Source: European Medicines Agency (EU) Revision Year: 2019 Publisher: Regeneron Ireland Designated Activity Company (DAC), Europa House, Harcourt Centre, Harcourt Street, Dublin 2, Ireland
Hypersensitivity to the active substance or to any of the excipients listed in section 6.1.
In order to improve the traceability of biological medicinal products, the name and the batch number of the administered product should be clearly recorded.
Severe and fatal immune-related adverse reactions have been observed with cemiplimab (see section 4.8). These immune-related reactions may involve any organ system. Most immune-related reactions initially manifest during treatment with cemiplimab; however, immune-related adverse reactions can occur after discontinuation of cemiplimab.
Immune-related adverse reactions should be managed with cemiplimab treatment modifications, hormone replacement therapy (if clinically indicated), and corticosteroids. For suspected immune-related adverse reactions, patients should be evaluated to confirm an immune-related adverse reaction and to exclude other possible causes. Depending upon the severity of the adverse reaction, cemiplimab should be withheld or permanently discontinued (see section 4.2).
Immune-related pneumonitis, defined as requiring use of corticosteroids with no clear alternate aetiology, including fatal cases, has been observed in patients receiving cemiplimab (see section 4.8). Patients should be monitored for signs and symptoms of pneumonitis. Patients with suspected pneumonitis should be evaluated with radiographic imaging as indicated based on clinical evaluation and managed with cemiplimab treatment modifications and corticosteroids. (see section 4.2).
Immune-related diarrhoea or colitis, defined as requiring use of corticosteroids with no clear alternate aetiology, has been observed in patients receiving cemiplimab (see section 4.8). Patients should be monitored for signs and symptoms of diarrhoea or colitis and managed with cemiplimab treatment modifications, anti-diarrhoeal agents, and corticosteroids (see section 4.2).
Immune-related hepatitis, defined as requiring use of corticosteroids with no clear alternate aetiology, including fatal cases, has been observed in patients receiving cemiplimab (see section 4.8). Patients should be monitored for abnormal liver tests prior to and periodically during treatment as indicated based on clinical evaluation and managed with cemiplimab treatment modifications and corticosteroids (see section 4.2).
Immune-related endocrinopathies, defined as treatment-emergent endocrinopathies with no clear alternate aetiology, have been observed in patients receiving cemiplimab (see section 4.8).
Immune-related thyroid disorders have been observed in patients receiving cemiplimab. Thyroid disorders can occur at any time during the treatment. Patients should be monitored for changes in thyroid function at the start of treatment and periodically during the treatment as indicated based on clinical evaluation (see section 4.8). Patients should be managed with hormone replacement therapy (if indicated) and cemiplimab treatment modifications. Hyperthyroidism should be managed according to standard medical practice (see section 4.2).
Immune-related hypophysitis has been observed in patients receiving cemiplimab (see section 4.8). Patients should be monitored for signs and symptoms of hypophysitis and managed with cemiplimab treatment modifications and corticosteroids (see section 4.2).
Adrenal insufficiency has been observed in patients receiving cemiplimab (see section 4.8). Patients should be monitored for signs and symptoms of adrenal insufficiency during and after treatment and managed with cemiplimab treatment modifications and corticosteroids (see section 4.2).
Immune-related type 1 diabetes mellitus, including diabetic ketoacidosis, has been observed in patients receiving cemiplimab (see section 4.8). Patients should be monitored for hyperglycaemia and signs and symptoms of diabetes as indicated based on clinical evaluation and managed with oral anti-hyperglycaemics or insulin and cemiplimab treatment modifications (see section 4.2).
Cemiplimab should be withheld and anti-hyperglycaemics or insulin should be administered in patients with severe or life-threatening (Grade ≥ 3) hyperglycaemia. Cemiplimab should be resumed when metabolic control is achieved on insulin replacement or anti-hyperglycaemics (see section 4.2).
Immune-related skin adverse reactions, defined as requiring use of systemic corticosteroids with no clear alternate aetiology, including severe cutaneous adverse reactions (SCARs), such as Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN) (some cases with fatal outcome), and other skin reactions such as rash, erythema multiforme, pemphigoid, have been reported in association with cemiplimab treatment (see section 4.8).
