NUZYRA Film-coated tablet Ref.[10362] Active ingredients: Omadacycline
Source: FDA, National Drug Code (US) Revision Year: 2020
12.1. Mechanism of Action
NUZYRA is an antibacterial drug [see Microbiology (12.4)].
12.2. Pharmacodynamics
Cardiac Electrophysiology
Based on the nonclinical and clinical data, including electrocardiogram evaluation in the phase 3 clinical trials, one of which had moxifloxacin as a control group, no clinically relevant QTc prolongation was observed at the maximum recommended dose of omadacycline.
Cardiac Physiology-Increase in Heart Rate
In phase 1 studies conducted in healthy volunteers, transient dose-dependent increases in heart rate have been observed following administration of single and multiple doses of omadacycline. The clinical implication of this finding is unknown [see Adverse Reactions (6.1)].
In a standard radiolabeled ligand binding assays, omadacycline was shown to inhibit binding of H-scopolamine to the M2 subtype of the muscarinic acetylcholine receptor. In the heart, muscarinic M2 receptors serve as mediators of the parasympathetic input that normally is received via the vagus nerve and stimulation of the receptor increases membrane potassium conductance through the acetylcholine-dependent channel, which slows depolarization and reduces pacemaker activity in the sinoatrial node.
12.3. Pharmacokinetics
The pharmacokinetic parameters of NUZYRA after single and multiple oral and intravenous doses are summarized in Table 6.
Table 6. Pharmacokinetic (PK) Parameters of NUZYRA in Healthy Adult Subjects:
| Dose and Route of Administration | 100 mg IV | 300 mg Oral | 450 mg Oral | |
|---|---|---|---|---|
| PK Parameters* | ||||
| Cmax (ng/mL) | Single dose | 1507 (38.6) | 548 (26.7) | 874 (26.6) |
| Steady state | 2120 (32.0) | 952 (44.2) | 1077 (25.0) | |
| AUC (h*ng/mL) | Single dose | 9358 (22.1) | 9399 (27.2) | 8977 (26.6) |
| Steady state | 12,140 (26.6) | 11,156 (44.9) | 13,367 (26.0) | |
| Dose Proportionality | Dose proportional increases in omadacycline Cmax and AUC following single oral doses of NUZYRA from 300 to 450 mg. | |||
| Accumulation | Accumulation ratio 1.5 | |||
| Absorption | ||||
| Bioavailability | 34.5% following single 300 mg dose of NUZYRA | |||
| Tmax Median (min, max) | Single dose | 0.55 (0.25, 0.68) | 2.50 (1, 4.05) | 2.50 (1.5, 3) |
| Steady state | 0.50 (0, 1) | 2.50 (0, 8) | 2.50 (1.5, 4) | |
| Distribution | ||||
| Plasma Protein Binding | 20%; not concentration dependent | |||
| Volume of Distribution (L) | Single dose | 256 (25.6) | 794 (23.6)† | ND |
| Steady state | 190 (27.7) | ND | ND | |
| Elimination | ||||
| Elimination Half-Life (hr) | Single dose | 16.2 (14.7) | 14.96 (16.5) | 13.45 (12.9) |
| Steady state | 16.0 (21.7) | 15.5 (10.7) | 16.83 (8.1) | |
| Systemic Clearance (L/hr) | Single dose | 11.24 (23.8) | 34.6 (30.9)† | ND |
| Steady state | 8.8 (25.2) | ND | ND | |
| Renal Clearance (L/hr) | 2.4 to 3.3 | |||
| Metabolism | Omadacycline is not metabolized | |||
| Excretion (Mean (SD) % dose) | Urine | 27 (3.5) % | 14.4 (2.3) %‡ | ND |
| Feces | ND | 81.1 (2.3) %‡ | ND | |
Cmax = maximum plasma concentration, AUC = area under concentration-time curve, IV = intravenous, ND = not determined, Tmax = time to Cmax
* All PK parameters presented as mean (% coefficient of variation; %CV) unless otherwise specified
† Presented as apparent clearance or volume of distribution
‡ Following administration of radiolabeled omadacycline
Absorption
The exposure to omadacycline is similar between a 300-mg oral dose and a 100-mg intravenous dose of NUZYRA in healthy fasted subjects.
