MYCOKEM 500 Film-coated tablet Ref.[50464] Active ingredients: Mycophenolate mofetil
Source: Pharmaceutical Benefits Scheme (AU) Revision Year: 2021 Publisher: Pharmacor Pty Ltd., Suite 803, Level 8, Tower A, The Zenith, 821 Pacific Highway, Chatswood, NSW 2067, Australia www.pharmacor.com.au Website: www.pharmacor.com.au Phone: 1300 138 805
4.3. Contraindications
Allergic reactions to mycophenolate mofetil tablets have been observed; therefore, mycophenolate mofetil tablets are contraindicated in patients with hypersensitivity to mycophenolate mofetil or to mycophenolic acid.
Mycophenolate mofetil is contraindicated during pregnancy due to its mutagenic and teratogenic potential (see Section 4.6 Fertility, pregnancy and lactation).
Mycophenolate mofetil is contraindicated in women of childbearing potential not using highly effective contraceptive methods (see Section 4.6 Fertility, pregnancy and lactation).
Mycophenolate mofetil is contraindicated in women who are breastfeeding (see Section 4.6 Fertility, pregnancy and lactation).
4.4. Special warnings and precautions for use
General
Female patients of childbearing potential must use effective contraception before, during and for six weeks after receiving mycophenolate tablets.
Mycophenolate mofetil is contraindicated during pregnancy and during breastfeeding (see Section 4.6 Fertility, pregnancy and lactation).
Men should not donate semen during therapy and for 90 days following discontinuation of mycophenolate mofetil.
Neoplasms
As with other patients receiving immunosuppressive regimes involving combinations of medicines, patients receiving Mycokem 500 as part of an immunosuppressive regimen are at an increased risk of developing lymphomas and other malignancies, particularly of the skin. The risk appears to be related to the intensity and duration of immunosuppression rather than the use of any specific agent. Approximately 1% of patients receiving mycophenolate mofetil with other immunosuppressive agents in the controlled studies of prevention of rejection have developed lymphoproliferative disease or lymphoma. As immunosuppression increases the risk of skin cancer, patients should also be advised to limit their exposure to sunlight and other sources of UV light by wearing protective clothing and using sunscreen with a high protection factor.
Infections
Oversuppression of the immune system can also increase susceptibility to infection, including opportunistic infections, fatal infections and sepsis. In the controlled studies for the prevention of rejection, the incidence of fatal infection was similar in patients receiving mycophenolate mofetil or control therapy in combination with other immunosuppresive agents. There was a higher incidence of fatal infection in the liver transplant study (5%) compared with the other studies (2%).
Such infections include latent viral reactivation, such as hepatitis B or hepatitis C reactivation or infections by polyomaviruses. Cases of hepatitis due to reactivation of hepatits B or hepatitis C have been reported in carrier patients treated with immunosuprresants. Casses of Progressive Multifocal Leukoencephalopathy (PML), associated with the JC virus, sometimes fatal, have been reported in mycophenolate mofetil-treated patients. Hemiparesis, apathy, confusion, cognitive deficiencies and ataxia were the most frequent clinical features observed. The reported cases generally had risk factors for PML, including concomitant immunosuppressant therapies and impaired immune function. In immunosuppressed patients, physicians should consider PML in the differential diagnosis in patients reporting neurological symptoms and consultation with a Neurologist should be considered as clinically indicated. Consideration should be given to reducing the amount of immunosuppression in patients who develop PML.
In transplant patients, physicians should also consider the risk that reduced immunosuppression represents to the graft.
BK virus- associated neuropathy has been observed during the use of mycophenolate mofetil in patients post-renal transplant.This infection can be associated with serious outcomes, sometimes leading to renal graft loss. Patient monitoring may help detect patients at risk of BK Virus-associated nephropathy. Reduction in immunosuppression should be considered for patients who develop evidence of BK virus-associated nephropathy
Blood and Immune System
Cases of pure red cell aplasia (PRCA) have been reported in patients treated with mycophenolate mofetil in combination with other immunosuppressive agents. The mechanism for mycophenolate mofetil-induced PRCA is unknown; the relative contribution of other immunosuppressants and their combinations in an immunosuppression regimen are also unknown. In some cases, PRCA was found to be reversible with dose reduction or cessation of mycophenolate mofetil therapy. In transplant patients however, reduced immunosuppression may place with graft at risk.
Patients receiving Mycokem 500 should be instructed to immediately report any evidence of infection, unexpected bruising, bleeding or any other manifestation of bone marrow depression.
Patients on mycophenolate mofetil should have complete blood counts weekly during the first month of treatment, twice monthly for the second and third months, then monthly through the first year. In particular, patients receiving mycophenolate mofetil should be monitored for neutropenia. The development of neutropenia may be related to mycophenolate mofetil, concomitant medications, viral infection or some combination of these causes. If neutropenia develops (absolute neutrophil count <1.3 x 103/μL), dosing with mycophenolate mofetil should be interrupted or the dose reduced and the patient should be carefully observed.
0.5% of patients receiving mycophenolate mofetil 2 g for prevention of rejection in renal transplantation, 2.8% of patients receiving mycophenolate mofetil 3 g in cardiac transplantation and 3.6% of patients receiving mycophenolate mofetil 3 g in hepatic transplantation, developed severe neutropenia (absolute neutrophil count [ANC] <5 x 108/L).
Patients should be advised that during treatment with mycophenolate mofetil vaccinations may be less effective and the use of live attenuated vaccines should be avoided (see Section 4.5 Interactions with Other Medicines and other forms of interactions). Influenza vaccination may be of value. Physicians should refer to the national guidelines for influenza vaccination.
Patients should not donate blood during therapy and for at least 6 weeks following discontinuation of mycophenolate mofetil.
Gastrointestinal
Mycophenolate mofetil has been associated with an increased incidence of digestive system adverse events, including uncommon cases of gastrointestinal tract ulceration, haemorrhage, and perforation (colon, gall bladder) in post-marketing surveillance, mycophenolate mofetil should be administered with caution in patients with active serious digestive system disease. Gastrointestinal tract bleeding (requiring hospitalisation) has been observed in approximately 1.4% of patients treated with mycophenolate mofetil 2 g in renal transplantation, 2.8% of patients receiving 3 g in cardiac transplantation and in 5.4% of patients receiving mycophenolate mofetil 3 g in hepatic transplantation. Gastrointestinal tract perforations have rarely been observed. Most patients were also receiving other drugs that are associated with these complications (see Section 4.8 Adverse effects (Undesirable effects)). It should be noted that patients with active peptic ulcer disease were excluded from enrolment in studies with mycophenolate mofetil.
