Source: FDA, National Drug Code (US) Revision Year: 2020
Neuraceq is indicated for Positron Emission Tomography (PET) imaging of the brain to estimate β-amyloid neuritic plaque density in adult patients with cognitive impairment who are being evaluated for Alzheimer’s Disease (AD) and other causes of cognitive decline.
A negative Neuraceq scan indicates sparse to no amyloid neuritic plaques and is inconsistent with a neuropathological diagnosis of AD at the time of image acquisition; a negative scan result reduces the likelihood that a patient’s cognitive impairment is due to AD. A positive Neuraceq scan indicates moderate to frequent amyloid neuritic plaques; neuropathological examination has shown this amount of amyloid neuritic plaque is present in patients with AD, but may also be present in patients with other types of neurologic conditions as well as older people with normal cognition. Neuraceq is an adjunct to other diagnostic evaluations.
Limitations of Use:
Neuraceq is a radioactive drug and should be handled with appropriate safety measures to minimize radiation exposure during administration [see Warnings and Precautions (5.2)]. Use waterproof gloves and effective shielding, including lead-glass syringe shields when handling and administering Neuraceq. Radiopharmaceuticals, including Neuraceq, should only be used by or under the control of physicians who are qualified by specific training and experience in the safe use and handling of radioactive materials, and whose experience and training have been approved by the appropriate governmental agency authorized to license the use of radiopharmaceuticals.
The recommended dose of Neuraceq is 300 MBq (8.1 mCi), maximum 30 mcg mass dose, administered as a single slow intravenous bolus (6 sec/mL) in a total volume of up to 10 mL. The dose may vary depending on the patient’s body weight, and image acquisition parameters [see Clinical Studies (14)].
Acquire PET images over 15 to 20 minutes starting 45 to 130 minutes after Neuraceq injection. Keep the patient supine with the head positioned to center the brain, including the cerebellum, in the PET scanner field of view. Reduce head movement with tape or other flexible head restraints if necessary. Reconstruction should include attenuation correction with resulting transaxial pixel sizes between 2 and 3 mm.
Neuraceq images should be interpreted only by readers who successfully complete Electronic Media- or In-Person Training provided by the manufacturer [see Warnings and Precautions (5.1)]. The objective of Neuraceq image interpretation is to estimate β-amyloid neuritic plaque density in brain gray matter, not to make a clinical diagnosis. Image interpretation is performed independently of a patient’s clinical features and relies upon the recognition of image features in certain brain regions.
PET images should be displayed in the transaxial orientation using gray scale or inverse gray scale. The sagittal and coronal planes may be used for additional orientation purposes. CT or MR images may be helpful for anatomic reference purposes. However, visual assessment should be performed using the axial planes according to the recommended reading methodology.
Interpretation of the images is made by visually comparing the activity in cortical gray matter with activity in adjacent white matter. Regions displayed in the PET images which ‘anatomically’ correspond to white matter structures (e.g., the cerebellar white matter or the splenium) should be identified to help the readers orient themselves. Images should be viewed and assessed in a systematic manner, starting with the cerebellum and scrolling up through the lateral temporal and frontal lobes, the posterior cingulate cortex/precuneus, and the parietal lobes. For a gray matter cortical region to be assessed as showing ‘tracer uptake’, the majority of slices from the respective region must be affected.
For each patient, the PET image assessment is categorized as either “β-amyloid-positive” or “β-amyloid-negative”. This determination is based on the assessment of tracer uptake in the gray matter of the following four brain regions: the temporal lobes, the frontal lobes, the posterior cingulate cortex/precuneus, and the parietal lobes; according to the following ‘rules for assessment’ [see Warnings and Precautions (5.1)]:
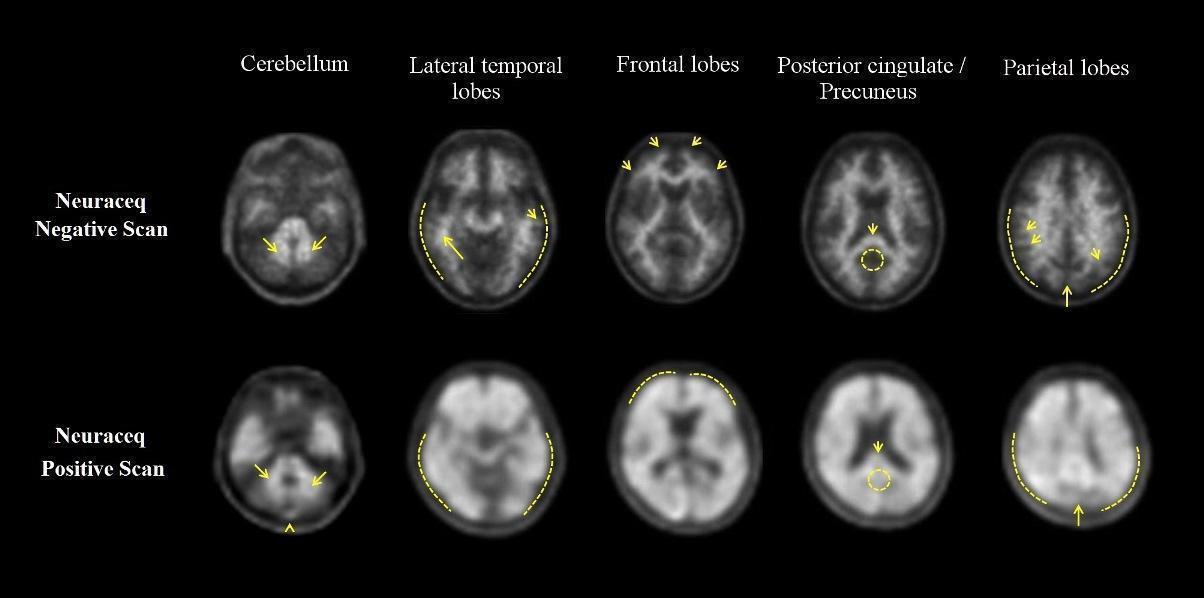
Examples of positive and negative scans for each of the four brain regions are illustrated in Figure 1.
