LOVENOX Solution for injection Ref.[10865] Active ingredients: Enoxaparin
Source: FDA, National Drug Code (US) Revision Year: 2020
12.1. Mechanism of Action
Enoxaparin is a low molecular weight heparin which has antithrombotic properties.
12.2. Pharmacodynamics
In humans, enoxaparin given at a dose of 1.5 mg/kg subcutaneously is characterized by a higher ratio of anti-Factor Xa to anti-Factor IIa activity (mean ±SD, 14.0±3.1) (based on areas under anti-Factor activity versus time curves) compared to the ratios observed for heparin (mean ±SD, 1.22±0.13). Increases of up to 1.8 times the control values were seen in the thrombin time (TT) and the activated partial thromboplastin time (aPTT). Enoxaparin at a 1 mg/kg dose (100 mg/mL concentration), administered subcutaneously every 12 hours to patients in a large clinical trial resulted in aPTT values of 45 seconds or less in the majority of patients (n=1607). A 30 mg intravenous bolus immediately followed by a 1 mg/kg subcutaneous administration resulted in aPTT postinjection values of 50 seconds. The average aPTT prolongation value on Day 1 was about 16% higher than on Day 4.
12.3. Pharmacokinetics
Absorption
Pharmacokinetic trials were conducted using the 100 mg/mL formulation. Maximum anti-Factor Xa and anti-thrombin (anti-Factor IIa) activities occur 3 to 5 hours after subcutaneous injection of enoxaparin. Mean peak anti-Factor Xa activity was 0.16 IU/mL (1.58 mcg/mL) and 0.38 IU/mL (3.83 mcg/mL) after the 20 mg and the 40 mg clinically tested subcutaneous doses, respectively. Mean (n=46) peak anti-Factor Xa activity was 1.1 IU/mL at steady state in patients with unstable angina receiving 1 mg/kg subcutaneously every 12 hours for 14 days. Mean absolute bioavailability of enoxaparin, after 1.5 mg/kg given subcutaneously, based on anti-Factor Xa activity is approximately 100% in healthy subjects.
A 30 mg intravenous bolus immediately followed by 1 mg/kg subcutaneously every 12 hours provided initial peak anti-Factor Xa levels of 1.16 IU/mL (n=16) and average exposure corresponding to 84% of steady-state levels. Steady state is achieved on the second day of treatment.
Enoxaparin pharmacokinetics appears to be linear over the recommended dosage ranges [see Dosage and Administration (2)]. After repeated subcutaneous administration of 40 mg once daily and 1.5 mg/kg once-daily regimens in healthy volunteers, the steady state is reached on day 2 with an average exposure ratio about 15% higher than after a single dose. Steady-state enoxaparin activity levels are well predicted by single-dose pharmacokinetics. After repeated subcutaneous administration of the 1 mg/kg twice-daily regimen, the steady state is reached from day 4 with mean exposure about 65% higher than after a single dose and mean peak and trough levels of about 1.2 and 0.52 IU/mL, respectively. Based on enoxaparin sodium pharmacokinetics, this difference in steady state is expected and within the therapeutic range.
Although not studied clinically, the 150 mg/mL concentration of enoxaparin sodium is projected to result in anticoagulant activities similar to those of 100 mg/mL and 200 mg/mL concentrations at the same enoxaparin dose. When a daily 1.5 mg/kg subcutaneous injection of enoxaparin sodium was given to 25 healthy male and female subjects using a 100 mg/mL or a 200 mg/mL concentration the following pharmacokinetic profiles were obtained (see Table 13).
Table 13. Pharmacokinetic Parameters* After 5 Days of 1.5 mg/kg Subcutaneous Once-Daily Doses of Enoxaparin Sodium Using 100 mg/mL or 200 mg/mL Concentrations:
| Concentration | Anti-Xa | Anti-IIa | Heptest | aPTT | |
|---|---|---|---|---|---|
| Amax (IU/mL or Δ sec) | 100 mg/mL | 1.37 (±0.23) | 0.23 (±0.05) | 105 (±17) | 19 (±5) |
| 200 mg/mL | 1.45 (±0.22) | 0.26 (±0.05) | 111 (±17) | 22 (±7) | |
| 90% CI | 102%–110% | 102%–111% | |||
| tmax† (h) | 100 mg/mL | 3 (2–6) | 4 (2–5) | 2.5 (2–4.5) | 3 (2–4.5) |
| 200 mg/mL | 3.5 (2–6) | 4.5 (2.5–6) | 3.3 (2–5) | 3 (2–5) | |
| AUC (ss) (h*IU/mL or h* Δ sec) | 100 mg/mL | 14.26 (±2.93) | 1.54 (±0.61) | 1321 (±219) | |
| 200 mg/mL | 15.43 (±2.96) | 1.77 (±0.67) | 1401 (±227) | ||
| 90% CI | 105%–112% | 103%–109% |
* Means ±SD at Day 5 and 90% Confidence Interval (CI) of the ratio
† Median (range)
Distribution
The volume of distribution of anti-Factor Xa activity is about 4.3 L.
