LYXUMIA Solution for injection Ref.[8550] Active ingredients: Lixisenatide
Source: European Medicines Agency (EU) Revision Year: 2023 Publisher: Sanofi Winthrop Industrie, 82 avenue Raspail, 94250 Gentilly, France
Pharmacodynamic properties
Pharmacotherapeutic group: Drugs used in Diabetes, Glucagon-like peptide-1 (GLP-1) analogues
ATC code: A10BJ03
Mechanism of action
Lixisenatide is a selective GLP-1 receptor agonist. The GLP-1 receptor is the target for native GLP-1, an endogenous incretin hormone that potentiates glucose-dependent insulin secretion from the pancreatic beta cells.
Lixisenatide action is mediated via a specific interaction with GLP-1 receptors, leading to an increase in intracellular cyclic adenosine monophosphate (cAMP). Lixisenatide stimulates insulin secretion when blood glucose is increased but not at normoglycaemia, which limits the risk of hypoglycaemia.
In parallel, glucagon secretion is suppressed. In case of hypoglycaemia, the rescue mechanism of glucagon secretion is preserved.
Lixisenatide slows gastric emptying thereby reducing the rate at which meal-derived glucose appears in the circulation.
Pharmacodynamic effects
When administered once daily, lixisenatide improves glycaemic control through the immediate and sustained effects of lowering both post-prandial and fasting glucose concentrations in patients with type 2 diabetes.
This effect on post-prandial glucose was confirmed in a 4-week study versus liraglutide 1.8 mg once a day in combination with metformin. Reduction from baseline in the AUC0:30-4:30h of plasma glucose after a test-meal was: -12.61 h*mmol/L (-227.25 h*mg/dl) in the lixisenatide group and -4.04 h*mmol/L (-72.83 h*mg/dl) in the liraglutide group. This was also confirmed in an 8-week study versus liraglutide, administered before breakfast, in combination with insulin glargine with or without metformin.
Clinical efficacy and safety
The clinical efficacy and safety of Lyxumia were evaluated in nine randomised double-blind, placebo-controlled clinical studies including 4,508 patients with type 2 diabetes (2,869 patients randomised to lixisenatide, 47.5% men and 52.5% women, and 517 were ≥65 years of age).
Efficacy of Lyxumia was also assessed in two randomised, open-label, active-controlled study (versus exenatide or versus insulin glulisine) and in a meal time study (in total 1,067 patients randomised to lixisenatide).
Efficacy and safety of Lyxumia in patients older than 70 years was addressed in a specifically dedicated placebo-controlled study (176 patients randomised to lixisenatide, including 62 patients ≥75 years of age).
In addition, a double-blind, placebo-controlled cardiovascular outcome study (ELIXA) enrolled 6,068 type 2 diabetes patients with previous acute coronary syndrome (3,034 randomised to lixisenatide, including 198 patients ≥75 years of age and 655 patients with moderate renal impairment).
In the completed Phase III studies, it was observed that approximately 90% of the patients were able to remain on the once daily maintenance dose of 20 mcg Lyxumia at the end of the main 24-week treatment period.
Glycaemic control
Add-on combination therapy with oral antidiabetics
Lyxumia in combination with metformin, a sulphonylurea, pioglitazone or a combination of these agents showed statistically significant reductions in HbA1c, in fasting plasma glucose and in 2-hour post-prandial glucose after a test-meal compared to placebo at the end of the main 24-week treatment period (tables 2 and 3). The HbA1c reduction was significant with once-daily administration, whether administered morning or evening.
This effect on HbA1c was sustained in long term studies for up to 76 weeks.