Effect of Food
Ingestion of a standard high-fat nondairy meal (855 calories; 59% calories from fat) and standard high-fat meal including dairy (985 calories; 60% calories from fat) 2-hours before administration of a single 300-mg oral dose of NUZYRA decreased the rate (Cmax) and extent of absorption (AUC) by 40% and 42%, and 59% and 63%, respectively compared to administration of NUZYRA under fasting conditions. The rate and extent of absorption of NUZYRA were not substantially decreased when a high-fat nondairy meal (800-1000 calories; 50% calories from fat) was ingested 4 hours pre-dose.
Following ingestion of either a light non-fat (300-350 calories; ≤5% calories from fat), or a standard low-fat (800-1000 calories; 30% calories from fat), or a standard high fat (800-1000 calories; 50% calories from fat) meal 2 hours post-dose, the AUC and Cmax were not substantially altered, as compared to fasting conditions.
Distribution
Plasma protein binding of omadacycline is approximately 20% and is not concentration dependent. The mean (% CV) volume of distribution of omadacycline at steady-state following IV administration of NUZYRA in healthy subjects was 190 (27.7) L.
Elimination
Renal clearance of omadacycline following IV administration of NUZYRA ranged from 2.4 to 3.3 L/h in healthy subjects.
Metabolism
In vitro studies using human liver microsomes and hepatocytes demonstrated that omadacycline is not metabolized.
Excretion
Following a 100-mg IV dose of NUZYRA, 27% of the dose was recovered as unchanged omadacycline in the urine. In healthy male volunteers receiving 300-mg oral [14C] NUZYRA, 77.5% to 84.0% of the dose was recovered in the feces, approximately 14.4% (range 10.8% to 17.4%) in the urine, with 95.5% of the administered radioactive dose recovered after 7 days.
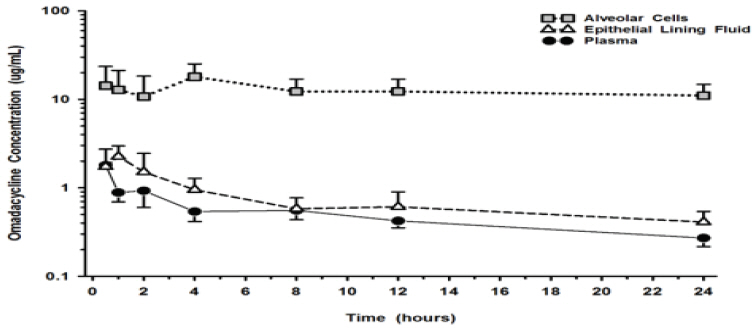
Lung Penetration
The mean omadacycline concentrations over time for alveolar cells (AC), epithelial lining fluid (ELF), and plasma following IV administration of multiple doses of 100-mg of NUZYRA to healthy volunteers are shown in Figure 1. The steady-state omadacycline AUC0-24h (302.5 hr*mcg/mL) in AC was 25.8-fold higher than the plasma AUC0-24h, and the AUC0-24h (17.2 hr*mcg/mL) in ELF was 1.5-fold higher than the AUC0-24h in plasma.
Figure 1. Mean (± SD) Concentrations of Omadacycline in Alveolar Cells, Epithelial Lining, and Plasma Following Multiple 100 mg IV Doses of NUZYRA to Healthy Subjects During Bronchoscopy Sampling Times:
Specific Populations
No clinically significant differences in the pharmacokinetics of omadacycline were observed based on age, gender, race, weight, renal impairment or end-stage renal disease, and hepatic impairment.