Elimination
Following intravenous dosing, the total body clearance of enoxaparin is 26 mL/min. After intravenous dosing of enoxaparin labeled with the gamma-emitter, 99mTc, 40% of radioactivity and 8 to 20% of anti-Factor Xa activity were recovered in urine in 24 hours. Elimination half-life based on anti-Factor Xa activity was 4.5 hours after a single subcutaneous dose to about 7 hours after repeated dosing. Significant anti-Factor Xa activity persists in plasma for about 12 hours following a 40 mg subcutaneous once a day dose.
Following subcutaneous dosing, the apparent clearance (CL/F) of enoxaparin is approximately 15 mL/min.
Metabolism
Enoxaparin sodium is primarily metabolized in the liver by desulfation and/or depolymerization to lower molecular weight species with much reduced biological potency. Renal clearance of active fragments represents about 10% of the administered dose and total renal excretion of active and non-active fragments 40% of the dose.
Special Populations
Gender
Apparent clearance and Amax derived from anti-Factor Xa values following single subcutaneous dosing (40 mg and 60 mg) were slightly higher in males than in females. The source of the gender difference in these parameters has not been conclusively identified; however, body weight may be a contributing factor.
Geriatric
Apparent clearance and Amax derived from anti-Factor Xa values following single and multiple subcutaneous dosing in geriatric subjects were close to those observed in young subjects. Following once a day subcutaneous dosing of 40 mg enoxaparin, the Day 10 mean area under anti-Factor Xa activity versus time curve (AUC) was approximately 15% greater than the mean Day 1 AUC value [see Dosage and Administration (2.4) and Use in Specific Populations (8.5)].
Renal impairment
A linear relationship between anti-Factor Xa plasma clearance and creatinine clearance at steady state has been observed, which indicates decreased clearance of enoxaparin sodium in patients with reduced renal function. Anti-Factor Xa exposure represented by AUC, at steady state, is marginally increased in patients with creatinine clearance 50 to 80 mL/min and patients with creatinine clearance 30 to <50 mL/min after repeated subcutaneous 40 mg once-daily doses. In patients with severe renal impairment (creatinine clearance <30 mL/min), the AUC at steady state is significantly increased on average by 65% after repeated subcutaneous 40 mg once-daily doses [see Dosage and Administration (2.3) and Use in Specific Populations (8.7)].
Hemodialysis
In a single study, elimination rate appeared similar but AUC was two-fold higher than control population, after a single 0.25 or 0.5 mg/kg intravenous dose.
Hepatic impairment
Studies with Lovenox in patients with hepatic impairment have not been conducted and the impact of hepatic impairment on the exposure to enoxaparin is unknown.
Weight
After repeated subcutaneous 1.5 mg/kg once-daily dosing, mean AUC of anti-Factor Xa activity is marginally higher at steady state in obese healthy volunteers (BMI 30–48 kg/m²) compared to non-obese control subjects, while Amax is not increased.
When non–weight-adjusted dosing was administered, it was found after a single-subcutaneous 40 mg dose, that anti-Factor Xa exposure is 52% higher in low-weight women (<45 kg) and 27% higher in low-weight men (<57 kg) when compared to normal weight control subjects [see Use in Specific Populations (8.8)].
Pharmacokinetic Interaction
No pharmacokinetic interaction was observed between Lovenox and thrombolytics when administered concomitantly.
13. Nonclinical Toxicology
13.3 Reproductive and Developmental Toxicology
Teratology studies have been conducted in pregnant rats and rabbits at subcutaneous doses of enoxaparin up to 30 mg/kg/day corresponding to 211 mg/m²/day and 410 mg/m²/day in rats and rabbits respectively. There was no evidence of teratogenic effects or fetotoxicity due to enoxaparin.
13.1. Carcinogenesis, Mutagenesis, Impairment of Fertility
No long-term studies in animals have been performed to evaluate the carcinogenic potential of enoxaparin. Enoxaparin was not mutagenic in in vitro tests, including the Ames test, mouse lymphoma cell forward mutation test, and human lymphocyte chromosomal aberration test, and the in vivo rat bone marrow chromosomal aberration test. Enoxaparin was found to have no effect on fertility or reproductive performance of male and female rats at subcutaneous doses up to 20 mg/kg/day or 141 mg/m²/day. The maximum human dose in clinical trials was 2.0 mg/kg/day or 78 mg/m²/day (for an average body weight of 70 kg, height of 170 cm, and body surface area of 1.8 m²).
13.2. Animal Toxicology and/or Pharmacology
A single subcutaneous dose of 46.4 mg/kg enoxaparin was lethal to rats. The symptoms of acute toxicity were ataxia, decreased motility, dyspnea, cyanosis, and coma.
14. Clinical Studies
14.1 Prophylaxis of Deep Vein Thrombosis following Abdominal Surgery in Patients at Risk for Thromboembolic Complications
Abdominal surgery patients at risk include those who are over 40 years of age, obese, undergoing surgery under general anesthesia lasting longer than 30 minutes or who have additional risk factors such as malignancy or a history of deep vein thrombosis (DVT) or pulmonary embolism (PE).
