MYRELEZ Solution for injection Ref.[50169] Active ingredients: Lanreotide
Source: Health Products Regulatory Authority (IE) Revision Year: 2021 Publisher: Amdipharm Limited, Temple Chambers, 3 Burlington Road, Dublin 4, Ireland
5.1. Pharmacodynamic properties
Pharmacotherapeutic group: Pituitary and hypothalamic hormones and analogues, somatostatin and analogues
ATC code: H01CB03
Lanreotide is an octapeptide analogue of natural somatostatin. Like somatostatin, lanreotide is an inhibitor of various endocrine, neuroendocrine, exocrine and paracrine functions. Lanreotide has a high affinity for human somatostatin receptors (SSTR) 2 and 5, and a reduced binding affinity for human SSTR 1, 3 and 4. Activity at human SSTR 2 and 5 is the primary mechanism considered to be responsible for GH inhibition. Lanreotide is more active than natural somatostatin and shows a longer duration of action.
Lanreotide, like somatostatin, exhibits a general exocrine anti-secretory action. It inhibits the basal secretion of motilin, gastric inhibitory peptide and pancreatic polypeptide, but has no significant effect on fasting secretin or gastrin secretion. Additionally, it decreases the levels of plasma chromogranin A and urinary 5-HIAA (5 Hydroxyindolacetic acid) in patients with GEP-NETs and elevated levels of these tumour markers. Lanreotide markedly inhibits meal-induced increases in superior mesenteric artery blood flow and portal venous blood flow. Lanreotide significantly reduces prostaglandin E1-stimulated jejunal secretion of water, sodium, potassium and chloride. Lanreotide reduces prolactin levels in patients with acromegaly patients treated long term.
In an open-label study, lanreotide 120mg was administered every 28 days for 48 weeks in 90 previously untreated acromegalic patients diagnosed with pituitary macroadenoma. Patients expected to require pituitary surgery or radiotherapy during the study period were excluded.
A reduction in tumour volume of ≥20% was observed in 63% of the patients (95% CI: 52%-73%). At week 48, the mean percentage reduction of tumour volume was 26.8%, GH levels were below 2.5 µg/L in 77.8% of the patients and IGF-1 levels normalised in 50%. Normalised IGF-1 levels combined with GH levels below 2.5 µg/L were observed in 43.5% of the patients.
Most patients reported a clear relief of acromegaly symptoms such as fatigue, excess perspiration, arthralgia and soft tissue swelling. Both early and sustained reduction of tumour volume as well as GH and IGF-1 levels were observed from week 12 onwards.
A phase III, 96-week, fixed duration, randomized, double-blind, multi-centre, placebo-controlled trial of lanreotide was conducted in patients with gastroenteropancreatic neuroendocrine tumours to assess the antiproliferative effect of lanreotide. Patients were randomized 1:1 to receive either lanreotide 120 mg every 28 days (n=101) or placebo (n=103). Randomization was stratified by previous therapy at entry and the presence/absence of progression at baseline as assessed by RECIST 1.0 (Response Evaluation Criteria in Solid Tumours) during a 3 to 6 month screening phase.
Patients had metastatic and/or locally advanced inoperable disease with histologically confirmed well or moderately well differentiated tumours primarily localized in the pancreas (44.6% patients), midgut (35.8%), hindgut (6.9%) or of other/unknown primary location (12.7%).
69% of patients with GEP-NETs had tumour grade 1 (G1), defined by either a proliferation index Ki67 ≤2% (50.5% of the overall patient population) or a mitotic index <2 mitosis/10 HPF (18.5% of the overall patient population) and 30% of patients with GEP-NETs had tumours in the lower range of grade 2 (G2) (defined by a Ki67 index >2% - ≤10%). Grade was not available in 1% of the patients. The study excluded patients with G2 GEP-NETs with a higher cellular proliferation index (Ki 67 >10% - ≤20%) and G3 GEP neuroendocrine carcinomas (Ki 67 index >20%). Overall, 52.5% of the patients had a hepatic tumour load ≤10%, 14.5% had a hepatic tumour load >10 and ≤25% and 33% had a hepatic tumour load >25%.