Figure 1. Axial view of negative (top row) and positive (bottom row) Neuraceq PET scans:
Cerebellum: A contrast between the white matter (arrows) and gray matter is seen in both negative and positive scans. Extracerebral tracer uptake in scalp and in the posterior sagittal sinus (arrowhead) can be seen. Lateral temporal lobes: Spiculated or “mountainous” appearance of the white matter (arrows) is seen in the negative scan, and radioactive signal does not reach the outer rim of the brain (dashed line) due to lower tracer uptake in the gray matter. The positive scan shows a “plumped”, smooth appearance of the outer border of the brain parenchyma (dashed line) due to tracer uptake in the gray matter. Frontal Lobes: Spiculated appearance of the white matter in the frontal lobes (arrows) is seen in the negative scan. The positive scan shows the tracer uptake in these regions has a “plumped”, smooth appearance due to the increased gray matter signal (dashed line). Posterior cingulate/precuneus: Adjacent and posterior to the splenium (arrow), these regions appear as a hypo-intense “hole” (circle) in the negative scan, whereas this hole is “filled-up” (circle) in the positive scan. Parietal lobes: In the negative scan, the midline between the parietal lobes can be easily identified (long arrow); white matter has a spiculated appearance (short arrow) with low signal near the outer rim of the brain (dashed line). In the positive scan, the midline between the parietal lobes is much thinner. The cortical areas are “filled-up” and are smooth in appearance as tracer uptake extends to the outer rim of the brain.
Some scans may be difficult to interpret due to image noise, atrophy with a thinned cortex, or image blur. If a co-registered computerized tomography (CT) image is available, the CT image may be used to clarify the relationship of the Neuraceq uptake and the gray matter anatomy.
The estimated radiation absorbed doses for adults from intravenous injection of Neuraceq are shown in Table 1.
Table 1. Estimated Radiation Absorbed Doses from Intravenous Injection of Neuraceq:
| Organ/Tissue | Mean Absorbed Radiation Dose per Unit Administered Activity [mcGy/MBq] |
|---|---|
| Adrenals | 13 |
| Brain | 13 |
| Breasts | 7 |
| Gallbladder Wall | 137 |
| Heart Wall | 14 |
| Kidneys | 24 |
| Liver | 39 |
| Lower Large Intestine-Wall | 35 |
| Lungs | 15 |
| Muscle | 10 |
| Osteogenic Cells | 15 |
| Ovaries | 16 |
| Pancreas | 14 |
| Red Marrow | 12 |
| Skin | 7 |
| Small Intestine | 31 |
| Spleen | 10 |
| Stomach Wall | 12 |
| Testes | 9 |
| Thymus | 9 |
| Thyroid | 8 |
| Upper Large Intestine-Wall | 38 |
| Urinary Bladder Wall | 70 |
| Uterus | 16 |
| Total Body | 11 |
| Effective Dose (mcSv/MBq) | 19 |
The effective dose resulting from a 300 MBq (8.1 mCi) administration of Neuraceq in adult subjects is 5.8 mSv. The use of a CT scan to calculate attenuation correction for reconstruction of Neuraceq images (as done in PET/CT imaging) will add radiation exposure. Diagnostic head CT scans using helical scanners administer an average of 2.2 ± 1.3 mSv effective dose (CRCPD Publication E-07-2, 2007). The actual radiation dose is operator and scanner dependent. Thus, the total combined radiation exposure from Neuraceq administration and subsequent scan on a PET/CT scanner is estimated to be 8 mSv.
A pharmacological overdose of Neuraceq is unlikely given the relatively low doses used for diagnostic purposes.
In the event of administration of a radiation overdose with Neuraceq, the absorbed organ dose to the patient should be reduced by increasing elimination of the radionuclide from the body by inducing frequent micturition.
Store Neuraceq at room temperature 25°C (77°F); excursions permitted to 2°C to 42°C (36°F to 108°F).
The product does not contain a preservative. Store Neuraceq within the original container or equivalent radiation shielding. Neuraceq must not be diluted.
This preparation is approved for use by persons under license by the Nuclear Regulatory Commission or the relevant regulatory authority of an Agreement State.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.