Since mycophenolate mofetil is an IMPDH (inosine monophosphate dehydrogenase) inhibitor, on theoretical grounds it should be avoided in patients with rare hereditary deficiency of hypoxanthine guanine phosphoribosyl transferase (HGPRT) such as Lesch-Nyhan and Kelley-Seegmiller syndrome.
Interactions
Caution should be exercised when switching combination therapy from regimens containing immunosuppressants which interfere with MPA enterohepatic recirculation e.g. ciclosporin, to others devoid of this effect e.g. tacrolimus, sirolimus, belatacept, or vice versa, as this might result in changes of MPA exposure. Drugs which interfere with MPA's enterohepatic cycle e.g. cholestyramine, antibiotics should be used with caution due to their potential to reduce the plasma levels and efficacy of mycophenolate mofetil (see section 4.5 Interactions with other medicines and other forms of interactions).
Therapeutic drug monitoring of MPA may be appropriate when switching combination therapy (e.g. from ciclosporin to tacrolimus or vice versa) or to ensure adequate immunosuppression in patients with high immunological risk (e.g. risk of rejection, treatment with antibiotics, addition or removal of an interacting medication).
Azathioprine: It is recommended that mycophenolate mofetil should not be administered concomitantly with azathioprine because both have the potential to cause bone marrow suppression and such concomitant administration has not been studied.
Phenylketonurics
Mycophenolate mofetil oral suspension contains aspartame, a source of phenylalanine (0.56mg phenylalanine per mL suspension). Therefore care should be taken if mycophenolate mofetil oral suspension is administered to patients with phenylketonuria.
Use in renal impairment
Patients with severe chronic renal impairment (GFR <25 mL/minute/1.73m²) who have received single doses of mycophenolate mofetil showed increased plasma AUCs of mycophenolic acid and glucuronide of mycophenolic acid relative to patients with lesser degrees of renal impairment or normal healthy patients. Patients with severe chronic renal impairment should be carefully monitored and administration of doses of mycophenolate mofetil greater than 1g bd should be avoided (see Sections 4.2 Dose and method of administration and 5.2 Pharmacokinetic properties).
In patients with delayed graft function post-transplant, mean mycophenolic acid AUC(0-12) was comparable, but MPAG AUC(0-12) was two to three fold higher, compared to that seen in post-transplant patients without delayed graft function. In the three controlled studies of prevention of rejection, there were 298 of 1 483 patients (20%) with delayed graft function. Although patients with delayed graft function have a higher incidence of certain adverse events (anaemia, thrombocytopenia, hyperkalaemia) than patients without delayed graft function, these events were not more frequent in patients receiving mycophenolate mofetil than azathioprine or placebo. No dose adjustment is recommended for these patients; however, they should be carefully observed.
In renal transplant patients with severe chronic renal impairment, administration of doses greater than 1 g twice daily should be avoided.
Use in the elderly
Elderly patients may be at an increased risk of certain infections (including CMV tissue invasive disease) and possibly gastrointestinal haemorrhage and pulmonary oedema, compared with younger individuals. Elderly patients (over 65 years) may generally be at increased risk of adverse reactions due to immunosuppression. Pharmacokinetic behaviour of mycophenolate mofetil in the elderly has not been formally evaluated.
Paediatric use
Based on a safety and pharmacokinetics study in renal paediatric patients, no significant differences in pharmacokinetic parameters in comparison to adult patients were observed. Paediatric patients experienced a higher incidence of certain adverse events (see Section 4.8 ADVERSE EFFECTS (UNDESIRABLE EFFECTS)). Data are insufficient to establish safety and efficacy in children below the age of two years.
Effects on laboratory tests
No data available.
4.5. Interaction with other medicinal products and other forms of interaction
Drug interaction studies with mycophenolate mofetil have been conducted with aciclovir, antacids, cholestyramine, ciclosporin A, ganciclovir, oral contraceptives, tacrolimus and trimethoprim/sulfamethoxazole. Drug interaction studies have not been conducted with other medicines that may be commonly administered to renal, cardiac or hepatic transplant patients.
Aciclovir
Following single dose administration of mycophenolate mofetil (1 g) and aciclovir (800 mg) to normal healthy subjects, higher glucuronide of mycophenolic acid (8.6%) and acyclovir (17.4%) plasma AUCs were observed when mycophenolate mofetil was administered with aciclovir in comparison to the administration of each drug alone. As mycophenolate mofetil plasma concentrations are increased in the presence of renal impairment, as are aciclovir concentrations, the potential exists for the mycophenolate and acyclovir or the prodrugs e.g. valaciclovir to compete for tubular secretion and thus further increases in concentrations of both drugs may occur.
Antacids with magnesium and aluminium hydroxides
Absorption of a single dose of mycophenolate mofetil (2 g) was decreased when aluminium/ magnesium hydroxide antacids were administered concomitantly to rheumatoid arthritis patients. The Cmax and 24 hour AUC values for mycophenolic acid were 33% and 17% lower, respectively than when mycophenolate mofetil was administered alone under fasting conditions.
Antibiotics
Antibiotics eliminating β-glucuronidase-producing bacteria in the intestine (e.g. aminoglycoside, cephalosporin, fluoroquinolone, and penicillin classes of antibiotics) may interfere with MPAG/MPA enterohepatic recirculation thus leading to reduced systemic MPA exposure. Information concerning the following antibiotics is available:
Ciprofloxacin and amoxicillin plus clavulanic acid
Reductions in pre-dose (trough) mycophenolic acid concentrations of 54% have been reported in renal transplant recipients in the days immediately following commencement of oral ciprofloxacin or amoxicillin plus clavulanic acid. Effects tended to diminish with continued antibiotic use and cease after discontinuation. The change in pre-dose level may not accurately represent changes in overall mycophenolic acid exposure, therefore, clinical relevance of these observations is unclear.
Norfloxacin /and Metronidazole
The combination of norfloxacin and metronidazole reduced the MPA AUC following a single dose of mycophenolate mofetil.
Trimethoprim /and Sulfamethoxazole
Following single dose administration of MMF (1.5 g) to healthy male volunteers pretreated for 10 days with trimethoprim 160 mg / and sulfamethoxazole 800 mg, no effect on the bioavailability of MPA was observed.