Add-on treatment to metformin alone
Table 2. Placebo-controlled studies in combination with metformin (24-week results):
| Metformin as background therapy | |||||
|---|---|---|---|---|---|
| Lixisenatide 20 mcg (N=160) | Placebo (N=159) | Lixisenatide 20 mcg | Placebo (N=170) | ||
| Morning (N=255) | Evening (N=255) | ||||
| Mean HbA1c (%) | |||||
| Baseline | 7.99 | 8.03 | 8.07 | 8.07 | 8.02 |
| LS mean change from baseline | -0.92 | -0.42 | -0.87 | -0.75 | -0.38 |
| Patients (%) achieving HbA1c <7% | 47.4 | 24.1 | 43.0 | 40.6 | 22.0 |
| Mean body weight (kg) | |||||
| Baseline | 90.30 | 87.86 | 90.14 | 89.01 | 90.40 |
| LS mean change from baseline | -2.63 | -1.63 | -2.01 | -2.02 | -1.64 |
In an active-controlled study, Lyxumia once daily showed an HbA1c reduction of -0.79% compared to -0.96% with exenatide twice daily at the end of the main 24-week treatment period with a mean treatment difference of 0.17% (95% CI: 0.033, 0.297) and a similar percentage of patients achieved an HbA1c less than 7% in the lixisenatide group (48.5%) and in the exenatide group (49.8%). The incidence of nausea was 24.5% in the lixisenatide group compared to 35.1% in the exenatide twice daily group and the incidence of symptomatic hypoglycaemia with lixisenatide was 2.5% during the 24-week main treatment period compared to 7.9% in the exenatide group.
In a 24-week open-label study, lixisenatide administered before the main meal of the day was non-inferior to lixisenatide administered before breakfast in terms of HbA1c reduction (LS mean change from baseline: -0.65% versus -0.74%). Similar HbA1c decreases were observed regardless of which meal was the main meal (breakfast, lunch or dinner). At the end of the study, 43.6% (main meal group) and 42.8% (breakfast group) of patients achieved an HbA1c less than 7%. Nausea was reported in 14.7% and 15.5% of patients, and symptomatic hypoglycaemia in 5.8% and 2.2% of patients, main meal group and breakfast group, respectively.
Add-on treatment to a sulphonylurea alone or in combination with metformin
Table 3. Placebo-controlled study in combination with a sulphonylurea (24-week results):
| Sulphonylurea as background therapy with or without metformin | ||
|---|---|---|
| Lixisenatide 20 mcg (N=570) | Placebo (N=286) | |
| Mean HbA1c (%) | ||
| Baseline | 8.28 | 8.22 |
| LS mean change from | -0.85 | -0.10 |
| Patients (%) achieving HbA1c <7% | 36.4 | 13.5 |
| Mean body weight (kg) | ||
| Baseline | 82.58 | 84.52 |
| LS mean change from | -1.76 | -0.93 |
Add-on treatment to pioglitazone alone or in combination with metformin
In a clinical study, the addition of lixisenatide to pioglitazone with or without metformin, in patients not adequately controlled with pioglitazone, resulted in an HbA1c decrease from baseline of 0.90%, compared to a decrease from baseline of 0.34% in the placebo group at the end of the 24-week main treatment period. At the end of the 24-week main treatment period, 52.3% of the lixisenatide patients achieved an HbA1c less than 7% compared to 26.4% in the placebo group.
During the 24-week main treatment period, nausea was reported in 23.5% in the lixisenatide group compared to 10.6% in the placebo group and symptomatic hypoglycaemia was reported in 3.4% of the lixisenatide patients compared to 1.2% in the placebo group.
Add-on combination therapy with a basal insulin
Lyxumia given with a basal insulin alone, or with a combination of a basal insulin and metformin, or a combination of a basal insulin and a sulphonylurea resulted in statistically significant reductions in HbA1c and in 2-hour post-prandial glucose after a test-meal compared to placebo.
