LEQSELVI Film-coated tablet Ref.[116129] Active ingredients: Deuruxolitinib
Source: FDA, National Drug Code (US) Revision Year: 2025
12.1. Mechanism of Action
Deuruxolitinib is a Janus kinase (JAK) inhibitor. JAKs mediate the signaling of a number of cytokines and growth factors that are important for hematopoiesis and immune function. JAK signaling involves recruitment of STATs (signal transducers and activators of transcription) to cytokine receptors, activation and subsequent localization of STATs to the nucleus leading to modulation of gene expression.
In an in vitro kinase activity assay, deuruxolitinib had greater inhibitory potency for JAK1, JAK2 and TYK2 relative to JAK3. The relevance of inhibition of JAK enzymes to therapeutic effectiveness is not currently known.
12.2. Pharmacodynamics
Deuruxolitinib Inhibition of IL-6 Induced STAT3 Phosphorylation
Deuruxolitinib inhibited whole blood IL-6 stimulated pSTAT3 in healthy subjects 2 hours post-dose. The relevance of this finding in patients is unknown.
Cardiac Electrophysiology
At concentrations approximately 4-fold higher than the Cmax associated with the highest dose evaluated clinically, 12 mg twice-daily, deuruxolitinib does not prolong the QT interval to any clinically relevant extent.
12.3. Pharmacokinetics
Following oral administration of deuruxolitinib, Cmax and AUCs increased dose proportionally over a dose range from 8 mg to 48 mg (6 times the approved recommended dosage) in healthy subjects. Steady-state plasma concentrations were achieved within 1 to 2 days, with minimal accumulation, after twice daily administration.
Absorption
Deuruxolitinib bioavailability is 90%, with peak plasma concentrations reached within 1.5 hrs.
Effect of Food
No clinically significant differences in the pharmacokinetics of deuruxolitinib were observed following administration of a high fat, high calorie meal (approximately 50% fat and 800-1000 calories).
Distribution
The deuruxolitinib steady state volume of distribution is approximately 50L. Deuruxolitinib plasma protein binding is 91.5% and blood to plasma concentration ratio is approximately 1.3.
Elimination
The deuruxolitinib mean elimination half-life is approximately 4 hrs.
Metabolism
Deuruxolitinib is primarily metabolized by CYP2C9 (76%) and CYP3A4 (21%) and to a lesser extent by CYP1A2 (3%). The two most abundant human metabolites C-21714 and C-21717, each of which accounted for approximately 5% of total drug-related AUC and both are approximately 10-fold less pharmacologically active than deuruxolitinib.
Excretion
After a single dose of radiolabeled deuruxolitinib, there was no unchanged dose recovered in either urine or feces.
Specific Populations
No clinically significant differences in the pharmacokinetics of deuruxolitinib were observed based on race [White (75%), African American (17%) and Asian (6%)], ethnicity [Hispanic or Latino (12%)], age (18-65 years), body weight (40.4-173 kg), mild to moderate renal impairment (eGFR 30-89 mL/min, MDRD), or mild to moderate hepatic impairment (Child Pugh A or B). The effect of severe renal impairment (eGFR <30 mL/min, MDRD) or severe hepatic impairment (Child Pugh C) on deuruxolitinib pharmacokinetics is unknown.
Drug Interaction Studies
Clinical Studies and Model-Informed Approaches
Effect of Other Drugs on LEQSELVI
Strong CYP3A4 and Moderate or strong CYP2C9 Inducers: Deuruxolitinib AUC decreased by 78% and Cmax by 41% following concomitant use of multiple doses of 600 mg rifampin (strong CYP3A4 and moderate CYP2C9 inducer) with a single dose of 12 mg deuruxolitinib (1.5 times the approved 8 mg dose).
Strong CYP2C9 Inhibitors: Based on modeling, deuruxolitinib AUC is predicted to be increased by 200% and Cmax by 25% following concomitant use of multiple dosages of a strong CYP2C9 inhibitor with a single dose of 12 mg deuruxolitinib (1.5 times the approved 8 mg dose).
Moderate CYP2C9 Inhibitors: Deuruxolitinib AUC increased by 140% and Cmax by 21% following concomitant use of multiple dosages of 200 mg fluconazole (dual moderate CYP3A4 and CYP2C9 inhibitor) with a single dose of 12 mg deuruxolitinib (1.5 times the approved 8 mg dose).
Other Drugs: No clinically significant differences in deuruxolitinib pharmacokinetics were observed when used concomitantly with itraconazole (strong CYP3A4 inhibitor) or are expected with efavirenz (moderate CYP3A4 inducer).