Cholestyramine
Following single dose administration of mycophenolate mofetil 1.5 g in normal healthy subjects pretreated with cholestyramine three times daily 4 g for four days, there was a mean 40% reduction in the AUC of mycophenolic acid (see Section 5.2 PHARMACOKINETICS PROPERTIES). In view of the significant reduction in the AUC of mycophenolic acid by cholestyramine, caution should be used with the concomitant use of Mycokem 500 and any drug which interferes with enterohepatic circulation because of the potential to reduce the efficacy of mycophenolate tablets.
Ciclosporin
Ciclosporin pharmacokinetics (at doses of 275 to 415 mg/day) were unaffected by single and multiple doses of mycophenolate mofetil 1.0 g bd in stable renal transplant patients. The mean (±SD) dose normalised AUC(0-12 hours) of mycophenolic acid after 14 days and 3 months of multiple doses of mycophenolate mofetil and cyclosporin in 17 renal transplant patients were 43 ± 11 and 56 ± 31μg, hour.mL, respectively. However, ciclosporin interferes with MPA enterohepatic recycling, resulting in reduced MPA exposures by 30-50% in renal transplant patients treated with mycophenolate mofetil and ciclosporin compared with patients receiving sirolimus or belatacept and similar doses of mycophenolate mofetil. Conversely, changes of MPA exposure should be expected when switching patients from ciclosporin to one of the immunosuppressants which do not interfere with MPA's enterohepatic cycle.
Drugs affecting glucuronidation
Concomitant administration of drugs inhibiting glucuronidation of MPA may increase MPA exposure (e.g., increase of MPA AUC0-∞ by 35% was observed with concomitant administration of isavuconazole). Caution is therefore recommended when administering these drugs concomitantly with mycophenolate mofetil.
Telmisartan
Concomitant administration of telmisartan and mycophenolate mofetil resulted in an approximately 30% decrease of mycophenolic acid (MPA) concentrations. Telmisartan changes MPA's elimination by enhancing PPAR gamma (peroxisome proliferator-activated receptor gamma) expression which in turn results in an enhanced UGT1A9 expression and activity.
Sirolimus
A study in 36 renal transplant patients demonstrated that concomitant administration of mycophenolate mofetil (1 g bd) and sirolimus resulted in the mean (± SD) AUC(0-12 hours) of mycophenolic acid after 14 days and 3 months were 81 ± 36 and 71 ± 26 μg. hour/mL respectively. Another study using 45 renal transplant patients demonstrated that a significant proportion of patients (10 of 30) who received the combination of sirolimus and mycophenolate mofetil were withdrawn with symptoms consistent with mycophenolic acid or sirolimus toxicity.
Monitoring of mycophenolic acid levels should be performed in renal graft recipients cotreated with sirolimus because of the risk of overexposure to this immunosuppressive agent.
Ganciclovir
Following single dose administration in stable renal transplant patients, no pharmacokinetic interaction was observed between mycophenolate mofetil (1.5 g) and intravenous ganciclovir (5 mg/kg). However, as glucuronide of mycophenolic acid (MPAG) plasma and ganciclovir concentrations are increased in the presence of renal impairment, the potential exists for the two medicines to compete for tubular secretion, and thus further increases in concentrations of both medicines may occur.
In patients with renal impairment in which mycophenolate mofetil and ganciclovir or its prodrugs (e.g. valganciclovir) are co administered, patients should be carefully monitored. However with mycophenolic acid no substantial alteration of MPA pharmacokinetics is anticipated and dose adjustment of mycophenolate mofetil is not required.
Iron
In a study involving 16 healthy volunteers, no clinically relevant interaction was found between mycophenolate mofetil and iron supplements when administered in a fasting state. In the same study, a 15% reduction in MPA AUC was observed when mycophenolate mofetil and iron were administered simultaneously with food. In an earlier study involving seven healthy volunteers, a significant reduction in MPA AUC was observed when mycophenolate mofetil and iron were administered in a fasting state. To avoid any possible interactions, iron supplements should be administered at least three hours following mycophenolate mofetil.
Live vaccines
Live vaccines should not be given to patients with an impaired immune response. The antibody response to other vaccines may be diminished.
Oral Contraceptives
The pharmacokinetics of oral contraceptives were unaffected by co administration of mycophenolate mofetil. A study of co-administration of mycophenolate mofetil (1 g bd) and combined oral contraceptives containing ethinyloestradiol (0.02-0.04 mg) and levonorgestrel (0.05-0.20 mg), desogestrel (0.15 mg) or gestodene (0.05-0.1 mg) conducted in 18 women with psoriasis over three menstrual cycles showed no clinically relevant influence of mycophenolate mofetil on serum levels of progesterone, LH and FSH, thus indicating no influence of mycophenolate mofetil on the ovulation-suppressing action of the oral contraceptives (see Section 4.6 Fertility, pregnancy and lactation, Use in Pregnancy).
Proton Pump Inhibitors (PPIs)
Decreased MPA exposure has been observed when PPIs, including lansoprazole and pantoprazole, were administered with mycophenolate mofetil. The clinical impact of reduced MPA exposure on organ rejection has not been established in transplant patients receiving PPIs and mycophenolate mofetil. Because clinical relevance has not been established, PPIs should be used with caution when co-administered to transplant patients being treated with mycophenolate mofetil.
Rifampicin
After correction for dose, a 70% decrease in mycophenolic acid exposure AUC(0-12hours) has been observed with concomitant rifampicin administration in a single heart lung transplant patient. It is, therefore recommended to monitor mycophenolic acid exposure levels and to adjust mycophenolate tablets doses accordingly to maintain clinical efficacy when the drugs are administered concomitantly.
Tacrolimus
The AUC and Cmax of mycophenolic acid, the active metabolite of mycophenolate mofetil, were not significantly affected by coadministration with tacrolimus, in stable hepatic transplant patients initiated on mycophenolate mofetil and tacrolimus. In contrast, there was an increase of approximately 20% in tacrolimus AUC when multiple doses of mycophenolate mofetil (1.5g bd) were administered to patients taking tacrolimus.
However, in renal transplant patients, tacrolimus concentration did not appear to be altered by mycophenolate mofetil.