Patients with Renal Impairment
A study was conducted to compare NUZYRA pharmacokinetics following 100-mg IV administration in 8 subjects with end-stage renal disease (ESRD) on stable hemodialysis, with and 8-matched healthy control subjects. In the ESRD subjects, NUZYRA was administered on two separate occasions; immediately prior to dialysis and after dialysis, and the AUC, Cmax, and CL of NUZYRA were comparable between the renally impaired subjects and the matching healthy subjects. During dialysis, 7.9% of omadacycline was recovered in the dialysate. Renal impairment did not impact NUZYRA elimination.
Patients with Hepatic Impairment
A study was conducted to compare NUZYRA pharmacokinetics following intravenous and oral dosing to 5 subjects with mild hepatic impairment (Child-Pugh Class A), 6 subjects with moderate hepatic impairment (Child-Pugh Class B), and 6 subjects with severe hepatic impairment (Child-Pugh Class C) as compared to 12 matched healthy control subjects. The AUC and Cmax of NUZYRA were comparable between the hepatically impaired subjects and the matching healthy subjects, and similar clearance was observed across all cohorts. Hepatic impairment did not impact NUZYRA elimination.
Drug Interaction Studies
Clinical Studies
Administration of oral verapamil (P-gp inhibitor) two hours prior to a single 300 mg oral dose of NUZYRA increased omadacycline AUC by approximately 25% and Cmax by approximately 9%.
In vitro Studies
In vitro studies in human liver microsomes indicate that omadacycline does not inhibit nor induce metabolism mediated by CYP 1A1, 1A2, 2A6, 2B6, 2C8, 2C9, 2C19, 2D6, and 3A4/5, or UGT1A1. Therefore, NUZYRA is not expected to alter the pharmacokinetics of drugs metabolized by the above stated human hepatic enzymes.
Omadacycline is not an inhibitor of P-gp and organic anion transporting polypeptide (OATP) 1B1 and OATP1B3. Omadacycline is a substrate of P-gp (see Clinical Studies above). Omadacycline is not a substrate or inhibitor of the major organic anion transporters (OAT-1 and 3), breast cancer resistance protein (BCRP), or multidrug resistance-associated protein 2 (MRP2). Omadacycline was not an OATP1B1 or OATP1B3 substrate at supra-therapeutic concentrations (5-13 fold higher than clinically relevant concentrations).
12.4. Microbiology
Mechanism of Action
Omadacycline is an aminomethylcycline antibacterial within the tetracycline class of antibacterial drugs. Omadacycline binds to the 30S ribosomal subunit and blocks protein synthesis. In general, omadacycline is considered bacteriostatic; however, omadacycline has demonstrated bactericidal activity against some isolates of S. pneumoniae and H. influenzae.
Resistance
The following in vitro data are available, but their clinical significance is unknown. Omadacycline was active in vitro against Gram-positive bacteria expressing ribosomal protection proteins (TetM) and tetracycline resistance active efflux pumps (TetK and TetL), and in Enterobactericeae expressing the TetB efflux pump. Additionally, omadacycline was active against some S. aureus, S. pneumoniae, and H. influenzae strains carrying macrolide resistance genes (ermA, B and/or C), or ciprofloxacin resistance genes (gyrA and parC) and beta-lactamase positive H. influenzae.
Interaction with Other Antimicrobials
In vitro studies have not demonstrated antagonism between omadacycline and other commonly used antibacterials (ampicillin, ceftazidime, ceftriaxone, imipenem, piperacillin/tazobactam, gentamicin, vancomycin, daptomycin, linezolid).
Antimicrobial Activity
Omadacycline has been shown to be active against most isolates of the following bacteria, both in vitro and in clinical infections [see Indications and Usage (1.1, 1.2)].