In a double-blind, parallel group study of patients undergoing elective cancer surgery of the gastrointestinal, urological, or gynecological tract, a total of 1116 patients were enrolled in the study, and 1115 patients were treated. Patients ranged in age from 32 to 97 years (mean age 67 years) with 52.7% men and 47.3% women. Patients were 98% Caucasian, 1.1% Black, 0.4% Asian and 0.4% others. Lovenox 40 mg subcutaneously, administered once a day, beginning 2 hours prior to surgery and continuing for a maximum of 12 days after surgery, was comparable to heparin 5000 U every 8 hours subcutaneously in reducing the risk of DVT. The efficacy data are provided below (see Table 14).
Table 14. Efficacy of Lovenox in the Prophylaxis of Deep Vein Thrombosis Following Abdominal Surgery:
| Dosing Regimen | ||
|---|---|---|
| Indication | Lovenox 40 mg daily subcutaneously n (%) | Heparin 5000 U q8h subcutaneously n (%) |
| All Treated Abdominal Surgery Patients | 555 (100) | 560 (100) |
| Treatment Failures | ||
| Total VTE* (%) | 56 (10.1) (95% CI†: 8 to 13) | 63 (11.3) (95% CI: 9 to 14) |
| DVT Only (%) | 54 (9.7) (95% CI: 7 to 12) | 61 (10.9) (95% CI: 8 to 13) |
* VTE = Venous thromboembolic events which included DVT, PE, and death considered to be thromboembolic in origin
† CI = Confidence Interval
In a second double-blind, parallel group study, Lovenox 40 mg subcutaneously once a day was compared to heparin 5000 U every 8 hours subcutaneously in patients undergoing colorectal surgery (one-third with cancer). A total of 1347 patients were randomized in the study and all patients were treated. Patients ranged in age from 18 to 92 years (mean age 50.1 years) with 54.2% men and 45.8% women. Treatment was initiated approximately 2 hours prior to surgery and continued for approximately 7 to 10 days after surgery. The efficacy data are provided below (see Table 15).
Table 15. Efficacy of Lovenox in the Prophylaxis of Deep Vein Thrombosis Following Colorectal Surgery:
| Dosing Regimen | ||
|---|---|---|
| Indication | Lovenox 40 mg daily subcutaneously n (%) | Heparin 5000 U q8h subcutaneously n (%) |
| All Treated Colorectal Surgery Patients | 673 (100) | 674 (100) |
| Treatment Failures | ||
| Total VTE* (%) | 48 (7.1) (95% CI†: 5 to 9) | 45 (6.7) (95% CI: 5 to 9) |
| DVT Only (%) | 47 (7.0) (95% CI: 5 to 9) | 44 (6.5) (95% CI: 5 to 8) |
* VTE = Venous thromboembolic events which included DVT, PE, and death considered to be thromboembolic in origin
† CI = Confidence Interval
14.2 Prophylaxis of Deep Vein Thrombosis following Hip or Knee Replacement Surgery
Lovenox has been shown to reduce the risk of postoperative deep vein thrombosis (DVT) following hip or knee replacement surgery.
In a double-blind study, Lovenox 30 mg every 12 hours subcutaneously was compared to placebo in patients with hip replacement. A total of 100 patients were randomized in the study and all patients were treated. Patients ranged in age from 41 to 84 years (mean age 67.1 years) with 45% men and 55% women. After hemostasis was established, treatment was initiated 12 to 24 hours after surgery and was continued for 10 to 14 days after surgery. The efficacy data are provided below (see Table 16).
Table 16. Efficacy of Lovenox in the Prophylaxis of Deep Vein Thrombosis Following Hip Replacement Surgery:
| Dosing Regimen | ||
|---|---|---|
| Indication | Lovenox 30 mg q12h subcutaneously n (%) | Placebo q12h subcutaneously n (%) |
| All Treated Hip Replacement Patients | 50 (100) | 50 (100) |
| Treatment Failures | ||
| Total DVT (%) | 5 (10)* | 23 (46) |
| Proximal DVT (%) | 1 (2)† | 11 (22) |
* p value versus placebo = 0.0002
† p value versus placebo = 0.0134
A double-blind, multicenter study compared three dosing regimens of Lovenox in patients with hip replacement. A total of 572 patients were randomized in the study and 568 patients were treated. Patients ranged in age from 31 to 88 years (mean age 64.7 years) with 63% men and 37% women. Patients were 93% Caucasian, 6% Black, <1% Asian, and 1% others. Treatment was initiated within two days after surgery and was continued for 7 to 11 days after surgery. The efficacy data are provided below (see Table 17).
Table 17. Efficacy of Lovenox in the Prophylaxis of Deep Vein Thrombosis Following Hip Replacement Surgery:
| Dosing Regimen | |||
|---|---|---|---|
| Indication | 10 mg daily subcutaneously n (%) | 30 mg q12h subcutaneously n (%) | 40 mg daily subcutaneously n (%) |
| All Treated Hip Replacement Patients | 161 (100) | 208 (100) | 199 (100) |
| Treatment Failures | |||
| Total DVT (%) | 40 (25) | 22 (11)* | 27 (14) |
| Proximal DVT (%) | 17 (11) | 8 (4)† | 9 (5) |
* p value versus Lovenox 10 mg once a day = 0.0008
† p value versus Lovenox 10 mg once a day = 0.0168
There was no significant difference between the 30 mg every 12 hours and 40 mg once a day regimens. In a double-blind study, Lovenox 30 mg every 12 hours subcutaneously was compared to placebo in patients undergoing knee replacement surgery. A total of 132 patients were randomized in the study and 131 patients were treated, of which 99 had total knee replacement and 32 had either unicompartmental knee replacement or tibial osteotomy. The 99 patients with total knee replacement ranged in age from 42 to 85 years (mean age 70.2 years) with 36.4% men and 63.6% women. After hemostasis was established, treatment was initiated 12 to 24 hours after surgery and was continued up to 15 days after surgery. The incidence of proximal and total DVT after surgery was significantly lower for Lovenox compared to placebo. The efficacy data are provided below (see Table 18).