Sevelamer and Other Calcium Free Phosphate Binders
Concomitant administration of sevelamer and mycophenolate mofetil in adults and paediatric patients decreased the Cmax and AUC(0-12) of mycophenolic acid by 30% and 25%, respectively. There are no data on mycophenolate mofetil with phosphate binders other than sevelamer. This data suggest that sevelamer and other calcium free phosphate binders should preferentially be given two hours after Mycophenolate tablets intake to minimise impact on the absorption of mycophenolic acid.
Other Interactions
The measured value for renal clearance of glucuronide of mycophenolic acid indicates removal occurs by renal tubular secretion as well as glomerular filtration. Consistent with this, co administration of probenecid, a known inhibitor of tubular secretion, with mycophenolate mofetil in monkeys raises the plasma AUC of glucuronide of mycophenolic acid by threefold. Thus, other medicines known to undergo renal tubular secretion may compete with glucuronide of mycophenolic acid and thereby raise plasma concentrations of glucuronide of mycophenolic acid or the other drug undergoing tubular secretion.
4.6. Fertility, pregnancy and lactation
Effects on fertility
MMF had no effect on fertility of male rats at oral doses up to 20 mg/kg/day or on female rats at oral doses up to 4.5mg/kg/day (0.8 and 0.1 times the expected maximum clinical dose based on AUC values respectively). A female fertility and reproduction study conducted in rats caused malformations (see Use in Pregnancy below). Malformations (including anophthalmia, agnathia, and hydrocephaly) occurred in the first generation offspring of female rats treated with oral doses of mycophenolate mofetil in the absence of maternal toxicity. No effect was seen on the fertility of male rats treated with mycophenolate mofetil.
Use in pregnancy.
Pregnancy Category D.
Mycophenolate mofetil is contraindicated during pregnancy and in women of childbearing potential not using highly effective contraceptive methods due to its mutagenic and teratogenic potential (see Section 4.3 Contraindications).
Mycophenolate mofetil is a human teratogen with an increased risk of spontaneous abortions (mainly in the first trimester) and congenital malformations in case of maternal exposure during pregnancy (see section 4.8 Adverse effects (Undesirable effects)). In the medical literature, the risk of spontaneous abortions have been reported as 45% to 49% following mycophenolate mofetil exposure, compared to a reported rate between 12% and 33% in solid organ transplant patients treated with other immunosuppressants.
Congenital malformations (including multiple malformations in individual newborns) have been reported in 23% to 27% of live births in mycophenolate mofetil exposed pregnancies in published literature. For comparison the risk of malformations is estimated at approximately 2% of live births in the overall population and at approximately 4% to 5 % in solid organ transplant patients treated with immunosuppressants other than mycophenolate mofetil.
Congenital malformations, including multiple malformations have been reported postmarketing in children of patients exposed to mycophenolate mofetil in combination with other immunosuppressants during pregnancy. The following malformations were most frequently reported:
- Facial malformations such as cleft lip, cleft palate, micrognathia and hypertelorism of the orbits;
- Abnormalities of the ear (e.g. abnormally formed or absent external/middle ear) and eye (e.g. coloboma, microphthalmos);
- Malformations of the fingers (e.g. polydactyly, syndactyly, brachydactyly);
- Cardiac abnormalities such as atrial and ventricular septal defects;
- Oesophageal malformations (e.g. oesophageal atresia);
- Nervous system malformations (such as spina bifida).
These findings were consistent with teratology studies performed in rats and rabbits where fetal resorptions and malformations occurred in absence of maternal toxicity.
Embryofoetal development studies were conducted with MMF in rats (0.6, 2, 6 mg/kg/day on gestation days 7-16, and 0.5, 1.5 and 4.5 mg/kg/day from prior to conception to weaning) and rabbits (10, 30, 90 mg/kg/day on gestation days 7-19). Foetal resorptions and malformations occurred in rats at doses of 4.5mg/kg/day or more (0.1 times the expected maximum human dose based on AUC values) and in rabbits at 90 mg/kg/day (0.1 times the expected maximum human dose based on AUC values), in the absence of maternal toxicity.
The observed malformations in rats or rabbits were highly predictive of human malformations. Animal malformations with reported human correlates can be broadly classified as facial defects (including cleft palate, agnathia), eye abnormalities (including anopthalmia, micropthalmia), cardiac malformations (including ectocardia), nervous system malformations (including hydrocephaly), abdominal and thoracic wall defects (including umbilical and diaphragmatic hernia), kidney and lung defects (including renal agenesis, ectopic kidney and lung hypoplasia), reproductive organ defects (cryptorchidism) and skeletal malformations. Additional animal malformations included spleen and adrenal gland defects (aplasia, dysplasia).
The no-effect levels for teratogenicity in rats and rabbits were 2 and 30 mg/kg/day, respectively. A peri and postnatal study in rats administered MMF 1, 3 or 10 mg/kg/day from gestation day 17 to weaning showed no adverse effects.
Before the start of treatment, female and male patients of reproductive potential must be made aware of the increased risk of pregnancy loss and congenital malformations and must be counseled regarding pregnancy prevention, and planning.
Use in lactation
It is not known whether the drug is excreted in human milk. Mycophenolate mofetil is contraindicated during breastfeeding due to the potential for serious adverse reactions in nursing infants (see Section 4.4 Contraindications).
Although the relevance to humans is unknown, studies in rats have shown MMF to be excreted in milk.
Pregnancy Testing
Prior to starting therapy with mycophenolate mofetil, female patients of childbearing potential must have two negative serum or urine pregnancy tests with a sensitivity of at least 25 mIU/mL; The second test should be performed 8-10 days after the first one and immediately before starting mycophenolate mofetil. Repeat pregnancy tests should be performed during routine follow-up visits. Results of all pregnancy tests should be discussed with the patient. Patients should be instructed to consult their physician immediately should they become pregnant.
Contraception
Females
Women of child bearing potential should use two reliable forms of contraception simultaneously, at least one of which must be highly effective, before beginning mycophenolate mofetil therapy, during therapy, and for six weeks following discontinuation of therapy, unless abstinence is the chosen method of contraception.
Males
Limited clinical evidence is currently available on paternal exposure to mycophenolate mofetil.
Non-clinical evidence shows that the dose of mycophenolate that could be transferred via the seminal fluid to a potentially pregnant partner is 30-fold lower than the concentration without teratogenic effects in rats, and 200-fold lower than the lowest teratogenic concentration in rats. Therefore, the risk of harm mediated via seminal fluid is considered negligible. However, genotoxic effects have been observed in animal studies at exposures exceeding the human therapeutic exposures by approximately 2.5-times. Thus, the risk of genotoxic effects on sperm cells cannot completely be excluded.