Community-Acquired Bacterial Pneumonia (CABP)
Gram-positive bacteria:
Streptococcus pneumoniae
Staphylococcus aureus (methicillin-susceptible isolates)
Gram-negative bacteria:
Haemophilus influenzae
Haemophilus parainfluenzae
Klebsiella pneumoniae
Other microorganisms:
Chlamydophila pneumoniae
Legionella pneumophila
Mycoplasma pneumoniae
Acute Bacterial Skin and Skin Structure Infections (ABSSSI)
Gram-positive bacteria:
Enterococcus faecalis
Staphylococcus aureus (methicillin-susceptible and -resistant isolates)
Staphylococcus lugdunensis
Streptococcus anginosus grp. (includes S. anginosus, S. intermedius, and S. constellatus)
Streptococcus pyogenes
Gram-negative bacteria:
Enterobacter cloacae
Klebsiella pneumoniae
The following in vitro data are available, but their clinical significance is unknown. At least 90% of isolates of the following bacteria exhibit an in-vitro minimum inhibitory concentration (MIC) less than or equal to the susceptible breakpoint for NUZYRA against isolates of similar genus or organism group. However, the efficacy of NUZYRA in treating clinical infections due to these bacteria has not been established in adequate and well controlled clinical trials.
Gram-positive bacteria:
Enterococcus faecium (vancomycin-susceptible and -resistant isolates)
Streptococcus agalactiae
Gram-negative bacteria:
Enterobacter aerogenes
Escherichia coli
Citrobacter freundii
Citrobacter koseri
Klebsiella oxytoca
Moraxella catarrhalis
Susceptibility Testing
For specific information regarding susceptibility test interpretive criteria and associated test methods and quality control standards recognized by FDA for this drug, please see: https://www.fda.gov/STIC.
13.1. Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
Carcinogenicity studies with omadacycline have not been conducted. However, there has been evidence of oncogenic activity in rats in studies with the related antibacterial drugs, oxytetracycline (adrenal and pituitary tumors), and minocycline (thyroid tumors).
Mutagenesis
Omadacycline was positive for clastogenicity and aneugenicity in an in vitro chromosome aberration assay in Chinese hamster ovary (CHO) cells and for mutagenicity in an in vitro forward mutation assay in mouse lymphoma cells. These effects were seen in the presence of metabolizing enzymes.
Omadacycline was negative in a chromosomal aberration test in Chinese hamster V79 cells and in vivo micronucleus assays administered intraperitoneally to ICR mice or intravenously to HanRcc: WIST rats.
Impairment of Fertility
Omadacycline administration to male rats in a fertility study caused reduced sperm counts and sperm motility at 20-mg/kg/day (approximately 1.3 times clinical systemic exposure, based on AUC in a separate study in rats at a similar dose), but had no effect on male fertility parameters. In general toxicity studies, inhibition of spermatogenesis occurred after administration of 45-mg/kg/day omadacycline (6 to 8 times the clinical AUC exposure) for 37 days or longer, but not at lower doses (15-mg/kg/day, ≤2 times clinical AUC exposure) or shorter treatment periods (4 weeks or less). In female rats, fertility was reduced at the 20-mg/kg/day dose (approximately equivalent to human exposures in a separate study in unmated females), characterized by reduced ovulation and increased embryonic loss when treatment occurred from before mating through early pregnancy.
13.2. Animal Toxicology and/or Pharmacology
Hyperpigmentation of the thyroid has been produced by members of the tetracycline class in the following species: in rats by omadacycline, oxytetracycline, doxycycline, tetracycline PO4, and methacycline; in minipigs by doxycycline, minocycline, tetracycline PO4, and methacycline; in dogs by doxycycline and minocycline; in monkeys by omadacycline and minocycline.
Minocycline, tetracycline PO4, methacycline, doxycycline, tetracycline base, oxytetracycline HCl, and tetracycline HCl were goitrogenic in rats fed a low iodine diet. This goitrogenic effect was accompanied by high radioactive iodine uptake. Administration of minocycline also produced a large goiter with high radioiodine uptake in rats fed a relatively high iodine diet.