Effect of LEQSELVI on Other Drugs
No clinically significant differences in the pharmacokinetics of the following drugs were observed when co-administered with deuruxolitinib: midazolam (a sensitive CYP3A4 substrate), oral contraceptives (ethinyl estradiol and levonorgestrel).
In Vitro Studies
Cytochrome P450 (CYP) Enzymes: Deuruxolitinib is not an inhibitor of CYP1A2, CYP2B6, CYP2C8, CYP2C19, CYP2D6, or CYP3A4. Deuruxolitinib is not an inducer of CYP1A2 or CYP2B6, CYP2C8 or CYP2C19.
Transporter Systems: Deuruxolitinib is a substrate of BCRP and MDR1 but not a substrate of the uptake transporters OATP1B1 and OATP1B3. Deuruxolitinib is not an inhibitor of OATP1B1, OATP1B3 and OCT1 but is an inhibitor of BCRP, BSEP, OAT3 and MATE2-K.
12.5. Pharmacogenomics
Deuruxolitinib is primarily metabolized by CYP2C9 (76%) and CYP3A4 (21%). CYP2C9 activity is reduced in patients with genetic variants in CYP2C9, such as the CYP2C9 ∗2 and CYP2C9 ∗3 alleles. The impact of CYP2C9 genetic variants on the pharmacokinetics of deuruxolitinib has not been directly evaluated. Based on drug-drug interaction modeling data, CYP2C9 poor metabolizers (e.g., ∗2/ ∗3, ∗3/ ∗3) may have up to 2-fold higher concentrations of deuruxolitinib, when compared to normal metabolizers [see Warnings and Precautions (5.6)].
The pharmacokinetics of deuruxolitinib were not evaluated in individuals who are intermediate metabolizers (e.g., individuals with ∗1/ ∗3 genotype).
The prevalence of the CYP2C9 poor metabolizer phenotype is approximately 2 to 3% in White populations, 0.5 to 4% in Asian populations, and <1% in Black or African American populations. Other decreased or nonfunctional CYP2C9 alleles (e.g., ∗5, ∗6, ∗8, ∗11) are more prevalent in Black or African American populations.
13.1. Carcinogenesis, Mutagenesis, Impairment of Fertility
Deuruxolitinib was not carcinogenic when administered orally in a 6-month transgenic rasH2 mouse study at doses up to 100 mg/kg/day. In a 2-year rat carcinogenicity study, no drug-related tumors were observed at oral doses of deuruxolitinib up to 30 mg/kg/day (0.6 times the MRHD based on AUC comparison).
Deuruxolitinib was positive in an in vitro micronucleus assay, but negative in a bacterial mutation assay (the Ames test), an in vitro chromosome aberration assay and an in vivo rat micronucleus assay.
In fertility and early embryonic development studies in rats, deuruxolitinib was administered to male rats prior to mating to conception, or to female rats prior to mating, through conception, to gestation day 7. Deuruxolitinib had no adverse effects on male or female fertility at oral doses up to 100 mg/kg/day (2.2 times MRHD in males and 14 times MRHD in females based on AUC comparison). However, adverse effects on early embryonic development were noted, including decreased viable embryos and increased pre-implantation loss observed at doses ≥30 mg/kg/day (0.9 times MRHD based on AUC comparison), and increased post-implantation loss and resorption at 100 mg/kg/day (14 times MRHD based on AUC comparison). No adverse effects on early embryonic development were observed at 10 mg/kg/day (0.2 times MRHD based on AUC comparison).
14. Clinical Studies
Two multicenter, randomized, double-blind, placebo-controlled phase 3 clinical trials (AA-1 [NCT04518995] and AA-2 [NCT04797650]), evaluated a total of 1,209 adult subjects with alopecia areata (AA), who had at least 50% scalp hair loss as measured by the Severity of Alopecia Tool (SALT) for more than six months. In both trials, subjects received LEQSELVI 8 mg twice daily, deuruxolitinib 12 mg twice daily, or placebo twice daily for 24 weeks.
Deuruxolitinib 12 mg is not approved.
The trial population ranged from 18 to 65 years of age. Among the subjects enrolled, 64% were female, 74% were White, 9% were Black or African American, and 6% were Asian; 8% identified as Hispanic or Latino. At baseline, subjects had average current episode of hair loss of approximately 4 years, with 59% of subjects having complete or near complete scalp hair loss (defined as ≥95% scalp hair loss). The mean pooled baseline SALT scores across treatment groups ranged from 85.9 to 88.6 with a mean duration of current episode of hair loss of ranging 3.7 to 3.9 years. Approximately 73% of subjects had eyebrow hair involvement and 70% of subjects had eyelash hair involvement.