In absence of sufficient data to exclude a risk of harm to the fetus conceived during or directly after the treatment of the father, the following precautionary measure is recommended. Sexually active men are recommended to use condoms during treatment and for at least 90 days after cessation of treatment. Condom use applies for both reproductively competent and vasectomized men, because the risks associated with the transfer of seminal fluid also apply to men who have had a vasectomy. In addition, female partners of male patients are recommended to use highly effective contraception during treatment and for a total of 90 days after the last dose of mycophenolate mofetil.
4.7. Effects on ability to drive and use machines
Mycophenolate mofetil may have a moderate influence on the ability to drive and use machines.
Patients should be advised to use caution when driving or using machines if they experience adverse drug reactions such as somnolence, confusion, dizziness, tremor or hypotension during treatment with mycophenolate mofetil (see 4.8 Adverse Effects (Undesirable Effects)).
4.8. Undesirable effects
The adverse event profile associated with the use of immunosuppressive medicines is often difficult to establish owing to the presence of underlying disease and the concurrent use of many other medications. The principal adverse reactions associated with the administration of mycophenolate mofetil in combination with ciclosporin and steroids include diarrhoea, leucopenia, sepsis and vomiting, and there is evidence of a higher frequency of certain types of infections, such as tuberculosis and atypical mycobacterial infection. Uncommon but serious life- threatening infections such as meningitis and infectious endocarditis have been reported.
The incidence of adverse events for mycophenolate mofetil was determined in three randomised comparative double blind trials in prevention of rejection in renal transplant patients. However, due to the lower overall reporting of events in the placebo controlled prevention of rejection study, these data were not combined with the other two active controlled prevention trials, but are instead presented separately.
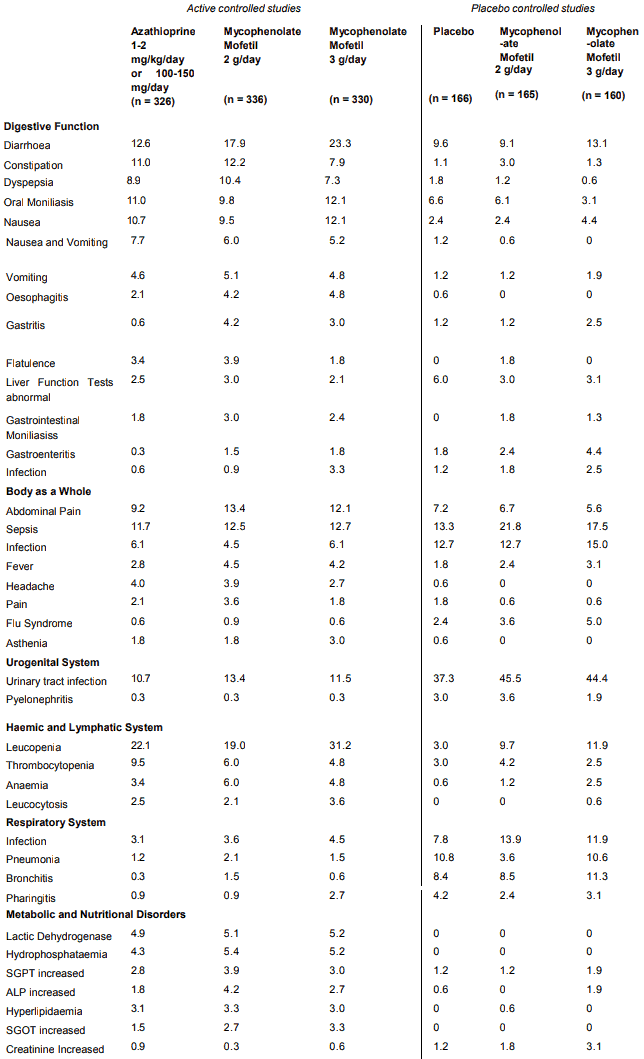
Patients in the double blind studies of the prevention of renal allograft rejection were treated for up to a minimum of one year, with approximately 53% of the patients having been treated for more than one year. The adverse events, reported as probably or possibly related to study medication at an incidence of greater than or equal to 3% of patients in either of the mycophenolate mofetil 2 or 3 g treatment groups, are presented in Table 1, for the two active controlled studies combined, and for the one placebo controlled study.
Table 1. Adverse Events in Prevention of Renal Allograft Rejection:
Patients in a double blind study of the prevention of cardiac allograft rejection were treated for up to a minimum of one year. The adverse events, reported as probably or possibly related to study medication at an incidence of greater than or equal to 3% of patients in either of the mycophenolate mofetil 3 g or azathioprine treatment groups are presented in Table 2.
Table 2. Adverse Events in Prevention of Cardiac Allograft Rejection with an Incidence of ≥3% in Either Treatment Arm:
| Active Controlled Cardiac Study | ||
|---|---|---|
| Mycophenolate mofetil 3 g/day (n=289) | Azathioprine 1.5-3.0 mg/kg/day (n=289) | |
| Digestive System | ||
| Nausea | 21.8 | 17.6 |
| Diarrhoea | 14.2 | 11.8 |
| Oral Moniliasis | 11.4 | 11.8 |
| Vomiting | 9.7 | 11.4 |
| Dyspepsia | 7.3 | 5.5 |
| Constipation | 5.5 | 6.6 |
| Flatulence | 3.1 | 5.5 |
| Gastritis | 5.2 | 2.8 |
| Nausea and Vomiting | 3.5 | 3.1 |
| Anorexia | 3.8 | 2.4 |
| Liver Damage | 3.1 | 3.1 |
| Liver Function Tests Abnormal | 3.1 | 2.1 |
| Haemic and Lymphatic System | ||
| Leucopenia | 26.0 | 36.3 |
| Anaemia | 6.2 | 7.6 |
| Thrombocytopenia | 3.5 | 6.6 |
| Body as a Whole | ||
| Sepsis | 9.7 | 10.0 |
| Headache | 7.3 | 9.0 |
| Abdominal Pain | 7.6 | 7.3 |
| Infection | 8.7 | 5.9 |
| Fever | 1.0 | 3.1 |
| Metabolic and Nutritional Disorders | ||
| Bilirubinaemia | 6.2 | 7.3 |
| SGPT Increased | 3.8 | 4.2 |
| SGOT Increased | 2.4 | 4.2 |
| Alkaline Phosphatase Increased | 2.4 | 3.8 |
| Lactic Dehydrogenase Increased | 2.8 | 3.5 |
| Respiratory System | ||
| Infection | 2.4 | 4.2 |
| Pneumonia | 1.7 | 3.1 |
| Nervous System | ||
| Insomnia | 3.1 | 2.1 |
| Urogenital System | ||
| Urinary tract infection | 4.2 | 4.5 |
Patients in a double blind study of the prevention of hepatic allograft rejection were treated for up to a minimum of one year. The adverse events, reported as probably or possibly related to study medication at an incidence of greater than or equal to 3% of patients in either of the mycophenolate mofetil 3 g or azathioprine treatment groups are presented in Table 3.