Treatment of various animal species with this class of drugs has also resulted in the induction of thyroid hyperplasia in the following: in rats and dogs (minocycline); in chickens (chlortetracycline); and in rats and mice (oxytetracycline). Adrenal gland hyperplasia has been observed in goats and rats treated with oxytetracycline.
14. Clinical Studies
14.1 Community-Acquired Bacterial Pneumonia
A total of 774 adults with CABP were randomized in a multinational, double-blind, double-dummy trial (Trial 1, NCT #02531438) comparing NUZYRA to moxifloxacin. NUZYRA was administered 100-mg intravenously every 12 hours for two doses on Day 1, followed by 100-mg intravenously daily, or 300-mg orally, daily. Moxifloxacin 400-mg was administered intravenously or orally daily. Total treatment duration was 7-14 days. All enrolled patients were expected to require a minimum of at least 3 days of intravenous treatment. Efficacy and safety of an oral loading dose was not evaluated in CABP.
A total of 386 patients were randomized to NUZYRA and 388 patients were randomized to moxifloxacin. Patient demographic and baseline characteristics were balanced between the treatment groups. Patients were predominantly male (55%) and white (92%). Approximately 60% of patients in each group belonged to PORT Risk Class III, 26% were PORT Risk Class IV and 14.5% were PORT Risk Class II. The median age was 62 years, mean BMI was 27.34 kg/m², and approximately 47% of NUZYRA treated patients had CrCl <90 ml/min. Among NUZYRA-treated patients, common comorbid conditions included hypertension (49.5%), diabetes mellitus (16.3%), chronic lung disease (21.2%), atrial fibrillation (10.1%), and coronary artery disease (9.1%). The majority of sites were in Eastern Europe, which accounted for 82% of enrollment; 3 patients were enrolled in the US.
Clinical success at the early clinical response (ECR) timepoint, 72 to 120 hours after the first dose, was defined as survival with improvement in at least two of four symptoms (cough, sputum production, chest pain, dyspnea) without deterioration in any of these four symptoms in the intent to treat population (ITT), which consisted of all randomized patients.
Table 7 presents the clinical success rates at the ECR timepoint (ITT population).
Table 7. Clinical Success* at the ECR Timepoint in Trial 1 (ITT Population):
| Endpoint | NUZYRA (%) | Moxifloxacin (%) | Treatment Difference (95% CI†) |
|---|---|---|---|
| Clinical Success | 81.1% | 82.7% | -1.6 (-7.1, 3.8) |
* Clinical Success at the early clinical response (ECR) timepoint, 72 to 120 hours after the first dose, was defined as survival with improvement in at least two of four symptoms (cough, sputum production, chest pain, dyspnea) from baseline without deterioration in any of these symptoms, with no receipt of antibacterial treatment either as a rescue for CABP or as a treatment for other infections that may be effective for CABP, and no discontinuation of study treatment due to AE.
† 95% confidence interval for the treatment difference
Clinical response was also assessed by the investigator at the post therapy evaluation visit (PTE), 5 to 10 days after last dose of study drug and defined as survival and improvement in signs and symptoms of CABP, based on the clinician’s judgment, to the extent that further antibacterial therapy is not necessary. Table 8 presents the results of clinical response at the PTE visit for both the ITT population and the Clinically Evaluable (CE) population, which consisted of all ITT patients who had a diagnosis of CABP, received a minimum number of expected doses of study drug, did not have any protocol deviations that would affect the assessment of efficacy, and had investigator assessment at the PTE visit. Clinical response rates by most common baseline pathogen in the microbiological ITT (micro-ITT) population, defined as all randomized patients with a baseline pathogen are presented in Table 9.