Patients should be monitored for evidence of suspected severe skin reactions and exclude other causes. Patients should be managed with cemiplimab treatment modifications and corticosteroids (see section 4.2).
Cases of SJS, fatal TEN and stomatitis occurred following 1 dose of cemiplimab in patients with prior exposure to idelalisib, who were participating in a clinical trial evaluating cemiplimab in Non-Hodgkin Lymphoma (NHL), and who had recent exposure to sulfa containing antibiotics (see section 4.8). Patients should be managed with cemiplimab treatment modifications and corticosteroids as described above (see section 4.2).
Immune-related nephritis, defined as requiring use of corticosteroids with no clear alternate aetiology, has been observed in patients receiving cemiplimab (see section 4.8). Patients should be managed with cemiplimab treatment modifications and corticosteroids (see section 4.2).
Other fatal and life-threatening immune-related adverse reactions have been observed in patients receiving cemiplimab including paraneoplastic encephalomyelitis and meningitis (see section 4.8 for other immune-related adverse reactions).
Patients should be monitored for signs and symptoms of immune-related adverse reactions and managed with cemiplimab treatment modifications and corticosteroids (see section 4.2).
Cemiplimab can cause severe or life-threatening infusion-related reactions (see section 4.8). Patients should be monitored for signs and symptoms of infusion-related reactions and managed with cemiplimab treatment modifications and corticosteroids. Cemiplimab should be interrupted or the rate of infusion slowed for mild or moderate infusion-related reactions. The infusion should be stopped and cemiplimab should be permanently discontinued for severe (Grade 3) or life-threatening (Grade 4) infusion-related reactions (see section 4.2).
Patients that had active infections or that were immunocompromised were not included in the main study. For a full list of patients excluded from clinical trials, see section 5.1.
In the absence of data, cemiplimab should be used with caution in these populations after careful evaluation of the balance of benefits and risks for the patient.
No pharmacokinetic drug-drug interaction studies have been conducted with cemiplimab.
The use of systemic corticosteroids or immunosuppressants before starting cemiplimab, except for physiological doses of systemic corticosteroid (≤10 mg/day prednisone or equivalent), should be avoided because of their potential interference with the pharmacodynamic activity and efficacy of cemiplimab. However, systemic corticosteroids or other immunosuppressants can be used after starting cemiplimab to treat immune-related adverse reactions (see sections 4.2).
Women of childbearing potential should use effective contraception during treatment with cemiplimab and for at least 4 months after the last dose of cemiplimab.
Animal reproduction studies have not been conducted with cemiplimab. There are no available data on the use of cemiplimab in pregnant women. Animal studies have demonstrated that inhibition of the PD-1/PD-L1 pathway can lead to increased risk of immune-mediated rejection of the developing foetus resulting in foetal death (see section 5.3).
Human IgG4 is known to cross the placental barrier and cemiplimab is an IgG4; therefore, cemiplimab has the potential to be transmitted from the mother to the developing foetus. Cemiplimab is not recommended during pregnancy and in women of childbearing potential not using effective contraception unless the clinical benefit outweighs the potential risk.
It is unknown whether cemiplimab is secreted in human milk. It is known that antibodies (including IgG4) are secreted in human milk; a risk to the breast-feeding newborns/infants cannot be excluded.
If a woman chooses to be treated with cemiplimab, she should be instructed not to breast-feed while being treated with cemiplimab and for at least 4 months after the last dose.
No clinical data are available on the possible effects of cemiplimab on fertility. No effects on fertility assessment parameters or in the male and female reproductive organs were observed in a 3-month repeat dose fertility assessment study with sexually mature cynomolgus monkeys.
Cemiplimab has no or negligible influence on the ability to drive and use machines. Fatigue has been reported following treatment with cemiplimab (see section 4.8).
Immune-related adverse reactions can occur with cemiplimab. Most of these, including severe reactions, resolved following initiation of appropriate medical therapy or withdrawal of cemiplimab (see “Description of selected adverse reactions” below).