Table 3. Adverse Events in Prevention of Hepatic Allograft Rejection with an Incidence of ≥3% in Either Treatment Arm:
| Active Controlled Hepatic Study | ||
|---|---|---|
| Mycophenolate mofetil 3 g/day (n=277) | Azathioprine 1-2 mg/kg/day (n=287) | |
| Digestive System | ||
| Diarrhoea | 28.2 | 25.4 |
| Nausea | 26.7 | 19.9 |
| Vomiting | 11.9 | 12.2 |
| Oral Moniliasis | 9.4 | 9.8 |
| Hepatitis | 6.5 | 10.1 |
| Anorexia | 4.7 | 8.0 |
| Dyspepsia | 7.9 | 4.5 |
| Constipation | 5.4 | 4.5 |
| Flatulence | 5.4 | 3.1 |
| Liver Function Tests Abnormal | 4.0 | 3.1 |
| Gastointestinal moniliasis | 2.5 | 4.2 |
| Infection | 3.2 | 2.8 |
| Melaena | 3.2 | 2.8 |
| Haemic and Lymphatic System | ||
| Leucopenia | 42.2 | 35.2 |
| Anaemia | 12.6 | 19.9 |
| Thrombocytopenia | 14.4 | 16.0 |
| Hypochromic Anaemia | 6.1 | 4.2 |
| Leucocytosis | 4.3 | 4.9 |
| Body as a Whole | ||
| Sepsis | 18.8 | 20.2 |
| Abdominal Pain | 15.9 | 11.5 |
| Fever | 8.7 | 9.4 |
| Infection | 7.9 | 9.4 |
| Headache | 7.6 | 7.3 |
| Peritonitis | 3.2 | 4.9 |
| Abdomen Enlarged | 4.0 | 3.5 |
| Asthenia | 2.2 | 3.1 |
| Respiratory System | ||
| Infection | 4.0 | 6.6 |
| Respiratory Moniliasis | 4.3 | 5.6 |
| Pneumonia | 4.7 | 2.4 |
| Nervous System | ||
| Insomnia | 5.1 | 4.5 |
| Tremor | 3.6 | 2.1 |
| Urogenital System | ||
| Urinary tract infection | 7.6 | 9.4 |
| Cardiovascular System | ||
| Hypertension | 6.5 | 2.8 |
| Skin and Appendages | ||
| Herpes Simplex | 9.4 | 5.6 |
| Herpes Zoster | 4.0 | 4.9 |
The following adverse events, considered by the investigator to be possibly or probably related to drug treatment and not mentioned in any of the tables above, were reported with an incidence of less than 3% in one or more of the mycophenolate mofetil 2 g or 3 g (renal) active controlled cohorts (n=336, n=330), the mycophenolate mofetil 2 g or 3 g (renal) placebo-controlled cohorts (n=165, n=160), less than 1.4% in the mycophenolate mofetil 3 g (cardiac) active controlled cohort (n=289), or less than 1.4% in the mycophenolate mofetil 3 g (hepatic) active controlled cohort study (n=277).
Digestive System: colitis (sometimes caused by cytomegalovirus), ileus, duodenal ulcer, rectal disorder, stomach ulcer, duodenitis, gastrointestinal haemorrhage, mouth ulceration, dysphagia, peptic ulcer, cholecystitis, gastrointestinal disorder, ulcerative stomatitis, cheilitis, large intestine perforation, periodontal abscess, haemorrhagic gastritis, gum hyperplasia, stomatitis, eructation, haemorrhagic pancreatitis, intestinal necrosis, intestinal perforation, intestinal ulcer, gingivitis, glossitis, oesophageal ulcer, pancreatitis, aphthous stomatitis, enteritis, faecal impaction, stomach atony, haematemesis, duodenal ulcer haemorrhage, proctitis, rectal haemorrhage, gastrointestinal carcinoma, faecal incontinence, pancreas disorder, stomach ulcer haemorrhage, cholangitis, hepatic failure, perforated peptic ulcer, ulcerative colitis.
Body as a Whole: back pain, ciclosporin level increased, chest pain, reaction unevaluable, accidental injury, abscess, lab test abnormal, cyst, neoplasm, chills, face oedema, malaise, substernal chest pain, carcinoma, moniliasis, chills and fever, sarcoma, adenoma, granuloma, lack of drug effect, syncope, pelvis pain, pain, oedema, drug level increased, drug level decreased, injection site reaction, injection site inflammation, injection site hypersensitivity.
Urogenital System: dysuria, cystitis, haematuria, infection, oliguria, urinary frequency, pyuria, kidney abscess, abnormal kidney function, urethritis, urogenital carcinoma, kidney pain, nephritis, urethral pain, urinary urgency, urinary tract disorder, hydronephrosis, epididymitis, kidney tubular necrosis, urogenital occlusion, bladder neoplasm, urinary incontinence, vaginal moniliasis, kidney failure, urine abnormality.
Reproductive System: vaginal moniliasis, metrorrhagia, prostatic disorder, amenorrhoea, balanitis, cervix disorder, endometrial carcinoma, vaginal haemorrhage, impotence, breast pain, gynaecomastia, penis disorder.
Skin and Appendages: alopecia, fungal dermatitis, benign skin neoplasm, rash, acne, cutaneous moniliasis, pruritus, infection, urticaria, cellulitis, sweating, haemorrhage (skin and appendages), vesiculobullous rash, skin disorder, skin hypertrophy, skin ulcer, furunculosis, injection site inflammation, maculopapular rash, petechial rash, seborrhoea, skin carcinoma, skin discolouration.
