MARVELON Tablet Ref.[27523] Active ingredients: 17 alpha-Ethinylestradiol Desogestrel
Source: Medicines & Healthcare Products Regulatory Agency (GB) Revision Year: 2021 Publisher: Organon Pharma (UK) Limited, Hertford Road, Hoddesdon, Hertfordshire, EN11 9BU, UK
4.3. Contraindications
Combined hormonal contraceptives (CHCs) should not be used in the presence of any of the conditions listed below. Should any of the conditions appear for the first time during CHC use, the product should be stopped immediately.
- Presence or risk of venous thromboembolism (VTE)
- Venous thromboembolism – current VTE (on anticoagulants) or history of (e.g. deep venous thrombosis [DVT] or pulmonary embolism [PE]).
- Known hereditary or acquired predisposition for venous thromboembolism, such as APC-resistance, (including Factor V Leiden), antithrombin-III-deficiency, protein C deficiency, protein S deficiency.
- Major surgery with prolonged immobilisation (see section 4.4).
- A high risk of venous thromboembolism due to the presence of multiple risk factors (see section 4.4).
- Presence or risk of arterial thromboembolism (ATE)
- Arterial thromboembolism – current arterial thromboembolism, history of arterial thromboembolism (e.g. myocardial infarction) or prodromal condition (e.g. angina pectoris)
- Cerebrovascular disease – current stroke, history of stroke or prodromal condition (e.g. transient ischaemic attack, TIA).
- Known hereditary or acquired predisposition for arterial thromboembolism, such as hyperhomocysteinaemia and antiphospholipid-antibodies (anticardiolipin-antibodies, lupus anticoagulant).
- History of migraine with focal neurological symptoms.
- A high risk of arterial thromboembolism due to multiple risk factors (see section 4.4) or to the presence of one serious risk factor such as:
- diabetes mellitus with vascular symptoms
- severe hypertension
- severe dyslipoproteinaemia
- Pancreatitis or a history thereof if associated with severe hypertriglyceridaemia.
- Presence or history of severe hepatic disease as long as liver function values have not returned to normal.
- Presence or history of liver tumours (benign or malignant).
- Known or suspected estrogen-dependent tumours, (See 4.4 Special warnings and special precautions for use: The Pill and Cancer).
- Endometrial hyperplasia.
- Undiagnosed vaginal bleeding.
- Known or suspected pregnancy.
- Hypersensitivity to the active substances or to any of the excipients listed in section 6.1.
- Marvelon is contraindicated for concomitant use with medicinal products containing ombitasvir/paritaprevir/ritonavir and dasabuvir (see sections 4.4 and 4.5).
4.4. Special warnings and precautions for use
4.4.1 Warnings
If any of the conditions or risk factors mentioned below is present, the suitability of Marvelon should be discussed with the woman.
In the event of aggravation, or first appearance of any of these conditions or risk factors, the woman should be advised to contact her doctor to determine whether the use of Marvelon should be discontinued.
1. Circulatory Disorders
Risk of venous thromboembolism (VTE)
- The use of any combined hormonal contraceptive (CHC) increases the risk of venous thromboembolism (VTE) compared with no use. Products that contain levonorgestrel, norgestimate or norethisterone are associated with the lowest risk of VTE. Other products such as Marvelon may have up to twice this level of risk. The decision to use any product other than one with the lowest VTE risk should be taken only after a discussion with the woman to ensure she understands the risk of VTE with Marvelon, how her current risk factors influence this risk, and that her VTE risk is highest in the first ever year of use. There is also some evidence that the risk is increased when a CHC is re-started after a break in use of 4 weeks or more.
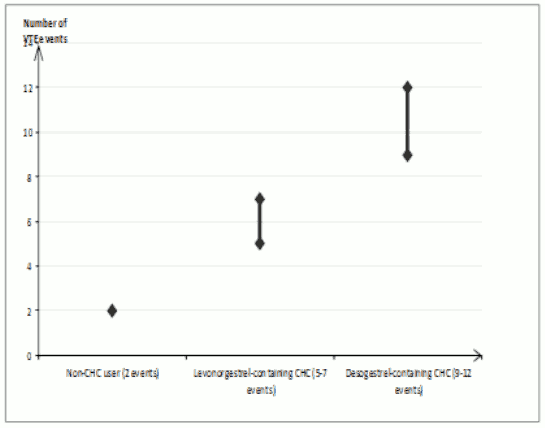
- In women who do not use a CHC and are not pregnant about 2 out of 10,000 will develop a VTE over the period of one year. However, in any individual woman the risk may be far higher, depending on her underlying risk factors (see below).