The safety of cemiplimab has been evaluated in 591 patients with advanced solid malignancies including 219 advanced CSCC patients who received cemiplimab monotherapy in 2 clinical studies (R2810-ONC-1423 and R2810-ONC-1540). Immune-related adverse reactions occurred in 20.1% of patients treated with cemiplimab in clinical trials including Grade 5 (0.7%), Grade 4 (1.2%) and Grade 3 (6.1%). Immune-related adverse reactions led to permanent discontinuation of cemiplimab in 4.4% of patients. The most common immune-related adverse reactions were hypothyroidism (7.1%), pneumonitis (3.7%), immune-related skin adverse reactions (2.0%), hyperthyroidism (1.9%) and hepatitis (1.9%) (see “Description of selected adverse reactions” below, Special warnings and precautions for use in section 4.4 and Recommended treatment modifications in section 4.2). Adverse reactions were serious in 8.6% patients and led to permanent discontinuation of cemiplimab in 5.8% of patients.
Severe cutaneous adverse reactions (SCARs), including Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN) have been reported in association with cemiplimab treatment (see section 4.4).
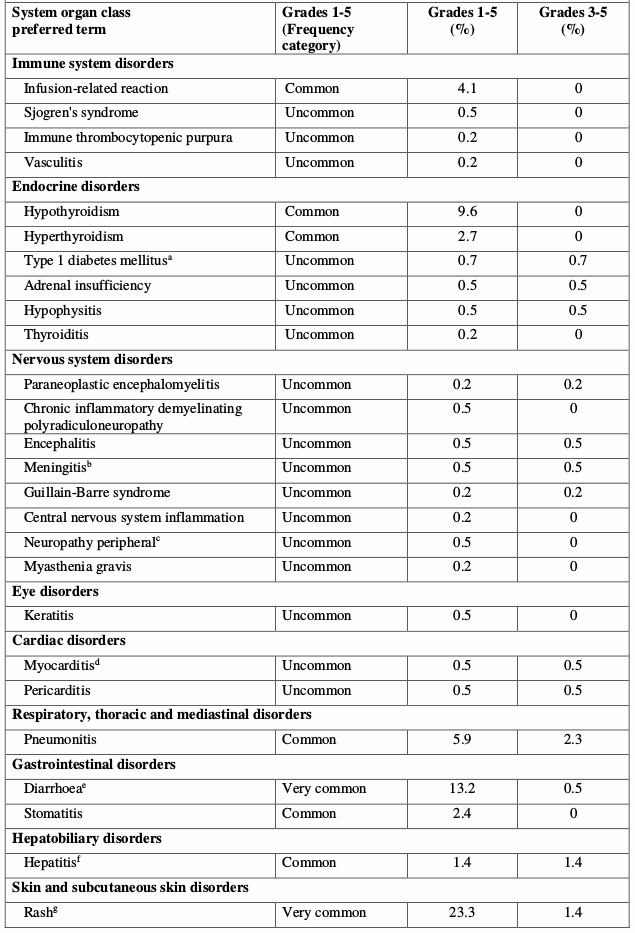
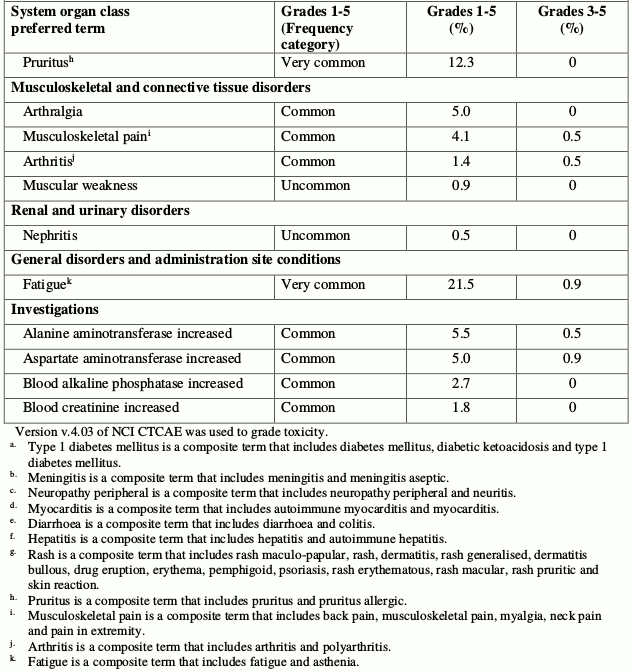
Listed in Table 2 are adverse reactions by system organ class and by frequency. Frequencies are defined as: very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1,000 to <1/100); rare (≥1/10,000 to <1/1,000); very rare (<1/10,000); not known (cannot be estimated from available data). Within each frequency grouping, adverse reactions are presented in the order of decreasing seriousness.
