43% of patients received treatment beyond progression with tebentafusp with no new safety signals identified. Median duration of tebentafusp treatment beyond progression was 8 weeks. Of the total tebentafusp infusions during the study, 21.5% was administered after progression.
After completion of the primary efficacy analysis, patients from the investigator's choice arm were permitted to crossover to the tebentafusp treatment. With a median duration of follow up of 22.4 months, the updated OS continued to favour the tebentafusp arm (HR= 0.58; 95% CI: 0.44, 0.77). At the time of analysis, 16 patients had crossed over to tebentafusp treatment.
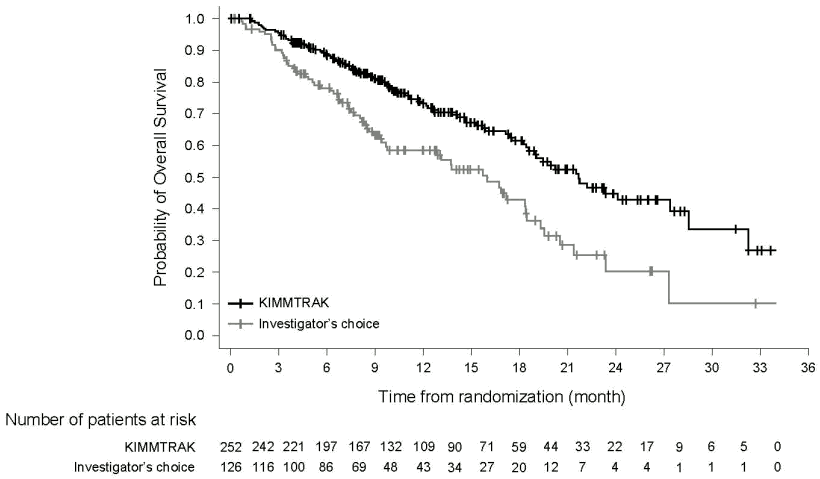
The efficacy results are summarized in Table 4 and Figure 1.
Table 4. Efficacy results in study IMCgp100-202:
| Primary and secondary endpoints | KIMMTRAK (N=252) | Investigator's choice therapy (N=126) |
|---|---|---|
| Overall survival (OS)1 | ||
| Number of deaths | 87 (34.5%) | 63 (50%) |
| Median months (95% CI) | 21.7 (18.6, 28.6) | 16.0 (9.7, 18.4) |
| HR (95% CI)2,4 | 0.51 (0.37, 0.71) | |
| Stratified log-rank p-value2 | p = <0.0001 | |
| Progression free survival (PFS)3,4 | ||
| Number (%) of patients with event | 198 (78.6%) | 97 (77%) |
| Median in months (95% CI) | 3.3 (3.0, 5.0) | 2.9 (2.8, 3.0) |
| HR (95% CI)4 | 0.73 (0.58, 0.94) | |
| Stratified log-rank p-value2 | p = 0.0139 | |
| Objective response rate (ORR)6 | ||
| n (%) | 26 (10.3) | 6 (4.8) |
| 95% CI | 6.9, 14.8 | 1.8, 10.1 |
| Complete Response (CR) | 1 (0.4) | 0 |
| Partial Response (PR) | 25 (9.9) | 6 (4.8) |
| Stable Disease (SD)5 | 52 (20.6) | 16 (12.7) |
| Median duration of response | ||
| Months (95% CI) | 9.9 (5.6, 22.1) | 9.7 (2.7, --) |
CI = Confidence interval, HR = Hazard ratio
1 At a prespecified interim analysis, 150 OS events were observed, and a p-value boundary for declaring efficacy (0.006) was determined by a Lan-Demets alpha spending function with O'Brien Fleming type boundary.
2 Two-sided p-value based on log rank test stratified by LDH.
3 As assessed by investigator using RECIST v1.1 criteria.
4 Hazard ratio is from a proportional hazards model stratified by LDH status
5 Based on ≥24 weeks.
6 Updated based on all patients having opportunity for at least 3 radiological assessments.
Figure 1. Kaplan-Meier curves of overall survival in the study IMCgp100-202:
Study IMCgp100-102: Previously treated metastatic uveal melanoma
Study IMCgp100-102 was an open-label, Phase 2 multicentre study conducted in 127 patients, who were treated with the dosing scheme recommended in section 4.2. Patients were required to be HLA-A*02:01 positive. Patients were eligible if they had experienced disease progression following at least 1 or more prior lines of liver directed therapy or systemic therapy including immune check point inhibitors in the metastatic setting. Patients were excluded for clinically significant cardiac disease and presence of symptomatic or untreated brain metastasis.