Haemic and Lymphatic System: pancytopenia, polycythaemia, thrombocythaemia, agranulocytosis, lymphoma-like reaction, decreased immunoglobulins, ecchymosis, thrombotic thrombocytopenic purpura, epistaxis, haemorrhage, petechiae, abnormal WBC, blood dyscrasia, haemolytic anaemia, lymphadenopathy, hepatitis B serum antigen positive, reticuloendothelial hyperplasia, marrow hyperplasia, coagulation disorder, haemolysis.
Respiratory System: sinusitis, cough increased, dyspnoea, rhinitis, respiratory abscess, interstitial pneumonia, lung carcinoma, lung disorder, asthma, laryngismus, laryngitis, pneumothorax, hypoxia, atelectasis, lung oedema, lung fibrosis, pleural effusion, pleural disorder.
Metabolic and Nutritional Disorders: gamma-glutamyl transpeptidase increased, hypercholesterolaemia, hypokalaemia, acidosis, increased creatinine, bilirubinaemia, peripheral oedema, increased amylase, healing abnormal, hypocalcaemia, hyperglycaemia, albuminuria, weight loss, BUN increased, dehydration, decreased gamma-globulin, hypercalcaemia, hypervolaemia, hypoproteinaemia, uremia, hyperkalaemia, hyperchloraemia, enzymatic abnormality, hypomagnesaemia, increased creatine phosphokinase, hyperuricaemia, hyponatraemia, diabetes mellitus, gout, respiratory acidosis, oedema, hypoglycaemia, cachexia, hyperphosphataemia.
Liver and Biliary System: liver damage, cholestatic jaundice, cholelithiasis.
Cardiovascular System: pulmonary embolus, thrombosis, palpitation, angina pectoris, vasodilatation, arterial thrombosis, cerebrovascular accident, phlebitis, atrial fibrillation, supraventricular tachycardia, cyanosis, cerebral ischaemia, hypotension, peripheral gangrene, tachycardia, arrhythmia, heart arrest, occlusion, shock, gangrene, deep thrombophlebitis, myocardial infarct, cardiomegaly, ventricular extrasystoles, ventricular tachycardia, cerebral ischaemia, myocarditis, endocarditis, heart failure, pulmonary hypertension, cardiomyopathy, electrocardiogram abnormal, heart arrest, pericardial effusion.
Central and Peripheral Nervous System: hypertonia, dizziness, anxiety, vocal cord paralysis, neuropathy, paraesthesia, convulsion, depression, confusion, amnesia, depersonalisation, encephalitis, psychosis, agitation, hallucinations, aphasia, delirium, encephalopathy, hyperaesthesia, nystagmus, speech disorder, thinking abnormal, vertigo, apathy, catatonic reaction, CNS neoplasia, delusions, hemiplegia, hostility, hypokinesia, opisthotonos, paranoid reaction, personality disorder, somnolence, hypaesthesia, emotional lability, hyperkinesia, manic reaction.
Special Senses: otitis media, infection, conjunctivitis, eye haemorrhage, blepharitis, ear pain, visual disturbance, lacrimation disorder, corneal ulcer, deafness, diplopia, retinal disorder, taste loss, keratitis, retinitis, ear disorder, vestibular disorder, eye disorder, taste perversion, tinnitus, otitis externa, amblyopia, abnormal vision, eye pain, photophobia.
Musculo-Skeletal System: arthralgia, bone pain, leg cramps, myalgia, bone necrosis, joint disorder, myasthenia, myopathy, osteoporosis.
Endocrine: sialadenitis, hormone level altered hypothyroidism.
Up to 0.5% (regardless of investigator assessment of causality) of patients receiving mycophenolate mofetil 2 g for prevention of renal allograft rejection developed severe neutropenia (absolute neutrophil count (ANC) <5 x 108/L). Up to 2.8% (regardless of investigator assessment of causality) of cardiac transplant patients receiving mycophenolate mofetil 3 g and up to 3.6% (regardless of investigator assessment of causality) of patients receiving mycophenolate mofetil 3 g in hepatic transplantation developed severe neutropenia.
Cytomegalovirus (CMV) tissue invasive disease was more common in renal transplant patients receiving mycophenolate mofetil 3 g/day (8-12%) than in those receiving mycophenolate mofetil 2 g/day (4-8%) or control therapy (2-6%) in the three controlled studies for prevention of renal allograft rejection (percentage incidences have been determined regardless of investigator assessment of causality). In the placebo-controlled renal study, there was an increased incidence of herpes simplex and herpes zoster infections in patients receiving mycophenolate mofetil compared to placebo. In addition, the incidence of overall infection with Candida and CMV viraemia/syndrome were similar in the three treatment groups. Table 4 shows the incidence of select opportunistic infections in the prevention of rejection trials:
Table 4. Viral and Fungal Infections in Controlled Studies in Prevention of Renal, Cardiac or Hepatic Transplant Rejection:
| Renal Studies | Cardiac Study | Hepatic Study | |||||
|---|---|---|---|---|---|---|---|
| Mycophenolate mofetil | Mycophenolate mofetil | Azathioprine | Mycophenolate mofetil | Azathioprine | Mycophenolate mofetil | Azathioprine | |
| 2 g/day | 3 g/day | 1-2 mg•kg-1•day-1 or 100-150 mg/day | 3 g/day | 1.5-3 mg•kg-1•day-1 | 3 g/day | 1-2 mg•kg-1•day-1 | |
| (n=336) % | (n =330) % | (n=326) % | (n=289) % | (n=289) % | (n=277) % | (n=287) % | |
| Herpes simplex | 16.7 | 20.0 | 19.0 | 20.8 | 14.5 | 10.1 | 5.9 |
| CMV | |||||||
| Viraemia/syndrome | 13.4 | 12.4 | 13.8 | 12.1 | 10.0 | 14.1 | 12.2 |
| Tissue invasive disease | 8.3 | 11.5 | 6.1 | 11.4 | 8.7 | 5.8 | 8.0 |
| Herpes zoster | 6.0 | 7.6 | 5.8 | 10.7 | 5.9 | 4.3 | 4.9 |
| Cutaneous disease | 6.0 | 7.3 | 5.5 | 10.0 | 5.5 | 4.3 | 4.9 |
| Candida | 17.0 | 17.3 | 18.1 | 18.7 | 17.6 | 22.4 | 24.4 |
| Mucocutaneous | 15.5 | 16.4 | 15.3 | 18.0 | 17.3 | 18.4 | 17.4 |
The following other opportunistic infections occurred with an incidence of less than 4% in mycophenolate mofetil patients in the above azathioprine controlled studies: herpes zoster, visceral disease; Candida, urinary tract infection, fungemia/disseminated disease, tissue invasive disease; Cryptococcosis; Aspergillus/Mucor; Pneumocystis carinii.