It is estimated1 that out of 10,000 women who use a CHC containing desogestrel between 9 and 12 women will develop a VTE in one year; this compares with about 62 in women who use a levonorgestrel-containing CHC.
In both cases, the number of VTEs per year is fewer than the number expected during pregnancy or in the postpartum period.
- VTE may be fatal in 1-2% of cases.
Number of VTE events per 10,000 women in one year:
Extremely rarely, thrombosis has been reported to occur in CHC users in other blood vessels, e.g. hepatic, mesenteric, renal or retinal veins and arteries.
Risk factors for VTE
The risk for venous thromboembolic complications in CHC users may increase substantially in a woman with additional risk factors, particularly if there are multiple risk factors (see table).
Marvelon is contraindicated if a woman has multiple risk factors that put her at high risk of venous thrombosis (see section 4.3). If a woman has more than one risk factor, it is possible that the increase in risk is greater than the sum of the individual factors – in this case her total risk of VTE should be considered. If the balance of benefits and risks is considered to be negative a CHC should not be prescribed (see section 4.3).
Table. Risk factors for VTE:
| Risk factor | Comment |
|---|---|
| Obesity (body mass index over 30 kg/m²) | Risk increases substantially as BMI rises. Particularly important to consider if other risk factors also present. |
| Prolonged immobilisation, major surgery, any surgery to the legs or pelvis, neurosurgery, or major trauma Note: Temporary immobilisation including air travel >4 hours can also be a risk factor for VTE, particularly in women with other risk factors. | In these situations it is advisable to discontinue use of the patch/pill/ring (in the case of elective surgery at least four weeks in advance) and not resume until two weeks after complete remobilisation. Another method of contraception should be used to avoid unintentional pregnancy. Antithrombotic treatment should be considered if Marvelon has not been discontinued in advance. |
| Positive family history (venous thromboembolism ever in a sibling or parent especially at a relatively early age e.g. before 50). | If a hereditary predisposition is suspected, the woman should be referred to a specialist for advice before deciding about any CHC use. |
| Other medical conditions associated with VTE | Cancer, systemic lupus erythematosus, haemolytic uraemic syndrome, chronic inflammatory bowel disease (Crohn's disease or ulcerative colitis) and sickle cell disease |
| Increasing age | Particularly above 35 years |
There is no consensus about the possible role of varicose veins and superficial thrombophlebitis in the onset or progression of venous thrombosis.
The increased risk of thromboembolism in pregnancy, and particularly the 6-week period of the puerperium, must be considered (for information on "Pregnancy and lactation" see section 4.6).
Symptoms of VTE (deep vein thrombosis and pulmonary embolism)
In the event of symptoms women should be advised to seek urgent medical attention and to inform the healthcare professional that she is taking a CHC.
Symptoms of deep vein thrombosis (DVT) can include:
- unilateral swelling of the leg and/or foot or along a vein in the leg;
- pain or tenderness in the leg which may be felt only when standing or walking;
- increased warmth in the affected leg; red or discoloured skin on the leg.
Symptoms of pulmonary embolism (PE) can include:
- sudden onset of unexplained shortness of breath or rapid breathing;
- sudden coughing which may be associated with haemoptysis;
- sharp chest pain;
- severe light headedness or dizziness;
- rapid or irregular heartbeat.
Some of these symptoms (e.g. "shortness of breath", "coughing") are non-specific and might be misinterpreted as more common or less severe events (e.g. respiratory tract infections).
Other signs of vascular occlusion can include: sudden pain, swelling and slight blue discoloration of an extremity.
If the occlusion occurs in the eye symptoms can range from painless blurring of vision which can progress to loss of vision. Sometimes loss of vision can occur almost immediately.
Risk of arterial thromboembolism (ATE)
Epidemiological studies have associated the use of CHCs with an increased risk for arterial thromboembolism (myocardial infarction) or for cerebrovascular accident (e.g. transient ischaemic attack, stroke). Arterial thromboembolic events may be fatal.