Table 18. Efficacy of Lovenox in the Prophylaxis of Deep Vein Thrombosis Following Total Knee Replacement Surgery:
| Dosing Regimen | ||
|---|---|---|
| Indication | Lovenox 30 mg q12h subcutaneously n (%) | Placebo q12h subcutaneously n (%) |
| All Treated Total Knee Replacement Patients | 47 (100) | 52 (100) |
| Treatment Failures | ||
| Total DVT (%) | 5 (11)* (95% CI†: 1 to 21) | 32 (62) (95% CI: 47 to 76) |
| Proximal DVT (%) | 0 (0)‡ (95% Upper CL§: 5) | 7 (13) (95% CI: 3 to 24) |
* p value versus placebo = 0.0001
† CI = Confidence Interval
‡ p value versus placebo = 0.013
§ CL = Confidence Limit
Additionally, in an open-label, parallel group, randomized clinical study, Lovenox 30 mg every 12 hours subcutaneously in patients undergoing elective knee replacement surgery was compared to heparin 5000 U every 8 hours subcutaneously. A total of 453 patients were randomized in the study and all were treated. Patients ranged in age from 38 to 90 years (mean age 68.5 years) with 43.7% men and 56.3% women. Patients were 92.5% Caucasian, 5.3% Black, and 0.6% others. Treatment was initiated after surgery and continued up to 14 days. The incidence of deep vein thrombosis was lower for Lovenox compared to heparin.
Extended Prophylaxis of Deep Vein Thrombosis Following Hip Replacement Surgery: In a study of extended prophylaxis for patients undergoing hip replacement surgery, patients were treated, while hospitalized, with Lovenox 40 mg subcutaneously, initiated up to 12 hours prior to surgery for the prophylaxis of postoperative DVT. At the end of the peri-operative period, all patients underwent bilateral venography. In a double-blind design, those patients with no venous thromboembolic disease were randomized to a post-discharge regimen of either Lovenox 40 mg (n=90) once a day subcutaneously or to placebo (n=89) for 3 weeks. A total of 179 patients were randomized in the double-blind phase of the study and all patients were treated. Patients ranged in age from 47 to 87 years (mean age 69.4 years) with 57% men and 43% women. In this population of patients, the incidence of DVT during extended prophylaxis was significantly lower for Lovenox compared to placebo. The efficacy data are provided below (see Table 19).
Table 19. Efficacy of Lovenox in the Extended Prophylaxis of Deep Vein Thrombosis Following Hip Replacement Surgery:
| Post-discharge Dosing Regimen | ||
|---|---|---|
| Indication (Post Discharge) | Lovenox 40 mg daily subcutaneously n (%) | Placebo daily subcutaneously n (%) |
| All Treated Extended Prophylaxis Patients | 90 (100) | 89 (100) |
| Treatment Failures | ||
| Total DVT (%) | 6 (7)* (95% CI†: 3 to 14) | 18 (20) (95% CI: 12 to 30) |
| Proximal DVT (%) | 5 (6)‡ (95% CI: 2 to 13) | 7 (8) (95% CI: 3 to 16) |
* p value versus placebo = 0.008
† CI = Confidence Interval
‡ p value versus placebo = 0.537
In a second study, patients undergoing hip replacement surgery were treated, while hospitalized, with Lovenox 40 mg subcutaneously, initiated up to 12 hours prior to surgery. All patients were examined for clinical signs and symptoms of venous thromboembolic (VTE) disease. In a double-blind design, patients without clinical signs and symptoms of VTE disease were randomized to a post-discharge regimen of either Lovenox 40 mg (n=131) once a day subcutaneously or to placebo (n=131) for 3 weeks. A total of 262 patients were randomized in the study double-blind phase and all patients were treated. Patients ranged in age from 44 to 87 years (mean age 68.5 years) with 43.1% men and 56.9% women. Similar to the first study the incidence of DVT during extended prophylaxis was significantly lower for Lovenox compared to placebo, with a statistically significant difference in both total DVT (Lovenox 21 [16%] versus placebo 45 [34%]; p=0.001) and proximal DVT (Lovenox 8 [6%] versus placebo 28 [21%]; p=<0.001).