In the placebo-controlled renal transplant study, the same pattern of opportunistic infection was observed compared to the azathioprine controlled renal study, with a notably lower incidence of herpes simplex and CMV tissue invasive disease.
In the three controlled studies for prevention of rejection in renal transplantation, similar rates of fatal infections/sepsis (<2%) have occurred in patients receiving mycophenolate mofetil or control therapy in combination with other immunosuppressive agents. In the controlled cardiac transplant study, fatal infections occurred in 2.4% of patients receiving mycophenolate mofetil 3 g compared to 4.5% of patients receiving azathioprine, both in combination with other immunosuppressive agents. In the controlled hepatic transplant study, fatal infection/sepsis occurred in 5.4% of patients receiving mycophenolate mofetil 3 g compared to 7.3% receiving azathioprine, both in combination with other immunosuppressive agents.
As with other patients receiving immunosuppressive regimes involving combinations of drugs, patients receiving mycophenolate mofetil as part of an immunosuppressive regimen are at an increased risk of developing lymphomas and other malignancies, particularly of the skin. Within three years post transplant, lymphoproliferative disease or lymphoma developed in patients receiving mycophenolate mofetil in immunosuppressive regimens in 0.6% of patients receiving 2 g daily in the controlled studies of prevention of renal rejection compared to placebo (0%) and azathioprine groups (0.6%).
The incidence of malignancies among the 1,483 patients enrolled in controlled trials for the prevention of renal allograft rejection was low, and similar to the incidence reported in the literature for renal allograft recipients. There was a slight increase in the incidence of lymphoproliferative disease in the mycophenolate mofetil treatment groups compared to the placebo and azathioprine groups. Table 5 summarises the incidence of malignancies observed in the prevention of rejection trials.
Table 5. Malignancies Observed in Prevention of Renal, Cardiac and Hepatic Rejection Trials No. of patients (%) with one or more malignancies (Regardless of Investigator Assessment of Causality):
| Renal Studies | Cardiac Study | Hepatic Study | ||||||
|---|---|---|---|---|---|---|---|---|
| Placebo | Azathioprine | Mycophenolate mofetil | Mycophenolate mofetil | Azathioprine | Mycophenolate mofetil | Azathioprine | Mycophenolate mofetil | |
| (n=166) | 1-2 mg/kg/day or 100-150mg/day (n=326) | 2 g/day (n=501) | 3 g/day (n=490) | 1.5-3 mg/kg/day (n=289) | 3 g/day (n=289) | 1-2 mg/kg/day (n=287) | 3 g/day (n=277) | |
| Lymphoma/lymphoproliferative disease | 0 | 0.3 | 0.6 | 1.0 | 2.1 | 0.7 | 0 | 0.4 |
| Nonmelanoma skin carcinoma | 0 | 2.4 | 4.0 | 1.6 | 2.8 | 4.2 | 2.1 | 2.2 |
| Other Malignancy | 1.8 | 1.8 | 0.8 | 1.4 | 2.1 | 2.1 | 2.4 | 0.7 |
Three year safety data in renal and cardiac transplant patients indicated that the overall incidence of malignancy was comparable between mycophenolate mofetil and azathioprine groups. Hepatic transplant patients were followed for at least one year but less than three years.
Paediatric Adverse Events
The type and frequency of adverse drug reactions in a clinical study of 100 paediatric patients 3 months to 18 years of age given mycophenolate mofetil 600 mg/m² orally twice daily were generally similar to those observed in adult patients given mycophenolate mofetil 1 g twice daily with the exception that paediatric patients had a higher proportion of diarrhoea, anaemia, sepsis and leucopenia.
Post-Marketing Experience
Infections: uncommon: serious life threatening infections such as meningitis and infectious endocarditis have been reported occasionally and there is evidence of a higher frequency of certain types of serious infections such as tuberculosis and atypical mycobacterial infections.
Cases of Progressive Multifocal Leukoencephalopathy (PML), sometimes fatal, have been reported in mycophenolate mofetil treated patients. The reported cases generally had risk factors for PML, including concomitant immunosuppressant therapies and impaired immune function. BK Virus –associated nephropathy has been observed in patients treated with mycophenolate mofetil.This infection can be associated with serious outcomes, sometimes leading to renal graft loss.
Neoplasm benign, malignant and unspecified (including cysts and polyps): Lymphoma, lymphoproliferative disorder.
Gastrointestinal: uncommon: pancreatitis, isolated cases of intestinal villous atrophy, colitis (sometimes caused by cytomegalovirus).
Congenital Disorders: congenital malformations have been reported post marketing in children of patients exposed to mycophenolate mofetil in combination with other immunosuppressants during pregnancy (see Section 4.6 Fertility, Pregnancy and Lactation).
Pregnancy, Puerperium and Perinatal Conditions: Cases of spontaneous abortions mainly in the first trimester in patients exposed to mycophenolate mofetil have been reported (see Section 4.6 Fertility, Pregnancy and Lactation).
Blood and Immune System: Cases of pure red cell aplasia (PRCA) have been reported in patients treated with mycophenolate mofetil in combination with other immunosuppressive agents, hypersensitivity.
Respiratory, thoracic and mediastinal disorders: Bronchiectasis, interstitial lung disease, pulmonary fibrosis.
Vascular disorders: Lymphocele.
General disorders and administration site conditions: De novo purine synthesis inhibitorsassociated acute inflammatory syndrome is a newly described paradoxical pro-inflammatory reaction associated with mycophenolate and other purine synthesis inhibitors, characterized by fever, arthralgias, arthritis, muscle pain and elevated inflammatory markers. Anecdotal literature reports showed rapid improvements following discontinuation of the drug.
Reporting suspected adverse effects
Reporting suspected adverse reactions after registration of the medicinal product is important. It allows continued monitoring of the benefit-risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions at www.tga.gov.au/reporting-problems.
6.2. Incompatibilities
Incompatibilities were either not assessed or not identified as part of the registration of this medicine.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.