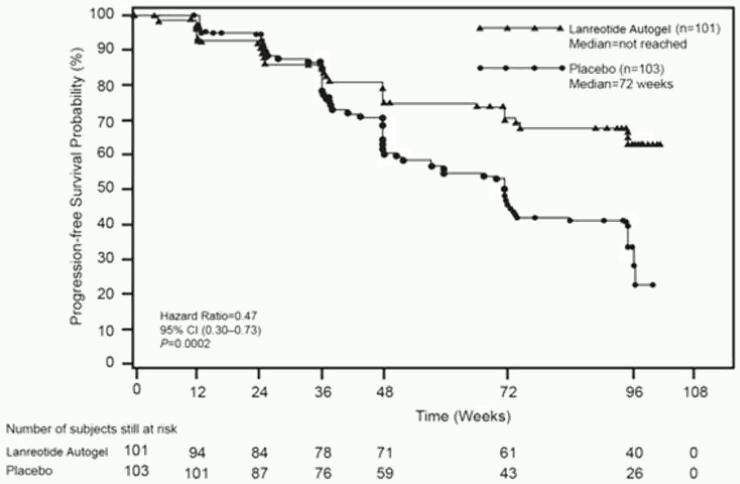
The primary endpoint was progression-free survival (PFS) measured as time to either disease progression by RECIST 1.0 or death within 96 weeks after first treatment administration. Analysis of PFS utilized independent centrally-reviewed radiological assessment of progression.
Table 1. Efficacy results of the phase III study:
| Median Progression free survival (weeks) | Hazard Ratio (95% CI) | Reduction in risk of progression or death | p-value | |
|---|---|---|---|---|
| lanreotide (n=101) | Placebo (n=103) | |||
| >96 weeks | 72.00 weeks (95% CI: 48.57, 96.00) | 0.470 (0.304, 0.729) | 53% | 0.0002 |
Figure 1. Kaplan-Meier Progression Free Survival Curves:
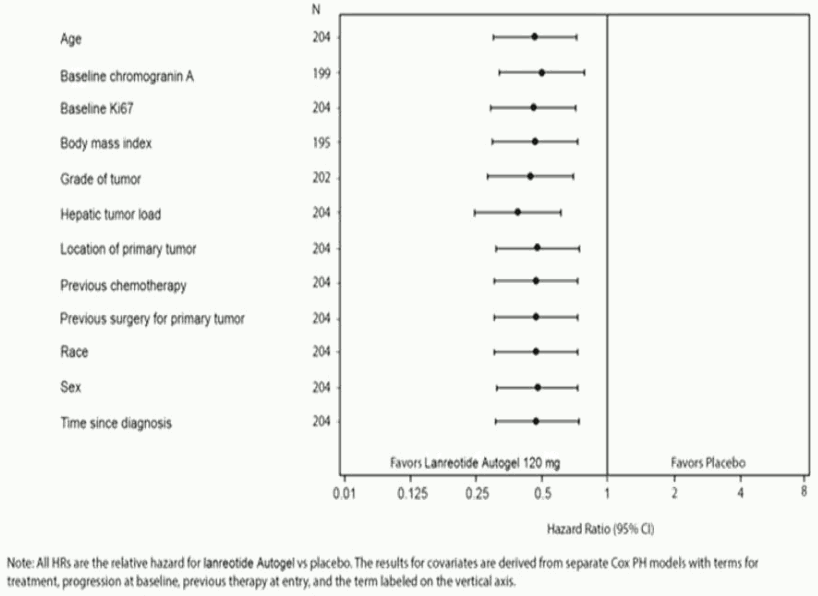
The beneficial effect of lanreotide in reducing the risk of progression or death was consistent regardless of the location of primary tumour, hepatic tumour load, previous chemotherapy, baseline Ki67, tumour grade or other pre-specified characteristics as shown in Figure 2.
A clinically-relevant benefit of treatment with lanreotide was seen in patients with tumours of pancreatic, midgut and other/unknown origin as in the overall study population. The limited number of patients with hindgut tumours (14/204) contributed to difficulty in interpreting the results in this subgroup. The available data suggested no benefit of lanreotide in these patients.
Figure 2. Results of the Cox Proportional Hazards Covariates Analysis of PFS:
Crossover from placebo to open-label lanreotide, in the extension study, occurred in 45.6% (47/103) of the patients.
Paediatric population
The European Medicines Agency has waived the obligation to submit the results of studies with the reference medicinal product containing lanreotide in all subsets of the paediatric population in acromegaly and pituitary gigantism (see section 4.2 for information on paediatric use). The European Medicines Agency has listed gastroenteropancreatic neuroendocrine tumours (excluding neuroblastoma, neuroganglioblastoma, phaechromocytoma) on the list of class waivers.
5.2. Pharmacokinetic properties
Intrinsic pharmacokinetic parameters of lanreotide after intravenous administration in healthy volunteers indicated limited extravascular distribution, with a steady-state volume of distribution of 16.1L. Total clearance was 23.7L/h, terminal half-life was 1.14 hours and mean residence time was 0.68 hours.