14.3 Prophylaxis of Deep Vein Thrombosis in Medical Patients with Severely Restricted Mobility during Acute Illness
In a double blind multicenter, parallel group study, Lovenox 20 mg or 40 mg once a day subcutaneously was compared to placebo in the prophylaxis of deep vein thrombosis (DVT) in medical patients with severely restricted mobility during acute illness (defined as walking distance of <10 meters for ≤3 days). This study included patients with heart failure (NYHA Class III or IV); acute respiratory failure or complicated chronic respiratory insufficiency (not requiring ventilatory support): acute infection (excluding septic shock); or acute rheumatic disorder (acute lumbar or sciatic pain, vertebral compression [due to osteoporosis or tumor], acute arthritic episodes of the lower extremities). A total of 1102 patients were enrolled in the study, and 1073 patients were treated. Patients ranged in age from 40 to 97 years (mean age 73 years) with equal proportions of men and women. Treatment continued for a maximum of 14 days (median duration 7 days). When given at a dose of 40 mg once a day subcutaneously, Lovenox significantly reduced the incidence of DVT as compared to placebo. The efficacy data are provided below (see Table 20).
Table 20. Efficacy of Lovenox in the Prophylaxis of Deep Vein Thrombosis in Medical Patients with Severely Restricted Mobility during Acute Illness:
| Dosing Regimen | |||
|---|---|---|---|
| Lovenox 20 mg daily subcutaneously | Lovenox 40 mg daily subcutaneously | Placebo | |
| Indication | n (%) | n (%) | n (%) |
| All Treated Medical Patients During Acute Illness | 351 (100) | 360 (100) | 362 (100) |
| Treatment Failure* | |||
| Total VTE† (%) | 43 (12.3) | 16 (4.4) | 43 (11.9) |
| Total DVT (%) | 43 (12.3) (95% CI‡ 8.8 to 15.7) | 16 (4.4) (95% CI‡ 2.3 to 6.6) | 41 (11.3) (95% CI‡ 8.1 to 14.6) |
| Proximal DVT (%) | 13 (3.7) | 5 (1.4) | 14 (3.9) |
* Treatment failures during therapy, between Days 1 and 14
† VTE = Venous thromboembolic events which included DVT, PE, and death considered to be thromboembolic in origin
‡ CI = Confidence Interval
At approximately 3 months following enrollment, the incidence of venous thromboembolism remained lower in the Lovenox 40 mg treatment group versus the placebo treatment group.
14.4 Treatment of Deep Vein Thrombosis with or without Pulmonary Embolism
In a multicenter, parallel group study, 900 patients with acute lower extremity deep vein thrombosis (DVT) with or without pulmonary embolism (PE) were randomized to an inpatient (hospital) treatment of either (i) Lovenox 1.5 mg/kg once a day subcutaneously, (ii) Lovenox 1 mg/kg every 12 hours subcutaneously, or (iii) heparin intravenous bolus (5000 IU) followed by a continuous infusion (administered to achieve an aPTT of 55 to 85 seconds). A total of 900 patients were randomized in the study and all patients were treated. Patients ranged in age from 18 to 92 years (mean age 60.7 years) with 54.7% men and 45.3% women. All patients also received warfarin sodium (dose adjusted according to PT to achieve an International Normalization Ratio [INR] of 2.0 to 3.0), commencing within 72 hours of initiation of Lovenox or standard heparin therapy, and continuing for 90 days. Lovenox or standard heparin therapy was administered for a minimum of 5 days and until the targeted warfarin sodium INR was achieved. Both Lovenox regimens were equivalent to standard heparin therapy in reducing the risk of recurrent venous thromboembolism (DVT and/or PE). The efficacy data are provided below (see Table 21).
Table 21. Efficacy of Lovenox in Treatment of Deep Vein Thrombosis with or without Pulmonary Embolism:
| Dosing Regimen* | |||
|---|---|---|---|
| Lovenox 1.5 mg/kg daily subcutaneously | Lovenox 1 mg/kg q12h subcutaneously | Heparin aPTT Adjusted Intravenous Therapy | |
| Indication | n (%) | n (%) | n (%) |
| All Treated DVT Patients with or without PE | 298 (100) | 312 (100) | 290 (100) |
| Patient Outcome | |||
| Τotal VTE† (%) | 13 (4.4)‡ | 9 (2.9)‡ | 12 (4.1) |
| DVT Only (%) | 11 (3.7) | 7 (2.2) | 8 (2.8) |
| Proximal DVT (%) | 9 (3.0) | 6 (1.9) | 7 (2.4) |
| PE (%) | 2 (0.7) | 2 (0.6) | 4 (1.4) |
* All patients were also treated with warfarin sodium commencing within 72 hours of Lovenox or standard heparin therapy.
† VTE = venous thromboembolic event (DVT and/or PE)
‡ The 95% Confidence Intervals for the treatment differences for total
VTE were:
Lovenox once a day versus heparin (-3.0 to 3.5)
Lovenox every 12 hours versus heparin (-4 .2 to 1.7)
Similarly, in a multicenter, open-label, parallel group study, patients with acute proximal DVT were randomized to Lovenox or heparin. Patients who could not receive outpatient therapy were excluded from entering the study. Outpatient exclusion criteria included the following: inability to receive outpatient heparin therapy because of associated comorbid conditions or potential for non-compliance and inability to attend follow-up visits as an outpatient because of geographic inaccessibility. Eligible patients could be treated in the hospital, but ONLY Lovenox patients were permitted to go home on therapy (72%). A total of 501 patients were randomized in the study and all patients were treated. Patients ranged in age from 19 to 96 years (mean age 57.8 years) with 60.5% men and 39.5% women. Patients were randomized to either Lovenox 1 mg/kg every 12 hours subcutaneously or heparin intravenous bolus (5000 IU) followed by a continuous infusion administered to achieve an aPTT of 60 to 85 seconds (in-patient treatment). All patients also received warfarin sodium as described in the previous study. Lovenox or standard heparin therapy was administered for a minimum of 5 days. Lovenox was equivalent to standard heparin therapy in reducing the risk of recurrent venous thromboembolism. The efficacy data are provided below (see Table 22).