Table 2. Tabulated list of adverse reactions in patients treated with cemiplimab:
The selected adverse reactions described below are based on safety of cemiplimab in 591 patients in uncontrolled clinical studies.
Immune-related pneumonitis occurred in 22 (3.7%) of 591 patients receiving cemiplimab, including 2 (0.3%) patients with Grade 5, 2 (0.3%) patients with Grade 4, and 6 (1.0%) patients with Grade 3 pneumonitis. Immune-related pneumonitis led to permanent discontinuation of cemiplimab in 11 (1.9%) of 591 patients. Among the 22 patients with immune-related pneumonitis, the median time to onset was 3.8 months (range: 7 days to 18 months) and the median duration of pneumonitis was 21.5 days (range: 5 days to 6.5 months). Eighteen patients (3.0%) received high-dose corticosteroids for a median of 8.5 days (range: 1 day to 5.9 months). Resolution of pneumonitis had occurred in 14 (63.6%) of the 22 patients at the time of data cut-off.
Immune-related diarrhoea or colitis occurred in 7 (1.2%) of 591 patients receiving cemiplimab including 2 (0.3%) with Grade 3 immune-related diarrhoea or colitis. Immune-related diarrhoea or colitis led to permanent discontinuation of cemiplimab in 1 (0.2%) of 591 patients. Among the 7 patients with immune-related diarrhoea or colitis, the median time to onset was 3.8 months (range: 15 days to 6.0 months) and the median duration of immune-related diarrhoea or colitis was 30 days (range: 4 days to 8.6 months). Four patients (0.7%) with immune-related diarrhoea or colitis received high-dose corticosteroids for a median of 29 days (range: 19 days to 2.0 months). Resolution of immune-related diarrhoea or colitis had occurred in 4 (57.1%) of the 7 patients at the time of data cut-off.
Immune-related hepatitis occurred in 11 (1.9%) of 591 patients receiving cemiplimab including 1 (0.2%) patient with Grade 5, 1 (0.2%) patient with Grade 4, and 9 (1.5%) patients with Grade 3 immune-related hepatitis. Immune-related hepatitis led to permanent discontinuation of cemiplimab in 5 (0.8%) of 591 patients. Among the 11 patients with immune-related hepatitis, the median time to onset was 1.0 month (range: 7 days to 4.2 months) and the median duration of hepatitis was 15 days (range: 8 days to 2.7 months). Ten (1.7%) patients with immune-related hepatitis received high-dose corticosteroids for a median of 10.5 days (range: 2 days to 1.9 months). Resolution of hepatitis had occurred in 8 (72.7%) of the 11 patients at the time of data cut-off.
Hypothyroidism occurred in 42 (7.1%) of 591 patients receiving cemiplimab including 1 (0.2%) patient with Grade 3 hypothyroidism. No patient discontinued cemiplimab due to hypothyroidism. Among the 42 patients with hypothyroidism, the median time to onset was 4.2 months (range: 15 days to 18.9 months).
Hyperthyroidism occurred in 11 (1.9%) of 591 patients receiving cemiplimab including 1 (0.2%) patient with Grade 3 hyperthyroidism. No patient discontinued cemiplimab due to hyperthyroidism. Among the 11 patients with hyperthyroidism, the median time to onset was 1.9 months (range: 28 days to 14.8 months).
Adrenal insufficiency occurred in 3 (0.5%) of 591 patients receiving cemiplimab including 1 (0.2%) patient with Grade 3 adrenal insufficiency. No patient discontinued cemiplimab due to adrenal insufficiency. Among the 3 patients with adrenal insufficiency, the median time to onset was 11.5 months (range: 10.4 months to 12.3 months). One of the 3 patients was treated with systemic corticosteroids.