Risk factors for ATE
The risk of arterial thromboembolic complications or of a cerebrovascular accident in CHC users increases in women with risk factors (see table). Marvelon is contraindicated if a woman has one serious or multiple risk factors for ATE that puts her at high risk of arterial thrombosis (see section 4.3). If a woman has more than one risk factor, it is possible that the increase in risk is greater than the sum of the individual factors - in this case her total risk should be considered. If the balance of benefits and risks is considered to be negative a CHC should not be prescribed (see section 4.3).
Table. Risk factors for ATE:
| Risk factor | Comment |
|---|---|
| Increasing age | Particularly above 35 years |
| Smoking | Women should be advised not to smoke if they wish to use a CHC. Women over 35 who continue to smoke should be strongly advised to use a different method of contraception. |
| Hypertension | |
| Obesity (body mass index over 30 kg/m²) | Risk increases substantially as BMI increases. Particularly important in women with additional risk factors |
| Positive family history (arterial thromboembolism ever in a sibling or parent especially at relatively early age e.g. below 50). | If a hereditary predisposition is suspected, the woman should be referred to a specialist for advice before deciding about any CHC use. |
| Migraine | An increase in frequency or severity of migraine during CHC use (which may be prodromal of a cerebrovascular event) may be a reason for immediate discontinuation. |
| Other medical conditions associated with adverse vascular events | Diabetes mellitus, hyperhomocysteinaemia, valvular heart disease and atrial fibrillation, dyslipoproteinaemia and systemic lupus erythematosus. |
Symptoms of ATE
In the event of symptoms women should be advised to seek urgent medical attention and to inform the healthcare professional that she is taking a CHC.
Symptoms of a cerebrovascular accident can include:
- sudden numbness or weakness of the face, arm or leg, especially on one side of the body;
- sudden trouble walking, dizziness, loss of balance or coordination;
- sudden confusion, trouble speaking or understanding;
- sudden trouble seeing in one or both eyes;
- sudden, severe or prolonged headache with no known cause;
- loss of consciousness or fainting with or without seizure.
Temporary symptoms suggest the event is a transient ischaemic attack (TIA).
Symptoms of myocardial infarction (MI) can include:
- pain, discomfort, pressure, heaviness, sensation of squeezing or fullness in the chest, arm, or below the breastbone;
- discomfort radiating to the back, jaw, throat, arm, stomach;
- feeling of being full, having indigestion or choking;
- sweating, nausea, vomiting or dizziness;
- extreme weakness, anxiety, or shortness of breath;
- rapid or irregular heartbeats.
2. Tumours
An increased risk of cervical cancer in long term users of combined oral contraceptives has been reported in some studies, but there continues to be controversy about the extent to which this is attributable to the confounding effects of sexual behaviour and other factors such as human papilloma virus (HPV).
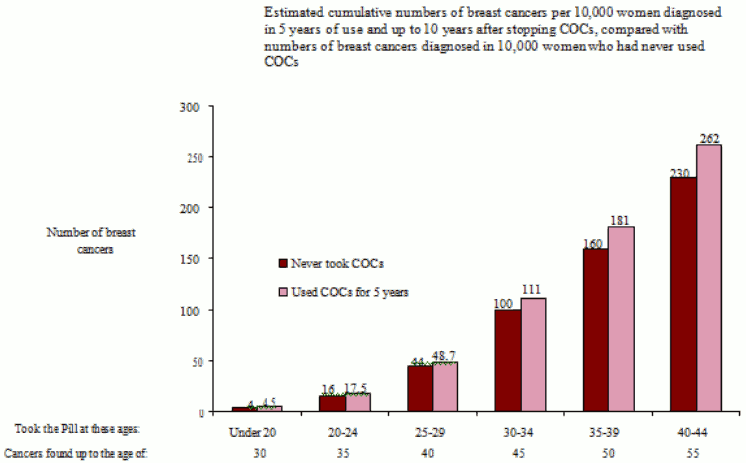
A meta-analysis from 54 epidemiological studies reported that there is a slightly increased relative risk (RR = 1.24) of having breast cancer diagnosed in women who are currently using combined oral contraceptives (COCs). The observed pattern of increased risk may be due to an earlier diagnosis of breast cancer in COC users, the biological effects of COCs or a combination of both. The additional breast cancers diagnosed in current users of COCs or in women who have used COCs in the last ten years are more likely to be localised to the breast than those in women who never used COCs.