Table 4. Placebo-controlled studies in combination with a basal insulin (24-week results):
| Basal insulin as background therapy Alone or in combination with metformin | Basal insulin as background therapy Alone or in combination with a sulphonylurea* | |||
|---|---|---|---|---|
| Alone or in combination with metformin | Alone or in combination with a sulphonylurea* | |||
| Lixisenatide 20 mcg (N=327) | Placebo (N=166) | Lixisenatide 20 mcg (N=154) | Placebo (N=157) | |
| Mean HbA1c (%) | ||||
| Baseline | 8.39 | 8.38 | 8.53 | 8.53 |
| LS mean change from baseline | -0.74 | -0.38 | -0.77 | 0.11 |
| Patients (%) achieving HbA1c <7% | 28.3 | 12.0 | 35.6 | 5.2 |
| Mean duration of treatment with basal insulin at baseline (years) | 3.06 | 3.2 | 2.94 | 3.01 |
| Mean change in basal insulin dose (U) | ||||
| Baseline | 53.62 | 57.65 | 24.87 | 24.11 |
| LS mean change from baseline | -5.62 | -1.93 | -1.39 | -0.11 |
| Mean body weight (kg) | ||||
| Baseline | 87.39 | 89.11 | 65.99 | 65.60 |
| LS mean change from baseline | -1.80 | -0.52 | -0.38 | 0.06 |
* performed in Asian population
A clinical study was conducted in insulin-naive patients insufficiently controlled on oral antidiabetic agents. This study consisted of a 12-week run-in period with introduction and titration of insulin glargine and of a 24-week treatment period during which patients receive either lixisenatide or placebo in combination with insulin glargine and metformin with or without thiazolidinediones. Insulin glargine was continuously titrated during this period. During the 12-week run-in period, addition and titration of insulin glargine resulted approximately in an HbA1c decrease of 1%. The addition of lixisenatide led to a significantly greater HbA1c decrease of 0.71% in the lixisenatide group compared to 0.40% in the placebo group. At the end of the 24-week treatment period, 56.3% of the lixisenatide patients achieved an HbA1c less than 7% compared to 38.5% in the placebo group.
During the 24-week treatment period, 22.4% lixisenatide patients reported at least one symptomatic hypoglycaemic event compared to 13.5% in the placebo group. The incidence of hypoglycaemia was mainly increased in the lixisenatide group during the first 6 weeks of treatment and thereafter, was similar to the placebo group.
Patients with type 2 diabetes with basal insulin combined with 1-3 oral anti-diabetic agents were enrolled in an open-label randomised study for insulin intensification. After 12-week of optimal insulin glargine titration with or without metformin, inadequately controlled patients were randomised to add single dose of lixisenatide or a single dose (QD) of insulin glulisine (both before the largest meal) or insulin glulisine administered three times a day (TID) for 26 weeks.
The level of HbA1c reduction was comparable between groups (table 5).
As opposed to both insulin glulisine treatment regimens, lixisenatide reduced body weight (table 5). The rate of symptomatic hypoglycaemic events was lower with lixisenatide (36%) compared to insulin glulisine QD and TID (47% and 52%, respectively).
Table 5. Active-controlled study in combination with basal insulin with or without metformin (26-week results) - (mITT) and safety population:
| Lixisenatide | Insulin glulisine QD | Insulin glulisine TID | |
|---|---|---|---|
| Mean HbA1c (%) | N=297 | N=298 | N=295 |
| LS change from baseline | -0.63 | -0.58 | -0.84 |
| LS mean difference (SE) of lixisenatide versus 95% CI | -0.05 (0.059) (-0.170 to 0.064) | 0.21 (0.059) (0.095 to 0.328) | |
| Mean body weight | N=297 | N=298 | N=295 |
| LS change from baseline | -0.63 | +1.03 | +1.37 |
| LS mean difference (SE) of lixisenatide versus 95% CI | -1.66 (0.305) (-2.257 to -1.062) | -1.99 (0.305) (-2.593 to -1.396)* |
* p<0.0001
Fasting plasma glucose The reductions in fasting plasma glucose obtained with Lyxumia treatment ranged from 0.42 mmol/L to 1.19 mmol/L (7.6 to 21.4 mg/dl) from baseline at the end of the main 24-week treatment period in placebo-controlled studies.
Post-prandial glucose
Treatment with Lyxumia resulted in reductions in 2-hour post-prandial glucose after a test-meal statistically superior to placebo whatever the background treatment.
The reductions with Lyxumia ranged from 4.51 to 7.96 mmol/L (81.2 to 143.3 mg/dl) from baseline at the end of the main 24-week treatment period across all studies in which post-prandial glucose was measured; 26.2% to 46.8% of patients had a 2-hour post-prandial glucose value below 7.8 mmol/L (140.4 mg/dl). h3. Body weight
Treatment with Lyxumia in combination with metformin and/or a sulphonylurea resulted in a sustained body weight change from baseline in all controlled studies in a range from -1.76 kg to - 2.96 kg at the end of the main 24-week treatment period.
Body weight change from baseline in a range from -0.38 kg to -1.80 kg was also observed in lixisenatide patients receiving stable basal insulin dose, alone or in combination with metformin or a sulphonylurea.