In studies evaluating excretion, less than 5% of lanreotide was excreted in urine and less than 0.5% was recovered unchanged in faeces indicating some biliary excretion.
After deep subcutaneous administration of lanreotide 60, 90 and 120 mg to healthy volunteers, lanreotide concentrations increase to achieve average maximum serum concentrations of 4.25, 8.39 and 6.79 ng/mL, respectively. These values of Cmax are achieved during the first day after the administration at 8, 12 and 7 hours (median values). From the peak serum levels of lanreotide, concentrations decrease slowly following first-order kinetics with a terminal elimination half-life of 23.3, 27.4 and 30.1 days respectively. 4 weeks after the administration mean lanreotide serum levels were 0.9, 1.11 and 1.69ng/mL respectively. Absolute bioavailability was 73.4, 69.0 and 78.4%, respectively.
After deep subcutaneous administration of lanreotide 60, 90 and 120 mg to patients with acromegaly, lanreotide concentrations increase to achieve average maximum serum concentrations of 1.6, 3.5 and 3.1ng/mL, respectively. These values of Cmax are achieved during the first day after the administration at 6, 6 and 24 hours. From the peak serum levels of lanreotide, concentrations decrease slowly following first-order kinetics and 4 weeks after the administration mean lanreotide serum levels were 0.7, 1.0 and 1.4 ng/mL, respectively.
Steady state serum levels of lanreotide were reached, on average, after 4 injections every 4 weeks. After repeated dose administration every 4 weeks the average values of Cmax at steady state were 3.8, 5.7 and 7.7ng/mL for 60, 90 and 120 mg respectively, the average Cmin values obtained being 1.8, 2.5 and 3.8ng/mL. The peak trough fluctuation index was moderate ranging from 81 to 108%.
Linear pharmacokinetic release profiles were observed after deep subcutaneous administration of lanreotide 60, 90 and 120 mg in patients with acromegaly.
Trough lanreotide serum levels obtained after three deep subcutaneous injections of lanreotide 60, 90 or 120 mg given every 28 days are similar to the steady-state trough lanreotide serum levels obtained in patients with acromegaly previously treated with intramuscular administrations of lanreotide 30 mg prolonged release microparticles every 14, 10 or 7 days, respectively.
In a population PK analysis in 290 GEP-NET patients receiving lanreotide 120 mg, rapid initial release was seen with mean Cmax values of 7.49 ± 7.58 ng/mL reached within the first day after a single injection. Steady-state concentrations were reached after 5 injections of lanreotide 120 mg every 28 days and were sustained up to the last assessment (up to 96 weeks after the first injection). At steady-state the mean Cmax values were 13.9 ± 7.44 ng/mL and the mean trough serum levels were 6.56 ± 1.99 ng/mL. The mean apparent terminal half-life was 49.8 ± 28.0 days.
Renal/Hepatic impairment
Subjects with severe renal impairment show an approximately 2-fold decrease in total serum clearance of lanreotide, with a consequent increase in half-life and AUC. In subjects with moderate to severe hepatic impairment, a reduction in clearance was observed (30%). Volume of distribution and mean residence time increased in subjects with all degrees of hepatic insufficiency.
No effect on clearance of lanreotide was observed in a population PK analysis of GEP-NET patients including 165 with mild and moderate renal impairment (106 and 59 respectively) treated with lanreotide. GEP-NET patients with severely impaired renal function were not studied.
No GEP-NET patients with hepatic impairment (as per Child-Pugh score) were studied. It is not necessary to alter the starting dose in patients with renal or hepatic impairment, as lanreotide serum concentrations in these populations are expected to be well within the range of serum concentrations safely tolerated in healthy subjects.
Elderly patients
Elderly subjects show an increase in half-life and mean residence time compared with healthy young subjects. It is not necessary to alter the starting dose in elderly patients, as lanreotide serum concentrations in this population are expected to be well within the range of serum concentrations safely tolerated in healthy subjects.
In a population PK analysis of GEP-NET patients including 122 aged 65 to 85 years, no effect of age on clearance and volume of distribution of lanreotide was observed.
5.3. Preclinical safety data
Effects in non-clinical studies were observed only at exposures considered sufficiently in excess of the maximum human exposure indicating little relevance to clinical use.
In carcinogenic bioassay studies conducted in rats and mice, no systemic neoplastic changes were observed at doses in excess of those achieved in humans at therapeutic doses. Increased incidence of subcutaneous tumours were observed at the injection sites likely due to the increased dose frequency in animals (daily) compared to monthly dosing in humans and therefore may not be clinically relevant.
In in vitro and in vivo standard battery tests, lanreotide did not show any genotoxic potential.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.