Table 22. Efficacy of Lovenox in Treatment of Deep Vein Thrombosis:
| Dosing Regimen* | ||
|---|---|---|
| Lovenox 1 mg/kg q12h subcutaneously | Heparin aPTT Adjusted Intravenous Therapy | |
| Indication | n (%) | n (%) |
| All Treated DVT Patients | 247 (100) | 254 (100) |
| Patient Outcome | ||
| Total VTE† (%) | 13 (5.3)‡ | 17 (6.7) |
| DVT Only (%) | 11 (4.5) | 14 (5.5) |
| Proximal DVT (%) | 10 (4.0) | 12 (4.7) |
| PE (%) | 2 (0.8) | 3 (1.2) |
* All patients were also treated with warfarin sodium commencing on the evening of the second day of Lovenox or standard heparin therapy.
† VTE = venous thromboembolic event (deep vein thrombosis [DVT] and/or pulmonary embolism [PE]).
‡ The 95% Confidence Intervals for the treatment difference for total VTE was: Lovenox versus heparin (-5.6 to 2.7).
14.5 Prophylaxis of Ischemic Complications in Unstable Angina and Non–Q-Wave Myocardial Infarction
In a multicenter, double-blind, parallel group study, patients who recently experienced unstable angina or non–Q-wave myocardial infarction were randomized to either Lovenox 1 mg/kg every 12 hours subcutaneously or heparin intravenous bolus (5000 U) followed by a continuous infusion (adjusted to achieve an aPTT of 55 to 85 seconds). A total of 3171 patients were enrolled in the study, and 3107 patients were treated. Patients ranged in age from 25 to 94 years (median age 64 years), with 33.4% of patients female and 66.6% male. Race was distributed as follows: 89.8% Caucasian, 4.8% Black, 2.0% Asian, and 3.5% other. All patients were also treated with aspirin 100 to 325 mg per day. Treatment was initiated within 24 hours of the event and continued until clinical stabilization, revascularization procedures, or hospital discharge, with a maximal duration of 8 days of therapy. The combined incidence of the triple endpoint of death, myocardial infarction, or recurrent angina was lower for Lovenox compared with heparin therapy at 14 days after initiation of treatment. The lower incidence of the triple endpoint was sustained up to 30 days after initiation of treatment. These results were observed in an analysis of both all-randomized and all-treated patients. The efficacy data are provided below (see Table 23).
Table 23. Efficacy of Lovenox in the Prophylaxis of Ischemic Complications in Unstable Angina and Non–Q-Wave Myocardial Infarction (combined endpoint of death, myocardial infarction, or recurrent angina):
| Dosing Regimen* | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Lovenox 1 mg/kg q12h subcutaneous | Heparin aPTT Adjusted Intravenous Therapy | Reduction (%) | p Value | ||||||
| Indication | n (%) | n (%) | All Treated Unstable Angina and Non–Q-Wave MI Patients | 1578 (100) | 1529 (100) | ||||
| Time point† | |||||||||
| 48 Hours | 96 (6.1) | 112 (7.3) | 1.2 | 0.120 | |||||
| 14 Days | 261 (16.5) | 303 (19.8) | 3.3 | 0.017 | |||||
| 30 Days | 313 (19.8) | 358 (23.4) | 3.6 | 0.014 | |||||
* All patients were also treated with aspirin 100 to 325 mg per day.
† Evaluation time points are after initiation of treatment. Therapy continued for up to 8 days (median duration of 2.6 days).
The combined incidence of death or myocardial infarction at all time points was lower for Lovenox compared to standard heparin therapy, but did not achieve statistical significance. The efficacy data are provided below (see Table 24).
Table 24. Efficacy of Lovenox in the Prophylaxis of Ischemic Complications in Unstable Angina and Non–Q-Wave Myocardial Infarction (Combined endpoint of death or myocardial infarction):
| Dosing Regimen* | ||||
|---|---|---|---|---|
| Lovenox 1 mg/kg q12h subcutaneously | Heparin aPTT Adjusted Intravenous Therapy | Reduction (%) | p Value | |
| Indication | n (%) | n (%) | ||
| All Treated Unstable Angina and Non–Q-Wave MI Patients | 1578 (100) | 1529 (100) | ||
| Time point† | ||||
| 48 Hours | 16 (1.0) | 20 (1.3) | 0.3 | 0.126 |
| 14 Days | 76 (4.8) | 93 (6.1) | 1.3 | 0.115 |
| 30 Days | 96 (6.1) | 118 (7.7) | 1.6 | 0.069 |
* All patients were also treated with aspirin 100 to 325 mg per day.
† Evaluation time points are after initiation of treatment. Therapy continued for up to 8 days (median duration of 2.6 days).