The primary endpoint for both trials assessed the proportion of subjects who achieved at least 80% scalp hair coverage (SALT score of ≤20) at Week 24. Key secondary outcomes included the percentage of responders (defined as "satisfied" or "very satisfied") at Week 24 on the Satisfaction of Hair Patient-Reported Outcome (SPRO) and the percentage of subjects achieving an absolute SALT score of ≤20 at Week 20, 16, 12, and 8.
Upon completion of the 24-week trials, subjects were eligible to enroll in a long-term extension trial.
Clinical Response
Assessment of scalp hair loss was based on the SALT score. At Week 24, a greater proportion of subjects had a SALT ≤20 response (80% or more scalp hair) and SALT ≤10 response (90% or more scalp hair) with LEQSELVI 8 mg twice daily compared to placebo (Table 3).
Table 3. Clinical Response at Week 24 in Adult Subjects with Severe AA in Trials AA-1 and AA-2:
| Trial AA-1 | Trial AA-2 | |||
| Placebo (N=140) | LEQSELVI 8 mg twice daily (N=351) | Placebo (N=127) | LEQSELVI 8 mg twice daily (N=249) | |
| SALT scores ≤20 Common risk difference from Placebo (95% CI) | 1% | 29% 28% (23%, 33%) | 1% | 32% 31% (25%, 37%) |
| SALT scores ≤10 Common risk difference from Placebo (95% CI) | 0%a | 20% 21% (16%, 25%)a | 0%a | 24% 24% (19%, 30%) a |
a Not adjusted for multiplicity.
Table 4. Evaluation of Patient Satisfaction with Scalp Hair Coverage at Weeks 24 in Adult Subjects with Severe AA in Trials AA-1 and AA-2:
| Trial AA-1 | Trial AA-2 | |||
| Placebo (N=140) | LEQSELVI 8 mg twice daily (N=351) | Placebo (N=127) | LEQSELVI 8 mg twice daily (N=249) | |
| "Very Satisfied"a | 2% | 19% | 0% | 18% |
| "Satisfied"a | 3% | 23% | 2% | 28% |
| "Neither Satisfied nor Dissatisfied" | 16% | 19% | 13% | 15% |
| "Dissatisfied" | 25% | 18% | 18% | 16% |
| "Very Dissatisfied" | 54% | 21% | 67% | 23% |
a In Trial AA-1, the proportion of responders (defined as subjects who were "satisfied" or "very satisfied") on LEQSELVI was 42% compared to 5% on placebo. In Trial AA-2, the proportion of responders on LEQSELVI was 46% compared to 2% on placebo.
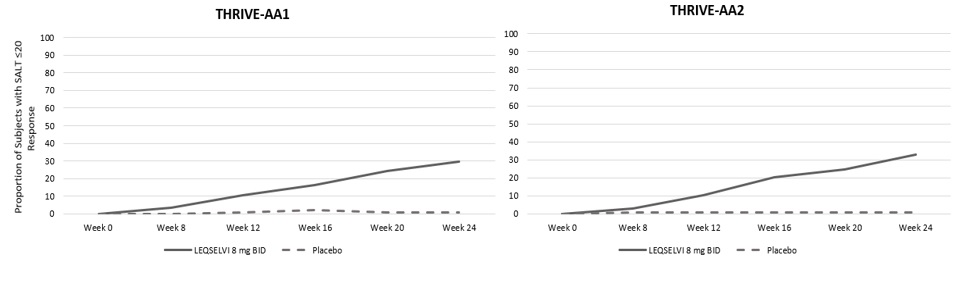
Figure 1. Clinical Response over Time in Adult Subjects with Severe AA in Trials AA-1 and AA-2:
The efficacy of LEQSELVI was generally comparable across multiple subgroups including age, gender, and body weight among these subgroups. The results for SALT score ≤20 at Week 24 by baseline scalp hair loss severity are presented in Table 5.
Table 5. Adult Subjects with Severe AA with Absolute SALT Scores ≤20 at Week 24 by Baseline Scalp Hair Loss Severity in Trials AA-1 and AA-2:
| Trials AA-1 and AA-2 | ||
| Placebo | LEQSELVI 8 mg BID | |
| 50% to 94% Scalp Hair Loss | ||
| N SALT ≤20 | 110 2% | 248 46% |
| 95% to 100% Scalp Hair Loss | ||
| N SALT ≤20 | 157 0% | 352 20% |
BID = twice-daily
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.