In patients newly started on insulin, body weight remained almost unchanged in the lixisenatide group while an increase was shown in the placebo group.
Body weight reduction was sustained in long term studies up to 76 weeks. The body weight reduction is independent from the occurrence of nausea and vomiting.
Beta cell function
Clinical studies with Lyxumia indicate improved beta-cell function as measured by the homeostasis model assessment for beta-cell function (HOMA-β). Restoration of first phase insulin secretion and improved second phase insulin secretion in response to an intravenous bolus of glucose were demonstrated in patients with type 2 diabetes (n=20) after a single dose of Lyxumia.
Cardiovascular evaluation
No increase in mean heart rate in patients with type 2 diabetes was seen in all placebo controlled phase III studies.
Mean systolic and diastolic blood pressure reductions up to 2.1 mmHg and up to 1.5 mmHg respectively were observed in phase III placebo-controlled studies.
The ELIXA study was a randomized, double-blind, placebo-controlled, multinational study that evaluated cardiovascular (CV) outcomes during treatment with lixisenatide in patients with type 2 diabetes mellitus after a recent Acute Coronary Syndrome.
Overall, 6068 patients were randomized 1:1 to either placebo or lixisenatide 20 mcg (following a starting dose of 10 mcg during the first 2 weeks).
Ninety-six percent of the patients in both treatment groups completed the study in accordance with the protocol and the vital status was known at the end of the study for 99.0% and 98.6% of the patients in the lixisenatide and placebo group, respectively. Median treatment duration was 22.4 months in the lixisenatide group and 23.3 months in the placebo group, and the median duration of study follow-up was 25.8 and 25.7 months, respectively. Mean HbA1c (±SD) in the lixisenatide and placebo groups was 7.72 (±1.32)% and 7.64 (±1.28)% at baseline and 7.46 (±1.51)% and 7.61 (±1.48)% at 24 months, respectively.
The results of the primary and secondary composite efficacy endpoints, and the results of all the individual components of the composite endpoints are shown in Figure 1.
Figure 1. Forest plot: analyses of each individual cardiovascular event -- ITT population:
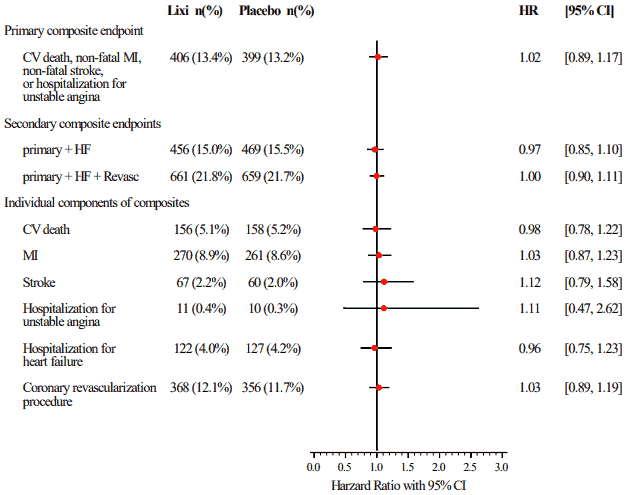
CV: cardiovascular, MI: myocardial infarction, HF: hospitalization for heart failure, Revasc: coronary revascularization procedure, HR: hazard ratio, CI: confidence interval.
Elderly
People aged ≥70 years
The efficacy and safety of lixisenatide in people aged ≥70 years with type 2 diabetes was evaluated in a double-blind, placebo-controlled study of 24 weeks duration. Frail patients, including patients at risk for malnutrition, patients with recent cardiovascular events and patients with moderate to severe cognitive impairment were excluded. A total of 350 patients were randomized (randomization ratio 1:1). Overall, 37% of the patients were ≥75 years old (N=131) and 31% had moderate renal impairment (N=107). Patients received stable dose(s) of oral antidiabetic drug(s) (OAD) and/or basal insulin as background therapy. Sulfonylureas or glinides were not used with basal insulin as background therapy.
Lixisenatide provided significant improvements in HbA1c (-0.64% change compared to placebo; 95% CI: -0.810% to -0.464%; p<0.0001), from a mean baseline HbA1c of 8.0%.