Table 8. Investigator’s Overall Assessment of Clinical Response at PTE* in Trial 1 (ITT and CE Population):
| Endpoint | Population | NUZYRA n/N (%) | Moxifloxacin n/N (%) | Treatment Difference (95% CI†) |
|---|---|---|---|---|
| Clinical Success at PTE | ITT | 338/386 (87.6) | 330/388 (85.1) | 2.5 (-2.4, 7.4) |
| Clinical Success at PTE | CE | 316/340 (92.9) | 312/345 (90.4) | 2.5 (-1.7, 6.8) |
* Investigator’s overall assessment of clinical response at PTE was defined as survival and improvement in signs and symptoms of CABP, based on the clinician’s judgment, to the extent that further antibacterial therapy is not necessary in the ITT and CE populations.
† 95% confidence interval for the treatment difference.
Table 9. Investigator’s Overall Assessment of Clinical Response at PTE by Baseline Pathogen in Trial 1 (micro-ITT population):
| Pathogen | NUZYRA n/N (%) | Moxifloxacin n/N (%) |
|---|---|---|
| Streptococcus pneumoniae | 37/43 (86.0) | 31/34 (91.2) |
| Methicillin-susceptible Staphylococcus aureus (MSSA) | 8/11 (72.7) | 8/10 (80.0) |
| Haemophilus influenzae | 26/32 (81.3) | 16/16 (100) |
| Haemophilus parainfluenzae | 15/18 (83.3) | 13/17 (76.5) |
| Klebsiella pneumoniae | 10/13 (76.9) | 11/13 (84.6) |
| Legionella pneumophila | 27/29 (93.1) | 27/28 (96.4) |
| Mycoplasma pneumoniae | 31/35 (88.6) | 25/29 (86.2) |
| Chlamydophila pneumoniae | 14/15 (93.3) | 13/14 (92.9) |
14.2 Acute Bacterial Skin and Skin Structure Infections
A total of 1390 adults with ABSSSI were randomized in two multicenter, multinational, double-blind, double-dummy trials (Trial 2 NCT #02378480 and Trial 3 NCT #02877927). Both trials compared 7 to 14 days of NUZYRA to linezolid. Patients with cellulitis, major abscess, or wound infection were enrolled in the trials.
In Trial 2, 329 patients were randomized to NUZYRA (100-mg intravenously every 12 hours for 2 doses followed by 100-mg intravenously every 24 hours, with the option to switch to 300-mg orally every 24 hours) and 326 patients were randomized to linezolid (600-mg intravenously every 12 hours, with the option to switch to 600-mg orally every 12 hours). Patients in the trial had the following infections: cellulitis (38%), wound infection (33%) and major abscess (29%). The mean surface area of the infected lesion was 455 cm² in NUZYRA-treated patients and 498 cm² in linezolid-treated patients. The mean age of patients was 47 years. Subjects were predominantly male (65%) and white (92%), and mean BMI was 28.1 kg/m². Among NUZYRA-treated patients, common comorbid conditions included drug abuse (53.9%), hepatitis C (29.1%), hypertension (20.4%), anxiety (19.5%), and depression (15.5%). Trial 2 was conducted globally including approximately 60% of patients enrolled in the United States.
In Trial 3, 368 patients were randomized to NUZYRA (450-mg oral once a day on Days 1 and 2, followed by 300-mg orally once a day) and 367 were randomized to linezolid (600-mg orally every 12 hours). All patients were enrolled in the United States. Patients in the trial had the following infections: wound infections (58%), cellulitis (24%), and major abscess (18%). The mean surface area of the infected lesion was 424 cm² in NUZYRA-treated patients and 399 cm² in linezolid-treated patients. The mean age of patients was 44 years. Subjects were predominantly male (63%) and white (91%) and mean BMI was 27.9 kg/m². The most common comorbid conditions included drug abuse (72.8%), tobacco use (12.0%), and chronic hepatitis C infection (31.5%).
In Trials 2 and 3, approximately 12% of NUZYRA treated patients had CrCl <90 ml/min.