In a survey one year following treatment, with information available for 92% of enrolled patients, the combined incidence of death, myocardial infarction, or recurrent angina remained lower for Lovenox versus heparin (32.0% vs 35.7%).
Urgent revascularization procedures were performed less frequently in the Lovenox group as compared to the heparin group, 6.3% compared to 8.2% at 30 days (p=0.047).
14.6 Treatment of Acute ST-Segment Elevation Myocardial Infarction
In a multicenter, double-blind, double-dummy, parallel-group study, patients with acute ST-segment elevation myocardial infarction (STEMI) who were to be hospitalized within 6 hours of onset and were eligible to receive fibrinolytic therapy were randomized in a 1:1 ratio to receive either Lovenox or unfractionated heparin.
Study medication was initiated between 15 minutes before and 30 minutes after the initiation of fibrinolytic therapy. Unfractionated heparin was administered beginning with an intravenous bolus of 60 U/kg (maximum 4000 U) and followed with an infusion of 12 U/kg per hour (initial maximum 1000 U per hour) that was adjusted to maintain an aPTT of 1.5 to 2 times the control value. The intravenous infusion was to be given for at least 48 hours. The Lovenox dosing strategy was adjusted according to the patient's age and renal function. For patients younger than 75 years of age, Lovenox was given as a single 30 mg intravenous bolus plus a 1 mg/kg subcutaneous dose followed by a subcutaneous injection of 1 mg/kg every 12 hours. For patients at least 75 years of age, the intravenous bolus was not given and the subcutaneous dose was reduced to 0.75 mg/kg every 12 hours. For patients with severe renal insufficiency (estimated creatinine clearance of less than 30 mL per minute), the dose was to be modified to 1 mg/kg every 24 hours. The subcutaneous injections of Lovenox were given until hospital discharge or for a maximum of eight days (whichever came first). The mean treatment duration for Lovenox was 6.6 days. The mean treatment duration of unfractionated heparin was 54 hours.
When percutaneous coronary intervention was performed during study medication period, patients received antithrombotic support with blinded study drug. For patients on Lovenox, the PCI was to be performed on Lovenox (no switch) using the regimen established in previous studies, i.e. no additional dosing, if the last subcutaneous administration was less than 8 hours before balloon inflation, intravenous bolus of 0.3 mg/kg Lovenox if the last subcutaneous administration was more than 8 hours before balloon inflation.
All patients were treated with aspirin for a minimum of 30 days. Eighty percent of patients received a fibrin-specific agent (19% tenecteplase, 5% reteplase and 55% alteplase) and 20% received streptokinase.
Among 20,479 patients in the ITT population, the mean age was 60 years, and 76% were male. Racial distribution was: 87% Caucasian, 9.8% Asian, 0.2% Black, and 2.8% other. Medical history included previous MI (13%), hypertension (44%), diabetes (15%) and angiographic evidence of CAD (5%). Concomitant medication included aspirin (95%), beta-blockers (86%), ACE inhibitors (78%), statins (70%) and clopidogrel (27%). The MI at entry was anterior in 43%, non-anterior in 56%, and both in 1%.
The primary efficacy endpoint was the composite of death from any cause or myocardial re-infarction in the first 30 days after randomization. Total follow-up was one year.
The rate of the primary efficacy endpoint (death or myocardial re-infarction) was 9.9% in the Lovenox group, and 12% in the unfractionated heparin group, a 17% reduction in the relative risk, (P=0.000003) (see Table 25).
Table 25. Efficacy of Lovenox in the Treatment of Acute ST-Segment Elevation Myocardial Infarction:
| Lovenox (N=10,256) n (%) | UFH (N=10,223) n (%) | Relative Risk (95% CI) | P Value | |
|---|---|---|---|---|
| Outcome at 48 hours | ||||
| Death or Myocardial Re-infarction | 478 (4.7) | 531 (5.2) | 0.90 (0.80 to 1.01) | 0.08 |
| Death | 383 (3.7) | 390 (3.8) | 0.98 (0.85 to 1.12) | 0.76 |
| Myocardial Re-infarction | 102 (1.0) | 156 (1.5) | 0.65 (0.51 to 0.84) | <0.001 |
| Urgent Revascularization | 74 (0.7) | 96 (0.9) | 0.77 (0.57 to 1.04) | 0.09 |
| Death or Myocardial Re-infarction or Urgent Revascularization | 548 (5.3) | 622 (6.1) | 0.88 (0.79 to 0.98) | 0.02 |
| Outcome at 8 Days | ||||
| Death or Myocardial Re-infarction | 740 (7.2) | 954 (9.3) | 0.77 (0.71 to 0.85) | <0.001 |
| Death | 559 (5.5) | 605 (5.9) | 0.92 (0.82 to 1.03) | 0.15 |
| Myocardial Re-infarction | 204 (2.0) | 379 (3.7) | 0.54 (0.45 to 0.63) | <0.001 |
| Urgent Revascularization | 145 (1.4) | 247 (2.4) | 0.59 (0.48 to 0.72) | <0.001 |
| Death or Myocardial Re-infarction or Urgent Revascularization | 874 (8.5) | 1181 (11.6) | 0.74 (0.68 to 0.80) | <0.001 |
| Outcome at 30 Days | ||||
| Primary efficacy endpoint (Death or Myocardial Re-infarction) | 1017 (9.9) | 1223 (12.0) | 0.83 (0.77 to 0.90) | 0.000003 |
| Death | 708 (6.9) | 765 (7.5) | 0.92 (0.84 to 1.02) | 0.11 |
| Myocardial Re-infarction | 352 (3.4) | 508 (5.0) | 0.69 (0.60 to 0.79) | <0.001 |
| Urgent Revascularization | 213 (2.1) | 286 (2.8) | 0.74 (0.62 to 0.88) | <0.001 |
| Death or Myocardial Re-infarction or Urgent Revascularization | 1199 (11.7) | 1479 (14.5) | 0.81 (0.75 to 0.87) | <0.001 |
Note: Urgent revascularization denotes episodes of recurrent myocardial ischemia (without infarction) leading to the clinical decision to perform coronary revascularization during the same hospitalization. CI denotes confidence intervals.