Breast cancer is rare among women under 40 years of age whether or not they take COCs. Whilst this background risk increases with age, the excess number of breast cancer diagnoses in current and recent COC users is small in relation to the overall risk of breast cancer (see bar chart).
The most important risk factor for breast cancer in COC users is the age women discontinue the COC; the older the age at stopping, the more breast cancers are diagnosed. Duration of use is less important and the excess risk gradually disappears during the course of the 10 years after stopping COC use such that by 10 years there appears to be no excess.
The possible increase in risk of breast cancer should be discussed with the user and weighed against the benefits of COCs taking into account the evidence that they offer substantial protection against the risk of developing certain other cancers (e.g. ovarian and endometrial cancer).
In rare cases, benign liver tumours, and even more rarely, malignant liver tumours have been reported in users of CHCs. In isolated cases, these tumours have led to life-threatening intra-abdominal haemorrhages. A hepatic tumour should be considered in the differential diagnosis when upper abdominal pain, enlarged liver or signs of intra-abdominal haemorrhage occur in women taking CHCs.
3. ALT elevations
During clinical trials with patients treated for hepatitis C virus infections (HCV) with medicinal products containing ombitasvir/paritaprevir/ritonavir and dasabuvir, with or without ribavirin, transaminase (ALT) elevations higher than 5 times the upper limit of normal (ULN) occurred significantly more frequently in women using ethinylestradiol-containing medications such as combined hormonal contraceptives (CHCs) (see sections 4.3 and 4.5).
4. Other conditions
Women with hypertriglyceridemia, or a family history thereof, may be at an increased risk of pancreatitis when using CHCs.
Although small increases in blood pressure have been reported in many women taking CHCs, clinically relevant increases are rare. A relationship between CHC use and clinical hypertension has not been established. However, if a sustained clinically significant hypertension develops during the use of a CHC then it is prudent for the physician to withdraw the CHC and treat the hypertension. Where considered appropriate, CHC use may be resumed if normotensive values can be achieved with antihypertensive therapy.
The following conditions have been reported to occur or deteriorate with both pregnancy and CHC use, but the evidence of an association with CHC use is inconclusive: jaundice and/or pruritus related to cholestasis; gallstone formation; porphyria; systemic lupus erythematosus; haemolytic uraemic syndrome: Sydenham's chorea; herpes gestationis; otosclerosis-related hearing loss; hereditary angioedema.
Acute or chronic disturbances of liver function may necessitate the discontinuation of CHC use until markers of liver function return to normal. Recurrence of cholestatic jaundice which occurred previously during pregnancy or use of sex steroids necessitates the discontinuation of CHCs.
Although CHCs may have an effect on peripheral insulin resistance and glucose tolerance, there is no evidence for a need to alter the therapeutic regimen in diabetics using CHCs. However, diabetic women should be carefully observed while taking CHCs.
Crohn's disease and ulcerative colitis have been associated with CHC use.
Chloasma may occasionally occur, especially in women with a history of chloasma gravidarum. Women with a tendency to chloasma should avoid exposure to the sun or ultraviolet radiation whilst taking this preparation.
Marvelon contains <80 mg lactose per tablet. Patients with rare hereditary problems of galactose intolerance, the Lapp lactase deficiency or glucose-galactose malabsorption should not take medicine.
Relative Contraindications
Severe depression or a history of this condition. Depressed mood and depression are well-known undesirable effects of hormonal contraceptive use (see section 4.8). Depression can be serious and is a well-known risk factor for suicidal behaviour and suicide. Women should be advised to contact their physician in case of mood changes and depressive symptoms, including shortly after initiating the treatment.
4.4.2 Medical Examination/consultation
Prior to the initiation or reinstitution of Marvelon a complete medical history (including family history) should be taken and pregnancy must be ruled out. Blood pressure should be measured and a physical examination should be performed, guided by the contraindications (see section 4.3) and warnings (see section 4.4). It is important to draw a woman's attention to the information on venous and arterial thrombosis, including the risk of Marvelon compared with other CHCs, the symptoms of VTE and ATE, the known risk factors and what to do in the event of a suspected thrombosis.