In both trials, efficacy was determined by the successful early clinical response at 48 to 72 hours after the first dose in the mITT population and was defined as a 20% or greater decrease in lesion size. Table 10 summarizes the clinical response rates in the two trials. The mITT population was defined as all randomized subjects without a sole Gram-negative causative pathogen at screening.
Table 10. Clinical Success* at the ECR Timepoint in the mITT Population in Trial 2 and Trial 3:
| Study | NUZYRA (%) | Linezolid (%) | Treatment Difference (Two-Sided 95% CI)† |
|---|---|---|---|
| Trial 2 | 84.8 | 85.5 | -0.7 (-6.3, 4.9) |
| Trial 3 | 87.3 | 82.2 | +5.1 (-0.2, 10.5) |
* Clinical success at early clinical response (ECR) at 4 8 to 72 hours after the first dose, was defined as a 20% or greater decrease in lesion size without any reasons for failure (less than 20% reduction in lesion size, administration of rescue antibacterial therapy, use of another antibacterial or surgical procedure to treat for lack of efficacy, or death).
† 95% confidence interval for the treatment difference.
Clinical response at the post therapy evaluation (PTE, 7 to 14 days after last dose) visit in the mITT and clinically evaluable (CE) populations was defined as survival after completion of study treatment without receiving any alternative antibacterial therapy other than NUZYRA, without unplanned major surgical intervention, and sufficient resolution of infection such that further antibacterial therapy is not needed (see Table 11). Clinical response rates at PTE by most common pathogen in the microbiological-mITT population, defined as all patients in the mITT population, who had at least 1 Gram-positive causative pathogen identified at baseline are provided in Table 12. The CE population consisted of all mITT patients who had a diagnosis of ABSSSI, received a minimum number of expected doses of study drug, did not have any protocol deviations that would affect the assessment of efficacy, and had investigator assessment at the PTE Visit.
Table 11. Investigator’s Overall Assessment of Clinical Response at PTE in mITT and CE Population in Trial 2 and Trial 3:
| Study | Population | NUZYRA n/N (%) | Linezolid n/N (%) | Treatment Difference (Two-Sided 95% CI)* |
|---|---|---|---|---|
| Trial 2 | mITT | 272/316 (86.1) | 260/311 (83.6) | +2.5 (-3.2, 8.2) |
| CE | 259/269 (96.3) | 243/260 (93.5) | +2.8 (-1.0, 6.9) | |
| Trial 3 | mITT | 296/353 (83.9) | 284/353 (80.5) | +3.4 (-2.3, 9.1) |
| CE | 272/278 (97.8) | 272/285 (95.4) | +2.4 (-0.6, 5.8) |
* 95% confidence interval for the treatment difference.
Table 12. Investigator’s Overall Assessment of Clinical Response at PTE by Baseline Pathogen in Trials 2 and 3 (micro-mITT population):
| Pathogen | NUZYRA n/N (%) | Linezolid n/N (%) |
|---|---|---|
| Staphylococcus aureus | 305/369 (82.7) | 306/378 (81.0) |
| Methicillin-susceptible Staphylococcus aureus (MSSA) | 164/201 (81.6) | 181/226 (80.1) |
| Methicillin-resistant Staphylococcus aureus (MRSA) | 146/173 (84.4) | 128/157 (81.5) |
| Staphylococcus lugdunensis | 10/11 (90.9) | ⅔ (66.7) |
| Streptococcus anginosus group | 84/104 (80.8) | 59/82 (72.0) |
| Streptococcus pyogenes | 28/40 (70.0) | 25/34 (73.5) |
| Enterococcus faecalis | 17/18 (94.4) | 21/25 (84.0) |
| Enterobacter cloacae | 11/14 (78.6) | 9/11 (81.8) |
| Klebsiella pneumoniae | 8/11 (72.7) | 6/11 (54.5) |
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.