Paediatric population
The European Medicines Agency has deferred the obligation to submit the results of studies with Lyxumia in one or more subsets of the paediatric population in type 2 diabetes mellitus (see section 4.2 for information on paediatric use).
Pharmacokinetic properties
Absorption
Following subcutaneous administration to patients with type 2 diabetes, the rate of lixisenatide absorption is rapid and not influenced by the dose administered. Irrespective of the dose and whether lixisenatide was administered as single or multiple doses, the median tmax is 1 to 3.5 hours in patients with type 2 diabetes. There are no clinically relevant differences in the rate of absorption when lixisenatide is administered subcutaneously in the abdomen, thigh, or arm.
Distribution
Lixisenatide has a moderate level of binding (55%) to human proteins.
The apparent volume of distribution after subcutaneous administration of lixisenatide (Vz/F) is approximately 100 L.
Biotransformation and elimination
As a peptide, lixisenatide is eliminated through glomerular filtration, followed by tubular reabsorption and subsequent metabolic degradation, resulting in smaller peptides and amino acids, which are reintroduced in the protein metabolism.
After multiple dose administration in patients with type 2 diabetes, mean terminal half-life was approximately 3 hours and the mean apparent clearance (CL/F) about 35 L/h.
Special populations
Patients with renal impairment
In subjects with mild (creatinine clearance calculated by the Cockcroft-Gault formula 60-90 ml/min), moderate (creatinine clearance 30-60 ml/min) and severe renal impairment (creatinine clearance 15-30 ml/min), AUC was increased by 46%, 51% and 87%, respectively.
Patients with hepatic impairment
As lixisenatide is cleared primarily by the kidney, no pharmacokinetic study has been performed in patients with acute or chronic hepatic impairment. Hepatic dysfunction is not expected to affect the pharmacokinetics of lixisenatide.
Gender
Gender has no clinically relevant effect on the pharmacokinetics of lixisenatide.
Race
Ethnic origin had no clinically relevant effect on the pharmacokinetics of lixisenatide based on the results of pharmacokinetic studies in Caucasian, Japanese and Chinese subjects.
Elderly
Age has no clinically relevant effect on the pharmacokinetics of lixisenatide. In a pharmacokinetic study in elderly non-diabetic subjects, administration of lixisenatide 20 mcg resulted in a mean increase of lixisenatide AUC by 29% in the elderly population (11 subjects aged 65 to 74 years and 7 subjects aged ≥75 years) compared to 18 subjects aged 18 to 45 years, likely related to reduced renal function in the older age group.
Body weight
Body weight has no clinically relevant effect on lixisenatide AUC.
Preclinical safety data
Non-clinical data reveal no special hazards for humans based on conventional studies of safety pharmacology and toxicology.
In 2-year subcutaneous carcinogenicity studies, non-lethal C-cell thyroid tumours were seen in rats and mice and are considered to be caused by a non-genotoxic GLP-1 receptor-mediated mechanism to which rodents are particularly sensitive. C-cell hyperplasia and adenoma were seen at all doses in rats and a no observed adverse effect level (NOAEL) could be not defined. In mice, these effects occurred at exposure ratio above 9.3-fold when compared to human exposure at the therapeutic dose. No C-cell carcinoma was observed in mice and C-cell carcinoma occurred in rats with an exposure ratio relative to exposure at human therapeutic dose of about 900-fold. In 2-year subcutaneous carcinogenicity study in mice, 3 cases of adenocarcinoma in the endometrium were seen in the mid dose group with a statistically significant increase, corresponding to an exposure ratio of 97-fold. No treatment-related effect was demonstrated.
Animal studies did not indicate direct harmful effects with respect to male and female fertility in rats. Reversible testicular and epididymal lesions were seen in dogs treated with lixisenatide. No related effect on spermatogenesis was seen in healthy men.
In embryo-foetal development studies, malformations, growth retardation, ossification retardation and skeletal effects were observed in rats at all doses (5-fold exposure ratio compared to human exposure) and in rabbits at high doses (32-fold exposure ratio compared to human exposure) of lixisenatide. In both species, there was a slight maternal toxicity consisting of low food consumption and reduced body weight. Neonatal growth was reduced in male rats exposed to high doses of lixisenatide during late gestation and lactation, with a slightly increased pup mortality observed.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.