The woman should also be instructed to carefully read the user leaflet and to adhere to the advice given. The frequency and nature of examinations should be based on established practice guidelines and be adapted to the individual woman.
Women should be advised that hormonal contraceptives do not protect against HIV infections (AIDS) and other sexually transmitted diseases. If there is risk of STI/HIV (including during pregnancy or postpartum), the correct and consistent use of condoms is recommended, either alone or with another contraceptive method.
4.4.3 Reduced Efficacy
The efficacy of Marvelon may be reduced in the event of missed tablets (Section 4.2.3), gastrointestinal disturbances (Section 4.2.4) or concomitant medications that decrease the plasma concentration of etonogestrel, the active metabolite of desogestrel (Section 4.5.1).
4.4.4 Reduced Cycle Control/ irregular bleeding
With all CHCs, irregular bleeding (spotting or breakthrough bleeding) may occur, especially during the first months of use. Therefore, the evaluation of any irregular bleeding is only meaningful after an adaptation interval of about three cycles.
If bleeding irregularities persist or occur after previously regular cycles, then non-hormonal causes should be considered and adequate diagnostic measures are indicated to exclude malignancy or pregnancy. These may include curettage.
In some women withdrawal bleeding may not occur during the tablet-free interval. If the CHC has been taken according to the directions described in Section 4.2, it is unlikely that the woman is pregnant. However, if the CHC has not been taken according to these directions prior to the first missed withdrawal bleed or if two withdrawal bleeds are missed, pregnancy must be ruled out before CHC use is continued.
1 These incidences were estimated from the totality of the epidemiological study data, using relative risks for the different products compared with levonorgestrel-containing CHCs.
2 Mid-point of range of 5-7 per 10,000 WY, based on a relative risk for CHCs containing levonorgestrel versus non-use of approximately 2.3 to 3.6
4.5. Interaction with other medicinal products and other forms of interaction
4.5.1 Interactions
Interactions between oral contraceptives and other medicinal products may lead to breakthrough bleeding and/or contraceptive failure. The following interactions have been reported in the literature:
Hepatic metabolism:
Interactions can occur with medicinal or herbal products that induce microsomal enzymes, specifically cytochrome P450 enzymes (CYP), which can result in increased clearance reducing plasma concentrations of sex hormones and may decrease the effectiveness of combined oral contraceptives, including Marvelon. These products include phenytoin, phenobarbital, primidone, bosentan, carbamazepine, rifampicin, rifabutin and possibly also oxcarbazepine, modafinil, topiramate, felbamate, griseofulvin, some HIV protease inhibitors (e.g., ritonavir) and non-nucleoside reverse transcriptase inhibitors (e.g., efavirenz) and products containing the herbal remedy St. John's wort.
Enzyme induction can occur after a few days of treatment. Maximal enzyme induction is generally observed within a few weeks. After drug therapy is discontinued, enzyme induction can last for about 28 days.
Women receiving any of the above mentioned hepatic enzyme-inducing medicinal or herbal products should be advised that the efficacy of Marvelon may be reduced. A barrier contraceptive method should be used in addition to Marvelon during administration of the hepatic enzyme-inducing medicinal product, and for 28 days after discontinuation of the hepatic enzyme-inducing medicinal product. If concomitant drug administration runs beyond the end of the tablets in the current COC pack, the next COC pack should be started right away without the usual tablet-free interval.
For women on long-term therapy with enzyme-inducing medicinal products, an alternative method of contraception unaffected by enzyme-inducing medicinal products should be considered.
- When co-administered with hormonal contraceptives, many combinations of HIV protease inhibitors (e.g., nelfinavir) and non-nucleoside reverse transcriptase inhibitors (e.g., nevirapine), and/or combinations with Hepatitis C virus (HCV) medicinal products (e.g., boceprevir, telaprevir), can increase or decrease plasma concentrations of progestins, including etonogestrel, the active metabolite of desogestrel, or estrogens. The net effect of these changes may be clinically relevant in some cases.
- Concomitant administration of strong (e.g., ketoconazole, itraconazole, clarithromycin) or moderate (e.g., fluconazole, diltiazem, erythromycin) CYP3A4 inhibitors may increase the serum concentrations of estrogens or progestins, including etonogestrel, the active metabolite of desogestrel.