Major efficacy outcome measures included confirmed ORR as assessed by Independent Central Review (ICR) using Response Evaluation Criteria in Solid Tumours (RECIST) v1.1. Secondary efficacy outcomes included PFS, DCR, DOR and OS.
The median age was 61 years, 50% were female, 99% were white, the ECOG performance score was 0 (70%) or 1 (30%) and 96% of patients had liver metastasis. Prior treatments included immunotherapy (73% of patients) including immune checkpoint inhibitors (PD-1/PD-L1; 65%; CTLA-4; 31%) and liver directed therapy 45%. Efficacy results from study IMCgp100-102 are summarised in Table 5.
Table 5. Efficacy results in study IMCgp100-102:
| Primary and secondary endpoints | KIMMTRAK (N=127) |
|---|---|
| Confirmed objective response rate1 | 6 (4.7%) |
| (95% CI) | (1.8%, 10%) |
| Complete response (CR) | 0 |
| Partial Response (PR) | 6 (4.7%) |
| Stable Disease (SD)2 | 23 (18.1%) |
| Median duration of response | |
| Months (95% CI) | 8.7 (5.6, 24.5) |
1 As assessed by independent central review using RECIST v1.1 criteria.
2 Based on ≥24 weeks.
Paediatric population
The European Medicines Agency has waived the obligation to submit the results of studies with KIMMTRAK in all subsets of the paediatric population in the treatment of ocular melanoma (see section 4.2 for information on paediatric use).
5.2. Pharmacokinetic properties
Absorption
The pharmacokinetics of tebentafusp appear linear and dose proportional over a dose range of 20 mcg to 68 mcg. Following weekly intravenous infusion in metastatic uveal melanoma patients, the maximum plasma concentrations (Cmax) reached 4.2 ng/mL - 13.7 ng/mL immediately at the end of infusion (T=0.5 hours). No accumulation was observed with a weekly dosing regimen at the target therapeutic doses.
Distribution
Tebentafusp did not distribute extensively and displayed a volume of distribution comparable to blood volume (5.25 L).
Biotransformation
The metabolic pathway of tebentafusp has not been characterised. Like other protein therapeutics, tebentafusp is expected to be degraded into small peptides and amino acids via catabolic pathways.
Elimination
The excretion of tebentafusp is not fully characterised. Based on its molecular size that is close to the glomerular filtration size exclusion threshold, small amounts of tebentafusp may be excreted in the urine.
Following administration of tebentafusp in metastatic uveal melanoma patients the estimated systemic clearance was 4.29 L/d, with a terminal half-life of 6 to 8 hours.
Special populations
Population pharmacokinetic analysis indicated that there was no significant effect of weight (43 to 163 kg), gender, race, and age (23 to 91 years) on tebentafusp clearance.
Renal impairment
No formal pharmacokinetic studies of tebentafusp have been conducted in patients with renal impairment.
No impact on safety or efficacy parameters was identified in patients with mild (creatinine clearance [CrCL] ranging 60 to 89 mL/min) to moderate (CrCL ranging 30 to 59 mL/min) renal impairment and no dose adjustments are recommended. There are limited data from patients (<5%) with moderate renal impairment and there is no information available from patients with severe renal impairment (CrCL <30 mL/min).
Hepatic impairment
No formal pharmacokinetic studies of tebentafusp have been conducted in patients with hepatic impairment. Population PK analyses demonstrated that baseline and on treatment ALT/AST elevations did not impact tebentafusp pharmacokinetics. No dose adjustments based on ALT/AST levels are recommended.
5.3. Preclinical safety data
Tebentafusp is a human--specific protein and there are no relevant animal species in which nonclinical toxicology of tebentafusp could be tested.
No carcinogenicity, genotoxicity, or developmental and reproductive toxicity studies have been conducted with tebentafusp.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.