The beneficial effect of Lovenox on the primary endpoint was consistent across key subgroups including age, gender, infarct location, history of diabetes, history of prior myocardial infarction, fibrinolytic agent administered, and time to treatment with study drug (see Figure 1); however, it is necessary to interpret such subgroup analyses with caution.
Figure 1. Relative Risks of and Absolute Event Rates for the Primary Endpoint at 30 Days in Various Subgroups*
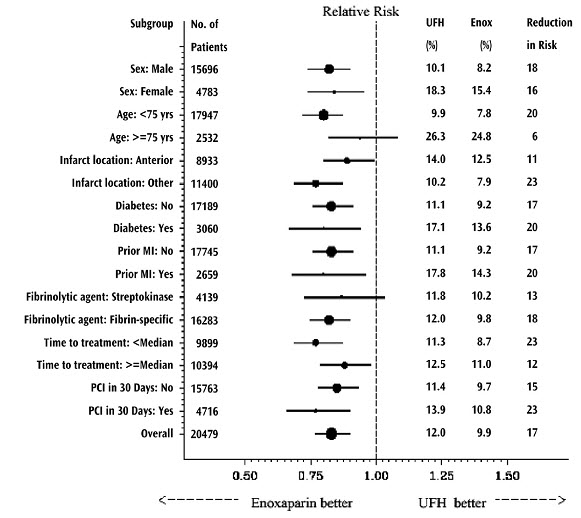
* The primary efficacy endpoint was the composite of death from any cause or myocardial re-infarction in the first 30 days. The overall treatment effect of Lovenox as compared to the unfractionated heparin is shown at the bottom of the figure. For each subgroup, the circle is proportional to the number and represents the point estimate of the treatment effect and the horizontal lines represent the 95% confidence intervals. Fibrin-specific fibrinolytic agents included alteplase, tenecteplase, and reteplase. Time to treatment indicates the time from the onset of symptoms to the administration of study drug (median: 3.2 hours).
The beneficial effect of Lovenox on the primary endpoint observed during the first 30 days was maintained over a 12 month follow-up period (see Figure 2).
Figure 2. Kaplan-Meier Plot – Death or Myocardial Re-infarction at 30 Days – ITT Population:
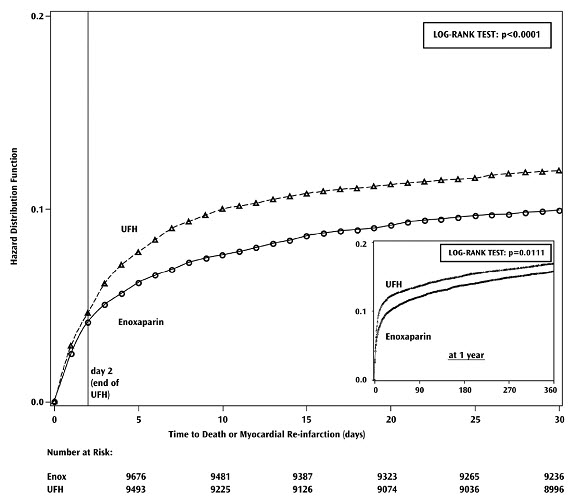
There is a trend in favor of Lovenox during the first 48 hours, but most of the treatment difference is attributed to a step increase in the event rate in the UFH group at 48 hours (seen in Figure 2), an effect that is more striking when comparing the event rates just prior to and just subsequent to actual times of discontinuation. These results provide evidence that UFH was effective and that it would be better if used longer than 48 hours. There is a similar increase in endpoint event rate when Lovenox was discontinued, suggesting that it too was discontinued too soon in this study.
The rates of major hemorrhages (defined as requiring 5 or more units of blood for transfusion, or 15% drop in hematocrit or clinically overt bleeding, including intracranial hemorrhage) at 30 days were 2.1% in the Lovenox group and 1.4% in the unfractionated heparin group. The rates of intracranial hemorrhage at 30 days were 0.8% in the Lovenox group and 0.7% in the unfractionated heparin group. The 30-day rate of the composite endpoint of death, myocardial re-infarction or ICH (a measure of net clinical benefit) was significantly lower in the Lovenox group (10.1%) as compared to the heparin group (12.2%).
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.