Immune-related hypophysitis occurred in 1 (0.2%) of 591 patients receiving cemiplimab. The event was Grade 3 hypophysitis.
Type 1 diabetes mellitus without an alternative aetiology occurred in 4 (0.7%) of 591 patients including 3 (0.5%) patients with Grade 4 and 1 (0.2%) patient with Grade 3 type 1 diabetes mellitus. Type 1 diabetes mellitus led to permanent discontinuation of cemiplimab in 1 (0.2%) of 591 patients. Among the 4 patients with type 1 diabetes mellitus, the median time to onset was 2.3 months (range: 28 days to 6.2 months).
Immune-related skin adverse reactions occurred in 12 (2.0%) of 591 patients receiving cemiplimab including 6 (1.0%) patients with Grade 3 immune-related skin adverse reactions. Immune-related skin adverse reactions led to permanent discontinuation of cemiplimab in 2 (0.3%) of 591 patients. Among the 12 patients with immune-related skin adverse reactions, the median time to onset was 1.5 months (range: 2 days to 10.9 months) and the median duration was 4.4 months (range: 14 days to 9.6 months). Nine patients (1.5%) with immune-related skin adverse reactions received high-dose corticosteroids for a median of 16 days (range: 7 days to 2.6 months). Resolution had occurred in 6 (50%) of 12 patients at the time of data cut-off.
Immune-related nephritis occurred in 3 (0.5%) of 591 patients receiving cemiplimab including 2 (0.3%) patients with Grade 3 immune-related nephritis. Immune-related nephritis led to permanent discontinuation of cemiplimab in 1 (0.2%) of 591 patients. Among the 3 patients with immune-related nephritis, the median time to onset was 1.8 months (range: 29 days to 4.1 months) and the median duration of nephritis was 18 days (range: 9 days to 29 days). Two (0.3%) patients with immune-related nephritis received high-dose corticosteroids for a median of 1.5 months (range: 16 days to 2.6 months). Resolution of nephritis had occurred in all patients at the time of data cut-off.
The following clinically significant, immune-related adverse reactions occurred at an incidence of less than 1% of 591 patients treated with cemiplimab. The events were Grade 3 or less unless stated otherwise:
Nervous system disorders: Meningitisa (Grade 4), Paraneoplastic encephalomyelitis (Grade 5), Guillain-Barre syndrome, central nervous system inflammation, Chronic inflammatory demyelinating polyradiculoneuropathy, Encephalitisb, Myasthenia gravis, Neuropathy peripheral.
Cardiac Disorders: Myocarditisc, Pericarditis
Immune system disorders: Immune thrombocytopenic purpura
Vascular disorders: Vasculitis
Musculoskeletal and connective tissue disorders: Myalgia, Arthritisd, Sjogren’s syndrome
Eye disorders: Keratitis
Gastrointestinal disorders: Stomatitis
a includes meningitis and meningitis aseptic
b includes encephalitis and noninfective encephalitis
c includes autoimmune myocarditis and myocarditis
d includes arthritis and polyarthritis
Infusion-related reactions occurred in 54 (9.1%) of 591 patients treated with cemiplimab including 1 (0.2%) patient with Grade 3 infusion-related reaction. Infusion-related reaction led to permanent discontinuation of cemiplimab in 2 (0.3%) patients. The most common symptoms of infusion-related reaction were nausea, pyrexia, vomiting, abdominal pain, chills and flushing. All patients recovered from the infusion-related reaction.
As with all therapeutic proteins, there is a potential for immunogenicity with cemiplimab. Five out of 398 patients (1.3%) administered cemiplimab developed treatment-emergent antibodies, with 1 out of 398 patients (0.3%) exhibiting persistent antibody responses. No neutralizing antibodies have been observed. There was no evidence of an altered pharmacokinetic or safety profile with anti-cemiplimab antibody development.
Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via the national reporting system listed in Appendix V.
In the absence of compatibility studies, this medicinal product must not be mixed with other medicinal products except those mentioned in section 6.6.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.