- Oral contraceptives may interfere with the metabolism of other drugs. Accordingly, plasma and tissue concentrations may be increased (e.g., ciclosporin) or decreased (e.g., lamotrigine).
Note: The prescribing information of concomitant medications should be consulted to identify potential interactions.
Pharmacodynamic interactions
Concomitant use with medicinal products containing ombitasvir/paritaprevir/ritonavir and dasabuvir, with or without ribavirin may increase the risk of ALT elevations (see sections 4.3 and 4.4). Therefore, Marvelon users must switch to an alternative method of contraception (e.g., progestagen-only contraception or non-hormonal methods) prior to starting therapy with this combination drug regimen. Marvelon can be restarted 2 weeks following completion of treatment with this combination drug regimen.
4.5.2 Laboratory Tests
The use of contraceptive steroids may influence the results of certain laboratory tests, including biochemical parameters of liver, thyroid, adrenal and renal function, plasma levels of (carrier) proteins, e.g. corticosteroid binding globulin and lipid/lipoprotein fractions, parameters of carbohydrate metabolism and parameters of coagulation and fibrinolysis. Changes generally remain within the normal laboratory range.
4.6. Pregnancy and lactation
Marvelon is not indicated for use during pregnancy. If pregnancy occurs during treatment with Marvelon, further intake should be stopped.
However, most epidemiological studies have revealed neither an increased risk of birth defects in children born to women who used CHCs prior to pregnancy, nor a teratogenic effect when CHCs were taken inadvertently during early pregnancy.
The increased risk of VTE during the postpartum period should be considered when re-starting Marvelon (see sections 4.2 and 4.4).
Lactation may be influenced by CHCs as they may reduce the quantity and change the composition of breast milk. Therefore, the use of CHCs should generally not be recommended until the nursing mother has completely weaned her child. Small amounts of the contraceptive steroids and/or their metabolites may be excreted with the milk but there is no evidence that this adversely affects infant health.
4.7. Effects on ability to drive and use machines
No effects on ability to drive and use machines have been observed.
4.8. Undesirable effects
Description of selected adverse reactions
As with all COCs, changes in vaginal bleeding patterns may occur, especially during the first months of use. These may include changes in bleeding frequency (absent, less, more frequent or continuous), intensity (reduced or increased) or duration.
An increased risk of arterial and venous thrombotic and thromboembolic events, including myocardial infarction, stroke, transient ischaemic attacks, venous thrombosis and pulmonary embolism has been observed in women using CHCs, which are discussed in more detail in section 4.4.
Possibly related undesirable effects that have been reported in users of Marvelon or CHC users in general are listed in the table below1. All ADRs are listed by system organ class and frequency; common (≥1/100), uncommon (≥1/1,000 to <1/100) and rare (<1/1,000).
| System Organ Class | Common | Uncommon | Rare |
|---|---|---|---|
| Immune system disorders | Hypersensitivity | ||
| Metabolism and nutrition disorders | Fluid retention | ||
| Psychiatric disorders | Depressed mood, mood altered | Libido decreased | Libido increased |
| Nervous system disorders | Headache | Migraine | |
| Eye disorders | Contact lens intolerance | ||
| Vascular disorders | Venous thromboembolism2 Arterial thromboembolism2 | ||
| Gastrointestinal disorders | Nausea, abdominal pain | Vomiting, diarrhoea | |
| Skin and subcutaneous tissue disorders | Rash, urticaria | Erythema nodosum, erythema multiforme | |
| Reproductive system and breast disorders | Breast pain, breast tenderness | Breast enlargement | Vaginal discharge, breast discharge |
| Investigations | Weight increased | Weight decreased |
1 The most appropriate MedDRA term (version 11) to describe a certain adverse reaction is listed. Synonyms or related conditions are not listed, but should be taken into account as well.
2 Incidence in observational cohort studies of ≥1/10000 to 1/1000 women-years.
Reporting of suspected adverse reactions
Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via the Yellow Card Scheme, at: www.mhra.gov.uk/yellowcard or search for MHRA Yellow Card in the Google Play or Apple App Store.
6.2. Incompatibilities
Not applicable.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.